Article Text

Abstract
Background This study assessed the psychosocial determinants as explanatory variables for the length of the work disability period. The aim was to estimate the predictive value of a selected set of psychosocial determinants from the Quickscan questionnaire for the length of the sick leave period. A comparison was also made with the most common biomedical determinant: diagnosis.
Methods In a cohort study of 4 981 insured Belgian patients, the length of the sick leave was calculated using Kaplan–Meier. Predictive psychosocial determinants were selected using backward conditional selection in Cox regression and using concordance index values (C-index) we compared the predictive value of the biomedical to the psychosocial model in a sample subset.
Results Fourteen psychosocial determinants were significantly (p<0.10) related to the length of the sick leave: health perception of the patient, physical workload, social support management, social support colleagues, work–health interference, psychological distress, fear of colleagues’ expectations, stressful life-events, autonomy, learning and development opportunities, job satisfaction, workload, work expectations and expectation to return to work. The C-index of this biopsychosocial model including gender, age and labour status was 0.80 (CI: 0.78; 0.81) (n=4 981). In the subset of 2 868 respondents with diagnostic information, the C-index for the same model was .73 (CI: 0.71; 0.76) compared with 0.63 (CI: 0.61; 0.65) for the biomedical model.
Conclusions A set of 14 psychosocial determinants showed good predictive capacity (C-index: 0.80). Also, in a subset of the sample, the selected determinants performed better compared with diagnostic information to predict long-term sick leave (>6 months).
- Disability
- epidemiology
- public health
- health services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Long-term sickness absence (>6 months) is a growing problem in Europe. In 2012, the percentage of sick leave spending was 0.97% of the GDP in the EU-28 and, since 2008 (0.88%), the long-term trend has been slightly increasing.1 In Belgium, there were over 400 000 patients on long-term sick leave (>1 year of work disability) in 2018. In 2009, this group numbered only 245 209 patients.2 Musculoskeletal diseases and mental health problems are the most prevalent conditions for long-term sick leave.3
Mainly biomedical models are implemented in Europe and North America to determine the permitted duration of sickness absence based on diagnostic information of the patient.4 However, many of these guidelines happen to be based on pragmatic expert consensus or non-systematic literature reviews; their effectiveness has not yet been formally evaluated.4
In addition, there is evidence in the literature that other factors (such as psychosocial and environmental) play a determining role in the duration of sickness absence.5 Therefore, purely biomedical models to explain sickness absence have been criticised. The assumption that a specific disease underlies all illnesses has led to the medicalisation of illness.6 Further, most biomedical models are strongly linked to primitive forms of intuitive mind–body dualism. Return to work (RTW) depends not only on disease but also on the nature and circumstances of the work, personal (eg, age, education, gender), cultural and organisational factors, including accessibility and quality of healthcare delivery.7 All these determinants may justify the critique on guidelines that include statements on the expected length of sickness absence based on biomedical determinants only.4 As previously confirmed, the longer the duration of the absence, the less likely the cause of the absence is related to the initial medical diagnosis.8 Therefore, in some countries, biopsychosocial models, which includes social and economic factors, have been introduced.6 The International Classification of Functioning, disability and health model is an example of this trend. Although the biopsychosocial model is increasingly accepted, separate services sometimes exist for patients with physical disability and for those with mental health problems.6
The current study aimed to prove that a selected set of psychosocial determinants from the Quickscan questionnaire can discriminate patients for their risk on long-term sickness absence. A second aim is to compare the discriminative ability with the common biomedical determinant: diagnosis.
METHODS
Design and sample
We conducted a register-based cohort study using psychosocial determinants and disability-related data from the disability register of sickness fund organisations. Psychosocial determinants are collected by sickness fund organisations, in compliance with the legislation,I which requires the collection of psychosocial data in sick-listed individuals. Other data (eg, diagnosis, sociodemographic variables) were extracted via the patients’ file within the sickness fund organisations.
