Article Text

Statistics from Altmetric.com
Editor,— Differences in mortality between areas have been found to be related to the socioeconomic conditions of the area.1 2 However, people also move to improve their physical and social environment, and the health status of the migrants differs considerably from that of the non-migrants.3Recently, Davey Smith and collegues4 found that mortality, measured 1991–92, was inversely related to the population growth in the two preceding decades in 292 areas in Britain. They found a negative correlation between population change and mortality both in men and women, although the correlation was somewhat stronger in men.
We investigated the association between population growth and mortality in the 16 municipalities of the county of Värmland in Sweden. The population change, as percentage increases or decreases between 1975 and 1994 was counted from the official population statistics. In Sweden, the official population statistics are based on continuous registration of births, deaths and migration. Although the population change was similar in both sexes (correlation 0.99), we calculated it separately for men and women. Mortality in 1992–96 was derived from the database administered by the Centre for Epidemiology, National Board of Health and Welfare. Age standardised total and cause specific mortalities have been calculated using weights from a Swedish standard population (1970).
The county of Värmland is an area with one of the highest mortalities from cardiovascular disease and non-insulin dependent diabetes in men and women in Sweden. The municipalities include several industrial municipalities with comparably high rates of unemployment, some rural municipalities, a few municipalities with growing populations, and the city of Karlstad, a growing centre of the county. The number of inhabitants in the different municipalities varied between 4700 and 79 000 in 1994, while 12 of the 16 municipalities had more than 10 000 inhabitants.
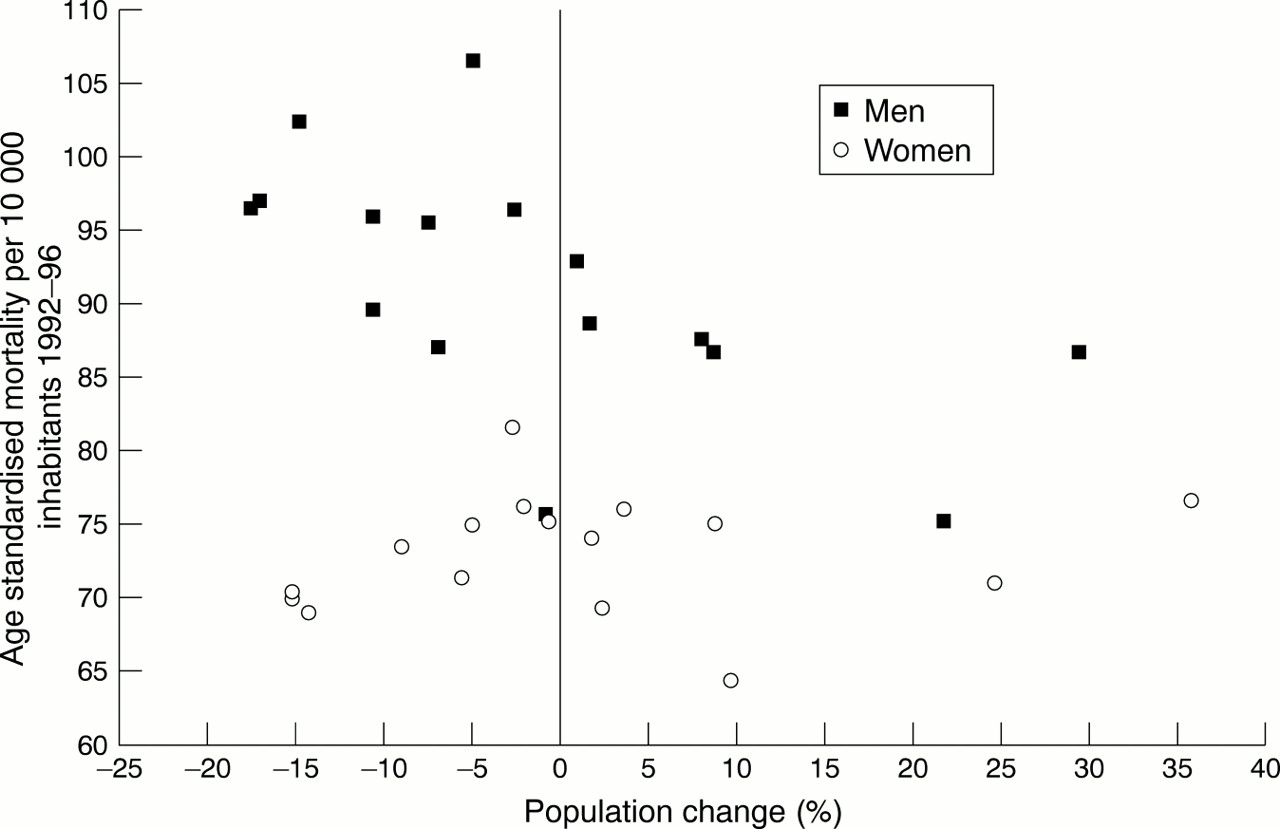
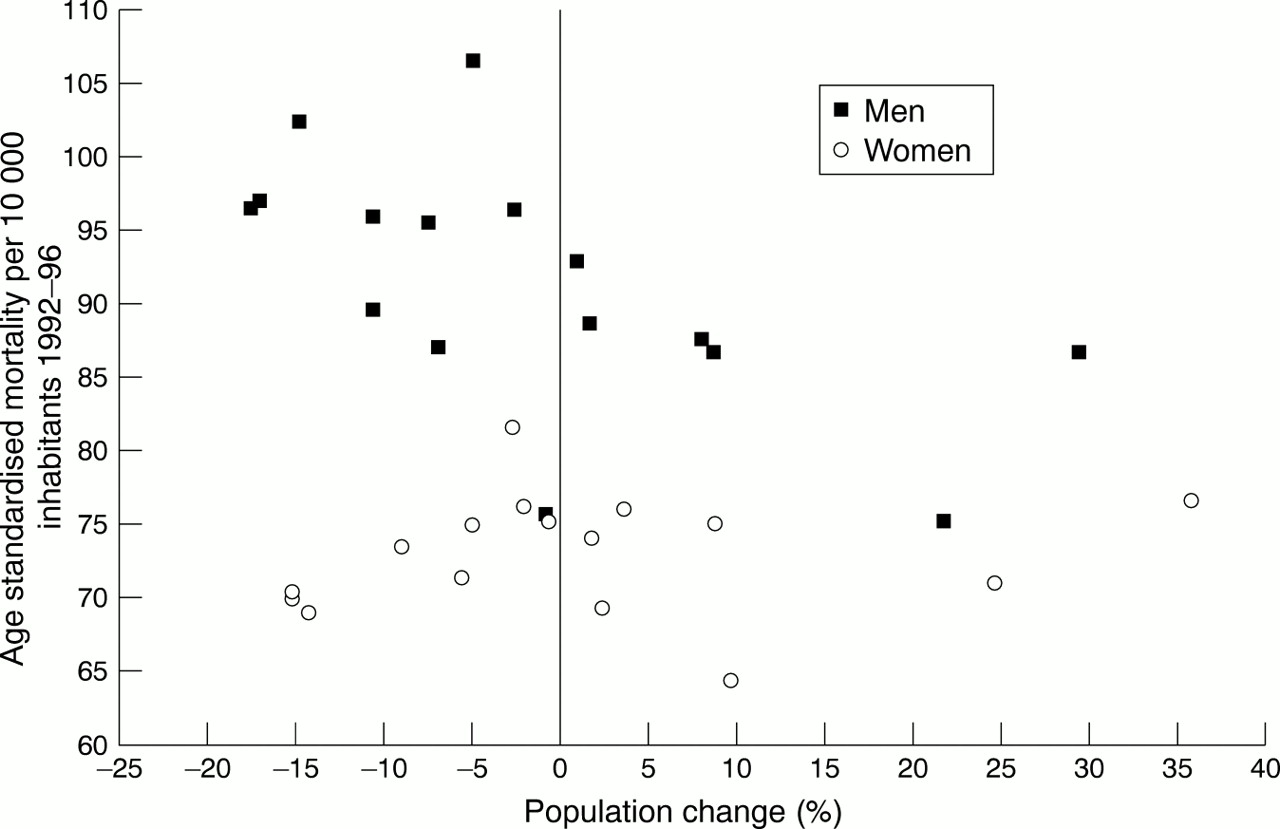
We found a similar inverse association between population change and mortality as Davey Smith and collegues4 in men but not in women (fig 1). The correlation between population change and age standardised all cause mortality was −0.61 (p=0.013) in men. In women, the correlation was positive but not statistically significant: 0.15 (p=0.57). Analysis of male cause specific mortality showed strongest correlations between population change and mortality from cancer (r=−0.62, p=0.011), alcohol related diseases (r=−0.56, p=0.025) and mental disorders (r=−0.50, p=0.050). Similar negative but somewhat weaker correlations were observed for mortality from cardiovascular disease, diabetes and lung cancer. In women, only mortality from diabetes was inversely related to population change (r=−0.49, p=0.055), and to a lesser degree mortality from mental disorders (r=−0.27, p=0.31). Because we only had 16 municipalities in the analysis, we repeated the analysis using non-parametric (rank) correlations. The results from the non-parametric analysis were similar to those from the parametric analysis. We also calculated the correlation between population change between 1975 and 1990 and mortality in 1988–92 and the results were consistent with those for the period 1992–96.