We included socially insured Belgian citizens who entered the seventh week of sickness absence for any reason between August 21 and December 3, 2017, excluding civil servants and self-employed individuals, who have different social insurance systems in Belgium. The eligibility criteria for receiving disability benefits are the same for employees and unemployed patients. The major evaluation criterion is having a reduced earning capacity of more than 66% due to new or worsening of functional disorders. When unemployed patients are no longer eligible, they will receive again unemployment benefits. The selected cohort was followed at least 341 days after the start of their sick leave period. The sickness fund organisations provided this follow-up data. Data extraction was executed on November 9, 2018.
Response versus non-response groups were compared with each other based on gender, age, diagnosis and time until the end of the disability period, because only this information was available for both groups. More detail about the non-response analysis and a socio-demographic analysis of both groups can be found in online additional file 1.
Supplemental material
Ethical approval was obtained from the Ethics Committee of the University Hospitals KU Leuven (S61255) on April 6, 2018. The coded data were transferred via the server of the Intermutualistic Agency, a coordination organisation of all Belgian sickness fund organisations. Secure access was provided to the researchers after login with Electronic Identity (eID).
The inclusion criterion for participation in the study was sick leave for 6 weeks due to a disease or private accident. The exclusion criteria were being self-employed and being a civil servant or non-consecutive leave. A recommenced disability within 14 days of the previous disability would be regarded as part of the same sickness period, after 14 days, a recommenced disability would be regarded as a new case. In total, 23 672 patients met the inclusion criteria during the inclusion period of 6 weeks. Of them, 5 235 (22.1%) provided a completed Quickscan questionnaire to sickness fund organisations. After data cleaning, 4 981 cases were retained. An overview of the data cleaning procedure can be found in online additional file 2.
Supplemental material
As ICD-10 coding, related to diagnostic information, is only mandatory starting from the seventh month of disability, ICD-10 coding was available for only 57.6% or 2 868 patients of the final database. The descriptive information of this subset of data is compared with the whole database in online additional file 3.
Supplemental material
Variables and instruments
Sickness fund organisations use the digital self-administered Quickscan questionnaire to measure psychosocial determinants.9 Quickscan is a generic questionnaire aimed at the entire population of sick-listed individuals after 6 weeks of paid sick leave9 and consist of 61 items loaded on 21 psychosocial factors (see online additional file 4).10 The questions can be categorised into four over-arching categories: work-related factors, functioning factors, person-related factors and stressful life events.10 When answering the work-related questions, the respondents are asked to think about their current job. Respondents who were unemployed when filling out the questionnaire were asked to think about their previous employment.
Supplemental material
Each question is scored on a 6-point likert scale (0–5) and is individually entered in the model.
Other variables extracted for this study were sociodemographic characteristics, such as gender, labour status (employed/unemployed) and age (year of birth). These variables were extracted from the patients’ files at the sickness fund organisations. The age variable was based on the date of birth and was further categorised into five groups: <25, 26–35, 36–45, 46–55 and 55+ years.
Diagnostic information was extracted for patients for whom a pathology code (ICD-10) was available.
The outcome variable was a disability period >6 months, which was derived from the length of the disability period (calculated in days using the start date of the disability and the end date of the work disability, as registered by the sickness fund organisations).
Statistical analysis
First, we derived all descriptive information on the independent variables (ie, psychosocial determinants, demographic variables, diagnosis) and outcome variable (ie, length of the sick leave period). Kaplan–Meier estimates were used to visualise the duration of the sick leave. Log-rank tests were applied to test for differences in length of work disability between different subgroups in our sample (eg, gender, age, labour status, diagnosis).
Second, we used Cox regression, with backward conditional selection, to remove non-significant factors (p<0.10), thereby reducing the number of items in our model. Age, gender and labour status were included in the model by default and could not be excluded during the selection process.
Third, the area under the curve (AUC) was calculated based on the linear predictor of the selected factors from the cox model (including gender, age and labour status). A 6-month cut-off was chosen since this is the moment when Belgian patients’ capacities are assessed regarding the entire labour market and not solely their previous job.
On a subset of the data (n=2 868), the predictive performance of the same Cox model with the psychosocial determinants was compared with the performance of a model containing gender, age, labour status and diagnosis (referred to the biomedical model in the remainder). To estimate the biomedical model, we condensed the number of ICD-10 categories into six large categories. The five most prevalent ICD-10 categories of our sample were retained (neoplasms; mental and behavioural disorders; diseases of the musculoskeletal system and connective tissues; injury, poisoning and certain other consequences of external causes; factors influencing health status and contact with health services (eg, alcohol abuse counselling)) and a sixth category included all ‘others’.
We evaluated the predictive performance of the final parsimonious models (including gender age and labour status) using Harrell’s concordance index (C-index). The C-index is equal to the AUC and has a range from 0.5 (no discriminatory ability) to 1 (maximum discriminatory ability). C-index under 0.7 represents poor, 0.7–0.8 good, and >0.8 strong discriminating ability.11
The predictive performance was externally validated using data from an independent population-based cohort of 5 160 sick-listed patients.
RESULTS
Description of the study population
The mean age of the participants in both the main sample (n=4 981) and the subsample (n=2 868) was 44 years. The age category 46–55 years had the largest proportion of patients, whereas the category <25 years had the smallest proportion in both the whole and subsample.
There were more women compared with men in both samples. Most patients were under contract, whereas others were unemployed. In Belgium, most citizens speak either French (Southern part) or Dutch (Northern part); in both samples, the majority of patients were Dutch speaking.
For a subset of 2 868 patients in our sample (57.6%), diagnostic information was available. The largest group reported experiencing diseases of the musculoskeletal system and connective tissues (33.7%), and the second largest group experienced mental and behavioural disorders (21.8%). Because reporting ICD-10 coding is mandatory from the 7th month of sick leave, this subgroup had much higher sick leave durations compared with the whole sample (median 280 days (n=2 868 vs 145 days in the whole sample (n=4 981)).
For both patients who were still under contract and who were unemployed, the end of the work disability period meant that they resumed work or they were (back) on unemployment benefits. Actual work resumption was thus not guaranteed after the end of the work disability period. The Kaplan–Meier curves for both the whole sample and the subsample are given in figure 1.
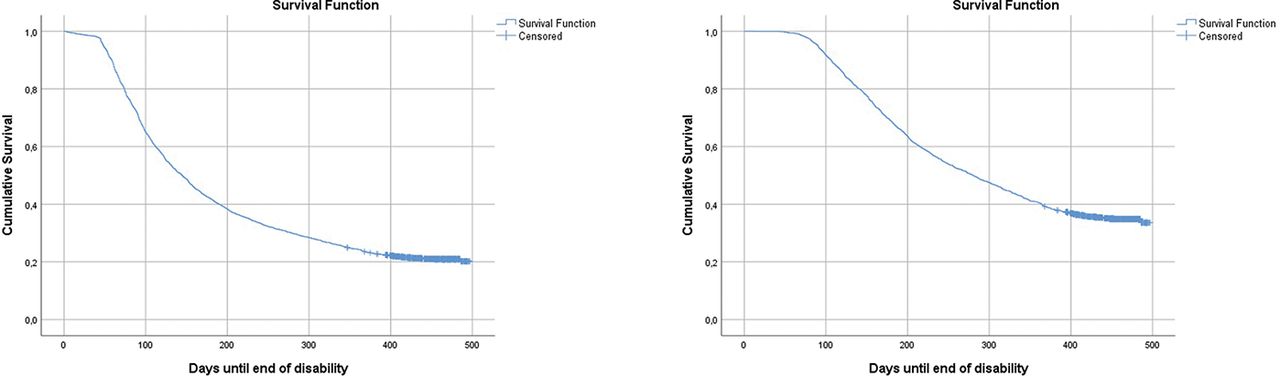
Survival function (cumulative survival probability) for the whole sample n=4 981(left) and the subsample (n=2 868) (right).