{kind=link}
Mortality among men and women in the 16 municipalities of the county of Värmland, Sweden, and population change 1975–94.
Population growth is closely linked to the socioeconomic conditions and deprivation of residential areas. In our study, population change was positively correlated with the proportion of inhabitants with high income (over 266 055 SEK in 1995) and proportion of inhabitants with high education (more than high school) and negatively correlated with the unemployment rate in the municipality. Therefore we calculated partial correlations between population growth and mortality controlling for these factors. The correlation between population change and all cause mortality in men was −0.41 (p=0.13) after controlling for proportion of inhabitants with high income. This indicates that about one third of the correlation between population change and mortality was explained by the proportion of inhabitants with high income. Controlling for proportion of inhabitants with high education and proportion of unemployed had a weaker effect on the association between population growth and mortality.
Why did we find the inverse association in men but not in women? It seems that, in women, different causes of mortality have different associations with population growth. Although diabetes mortality was inversely related to population growth, especially breast cancer mortality was higher in many of the growing areas (correlation between population change and breast cancer mortality 0.39, p=0.137) than in the shrinking areas. Female breast cancer mortality is known to be associated with affluency5 and was also in our study more common in municipalities with high proportions of inhabitants with high income (r=0.45, p=0.079) and less common in municipalities with high unemployment rates (r=−0.77, p<0.001). In men, all the cause specific mortalities studied were inversely related to population growth.
This study suggests that the association between population growth and mortality differs between men and women. Men in growing, wealthy areas are better off than men in shrinking, less affluent areas. Migration seems to strengthen the inverse association between affluency and mortality as healthier people move to more physically and socially attractive areas. This is indicated by the fact that population change was more strongly related to mortality than income or unemployment rates. The negative association between population growth and mortality does not unequivocally hold for women, among whom the association may be cause specific. Our study comprised only 16 municipalities and the findings should therefore be verified in a larger sample of areas. However, even in such a small sample of areas, the findings were consistent with previously published studies on population change and mortality in men and on socioeconomic conditions and breast cancer mortality in women.