Results of univariate analyses are given in online additional file 3. Men received significantly shorter (p<0.001) periods of time disability benefits compared with women in the whole sample (p=0.001 in the subsample). In addition, younger age groups received significantly less benefits (p<0.001) compared with older age groups in both the whole and the subsample. Patients who were under contract ended their disability period significantly faster (p<0.001) compared with patients who were unemployed in both the whole and the subsample.
Based on diagnosis, significant differences (p<0.001) were observed between the six largest pathology groups. Patients with cancer received disability benefits for the longest period (no median available), whereas the group with ‘Injury, poisoning, and certain other consequences of external causes’ had the shortest period covered by benefits (median 183 days).
Multivariable models
The significant psychosocial factors were selected using backward conditional selection in Cox regression in the whole sample (n=4 981). Figure 2 shows the significant factors visualised with the number of items retained in the measurement model (Quickscan).

Significant psychosocial determinants for sick leave duration.
Along with age, gender, and labour status, 18 items from 14 psychosocial factors were significantly retained in the prediction model (p<0.10): health perception of the patient, physical workload, social support management, social support colleagues, work–health interference, psychological distress, fear of colleagues’ expectations, stressful life events, autonomy, learning and development opportunities, job satisfaction, workload, work expectations and expectation to RTW. For some factors, more than one item was retained. The selected factors and their significance can be found in online additional file 5.
Supplemental material
For the functioning factors, we found that the better the perceived health and the more the patients believed they would RTW soon, the faster the disability period ended. Meanwhile, the greater the distress and the patients’ believe that work would interfere with their recovery, the more time it took to end the disability period.
For the work-related factors, we found that the greater the physical workload, workload, and pessimism about the work expectations, the longer the disability period. Meanwhile, the more job satisfaction, support by colleagues and by the employer, perceived autonomy at work, and learning and development opportunities, the shorter the disability period.
For the person-related factors, the more fear individuals had regarding the expectations of their colleagues, the slower the RTW process.
Finally, all stressful life event-related factors were negatively related to the outcome, and therefore, the increased stress or discomfort in their home situation would lead to increased time needed to end the disability period.
The predictive value of the psychosocial determinants was evaluated based on the linear predictor of the 14 selected factors from the cox model, gender, age and labour status. The dependent variable state was the binary variable of being sick for more than 6 months. The ROC curve yielded an AUC value of 0.80 (CI: 0.78; 0.81). The ROC curve is plotted in figure 3. The diagonal indicates the baseline, for a non-discriminating model. The curved line marks the performance area of the model. Using the same linear predictor as for the whole sample, in the subsample of 2 868 cases, the AUC value of the psychosocial model in this sample was 0.73 (CI: 0.71; 0.76). To compare this result to the usual assessment in insurance medicine, we plotted a ROC curve using the linear predictor of the model with sex, age and labour status and the diagnosis as independent variables for the ROC plotting. This resulted in AUC 0.63 (CI: 0.61; 0.65). Both curves are plotted in figure 4. Thus, based on diagnosis, labour status, age and gender, and in this subgroup, the predictive value is much weaker compared with using the psychosocial determinants.

ROC for 14 significant psychosocial determinants (p<0.10), AUC value: 0.80 (CI: 0.78; 0.81). AUC, area under the curve.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left: ROC psychosocial determinants, gender age and labour status AUC value: 0.73 (CI: 0.71; 0.76) (n=2 868). Right: ROC biomedical model (ICD-10 (six largest pathology groups), gender, age and labour status) AUC value: 0.63 (CI: 0.608; 0.654) (n=2 868). AUC, area under the curve.
External validation was executed on cohort data that was collected in the same way between 17/09/2018 and 04/11/2018. The AUC value of the psychosocial model in this sample (n=5 160) was 0.75 (CI: 0.73; 0.76). In the subsample of 3 451 cases for which diagnostic information was available, the C-index for the biopsychosocial model was 0.74 (CI: 0.72; 0.76), compared with 0.66 (CI: 0.64; 0.68) for the model with sex, age, labour status and diagnosis.
DISCUSSION
This study aimed to identify the psychosocial determinants that influence the duration of work disability among socially insured patients in Belgium. We found 14 psychosocial determinants that were significantly (p<0.10) related to the time until the end of the sick leave period. This model had a predictive value for long-term sickness absence (>6 months) of 80% (C-index), which indicates good to strong discriminative ability. The external validation of the model still indicated good discriminative ability (75%).
Most of our 14 factors are supported in the literature.12 We found 10 work related-factors; previous researchers have discussed physical work demands as a burden for returning to work.12–16 Den Boer et al also discussed job satisfaction in the case of work capacity at 6-month post-surgery.13 Kausto et al, Netterstrom and Marhold et al discussed the support by colleagues and by employers as important facilitators for returning to work.14 15 17 Meanwhile, Airaksinen did not find evidence for any of the work-related factors in their study after including lifestyle and demographic characteristics.18
We found one person-related factor: fear of colleagues’ expectations. This seems a factor related to ‘fear avoidance beliefs’, which is included as an important prognostic factor for participation in patients with sciatica.12 Steenstra et al found insufficient evidence for fear avoidance beliefs in later phases for patients with low back pain.16
Pain-related factors were not retained as a predictor for long-term sickness absence in our model, in contrast to Marhold et al, who found this factor to be related to sickness absence longer than 9 months.17 Pain coping has also been identified as a prognostic factor for participation in patients with sciatica.12 In our research, the population included patients with mental disorders, which might be the reason for the pain variables to be non-significant. Hence, patients with mental disorders often do not consistently identify their complaints as pain related.
Our psychological distress factor strongly related to the depression scale in the study of Marhold et al, which found depression to be strongly related to long-term sickness absence (<9 months). Depression and mental stress are also important for returning to work within 2 years according to Schade et al.19 Multiple studies found, as in our study, perceptions and beliefs about work and returning to work to be a significant hindrance for actual recovery.16 17 Steenstra et al report that workers’ recovery expectations remain important after 6 weeks for patients with low back pain.16 The general health factor is important according to two different studies in a systematic review.12
Netterstrom et al describe stressful negative life events during the year before baseline as a risk factor for no RTW after 1 year, among patients on sick leave due to occupational stress,15 which is very similar to our findings in the current study with all patients on sick leave.
Demographic factors were included in our model to correct for possible non-response bias. Gender and age were found to be significant, consistent with many studies in a systematic review.12 Lederer et al reported gender differences in the effect of personal and work-related psychosocial, physical and organisational determinants on time to RTW. They report similar survival curves for long-term disability for both genders, but they also found that many personal and occupational factors influencing RTW differed by gender. They plead for a gender-sensitive strategy to investigate RTW determinants.20
Labour status was found to be significant when tested as a univariate variable (see online additional file 3). This is in line with the idea that unemployed are less likely to have good health compared with the employed, indicating lower probabilities of RTW.21 However, labour status was no longer significant (p=0.28) when controlling for other biopsychosocial determinants. This means that the effect of labour status disappears when adding other psychosocial determinants. According to Allebeck et al, little is known about these underlying causes.22
For the biomedical model, we found a univariate significant difference (log-rank test) between the six pathology groups. However, when testing the predictive value of the diagnosis model, the model seemed rather weak with a C-index of 0.63 (66 external validation) compared with the psychosocial model with a C-index of 0.73 (0.74 external validation). Consequently, we could conclude that general patterns can be drawn for some diseases (eg, cancer patients will need more time to resume working), but on an individual level, these patterns are not significant to predict the risk for long-term sickness absence. This is a critical finding that supports the holistic view on sickness absence and that undermines the idea of a solely biological approach to reintegration. Since the model was only tested for a subgroup of our sample, who, in general, were absent for a longer amount of time (median 280 days), and who were probably a more homogeneous population, we must be careful with generalisability of the results.
However, we can conclude that ICD-10 coding was less predictive for the risk on long-term sick leave than our set of psychosocial determinants.
Strengths, limitations, and need for future research
The most important strength of our study is that it was executed on data from sickness fund organisations all over Belgium. The large samples and the external validation support the evidence of our findings.
A shortcoming of this study is the possibility of non-response bias. Taking into account unclarity about the factors related to the non-response, we did not correct for this possible bias. If there would be a bias, the questionnaire can still be applied to the subpopulation who is more responsive to this kind of questionnaires and who might be more cooperative to future RTW interventions.
Also, the lack of diagnostic information about a large part of the sample, makes it difficult to generalise the results of the diagnostic model towards the whole population. In this paper, we therefore made the comparison between the biopsychosocial model and the biomedical model only for the subsample in which this information was available.
In addition, questioning patients during their sickness period is sensitive and might induce fear of being forced to RTW. To limit this risk, we stressed that completing the questionnaire would not have consequences for their disability status. Because the questionnaire is self-administered, the patient might feel safer to answer honestly while being in the environment of his own home.
Finally, we only measured the outcome of the end of disability in the current study. We do not have data about actual work resumption or the number of patients that would receive unemployment benefits after their disability period. We also did not measure other possible outcomes, such as retirement or death, and the sustainability of the rehabilitation.
CONCLUDING REMARKS
Apart from its predictive capacity for long-term disability, the biopsychosocial model has another advantage: psychosocial determinants are subject to interventions, such as motivational interviewing, which can address problems related to the fear and negative perceptions of patients regarding returning to work.23 Recent research in Sweden, however, warns that to translate motivational interviewing into a sickness insurance context, training needs to be supported by organisational approaches that promote collective learning and sharing of experiences among officials.24
We suggest that more holistic models, including psychosocial factors, are used in addition to biomedical models. Finally, it is important that rehabilitation focuses on the manipulation of psychosocial determinants (eg, motivational interviewing), next to the treatment of the patient.
The C-index is indicating that in 80% of the cases, a patient who will be sick for more than 6 months, will have a higher risk score than a patient who would be sick less than 6 months.
What is already known on this subject
Psychosocial determinants are important when it comes to sick leave duration, and therefore, standardisation of sickness absence duration solely based on diagnosis will not be as accurate. Despite the existence of some screening instruments for very specific groups, there is little evidence for a generic screening tool based on psychosocial determinants only, tested in all sick people regardless of their diagnosis.
What this study adds
A model with 14 psychosocial determinants will assign a higher risk score to patients who are sick for more than six months than to patients who will be sick for less than six months in 80% of the cases. In a subset of the sample which contained diagnostic information, the psychosocial determinants still performed better (C-index: 0.73) compared with the biomedical model (C-index: 0.63). The screening instrument based on the 14 psychosocial determinants can be applied in social security settings to detect high-risk profiles for long-term sick leave (>6 months). When detecting high-risk profiles, prognostic psychosocial determinants can be used to refer patients towards additional interventions to promote sustainable return to work (RTW).
Footnotes
↵I 28 October 2016—Royal Decree amending the Royal Decree of 28 May 2003 on the health surveillance of employees with regard to the reintegration of disabled employees, s.d.
Contributors KG is the main author of the manuscript. She worked on the conception of the project as well as on data collection, analysis and interpretation of the data and writing the manuscript. SD was involved in the data collection processes of this validation study and was a formal connection between the university and the sickness fund organisations. She coordinated the data collection process within the sickness fund organisations and was present in meetings with these organisations. DR reviewed the manuscript. MDB provided support in the practical organisation of the study and has reviewed the manuscript. IB provided support in the analysis and the writing of the manuscript. LG assisted in the data collection processes of this validation study. He assisted in organising meetings with the sickness fund organisations. He assisted in writing and providing feedback for this article. He also contributed to the conception of the project and in the interpretation of the data as well as in writing the manuscript.
Funding This study was funded by the National Institute for Health and Disability Insurance.
Competing interests All authors wish to acknowledge that no part of this work is submitted elsewhere. Saskia Decuman, a co-author in this project, works for the National Institute for Health and Disability Insurance (funding organisation). She was involved in the organisation of the study and connected researchers with sickness fund organisations. She was not involved in the research process (methods, analysis or writing the manuscript). Otherwise, there was no conflict of interest.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.