Article Text

Statistics from Altmetric.com
- Epidemiology of ageing
- EPIDEMIOLOGY
- SOCIAL EPIDEMIOLOGY
- Social and life-course epidemiology
- SOCIAL INEQUALITIES
The occurrence of adult disease is related to lifetime experiences and, at least in part, to early life events. It is now well established that socioeconomic circumstances across the lifetime are major determinants of adult health and disease, and the current economic crisis is amplifying susceptibility to disease and unhealthy ageing in disadvantaged subgroups of the population. In adulthood, the gap between social groups is extensive in terms of mortality, functional performances and cognitive capacity. Since the occurrence of adult disease is related to lifetime experiences, including early life exposures, late-life preventive efforts may be of limited efficacy, particularly in disadvantaged subgroups. We now have the analytical tools to understand mechanisms that underlie life-long susceptibility to unhealthy ageing, and new knowledge can lead to better and more effective mechanisms to prevent diseases and reduce health inequalities. In this perspective, we first discuss the impact of recent changes in the understanding of chronic disease aetiology on our interpretation of the influence of life-course socioeconomic status (SES) on health and ageing. We then propose a model for integrating the exposome concept (the myriad of exposures derived from exogenous and endogenous sources) into the analysis of life-course socioeconomic differentials in ageing.
Changes in disease understanding
In the last decades, the conceptual framework for disease aetiology has changed significantly for non-communicable diseases, which are responsible for two-thirds of global mortality. One of the most important developments concerns the notion of disease inter-relatedness, which is now well established for cardiometabolic diseases such as obesity, diabetes and circulatory diseases, but which also potentially applies to Alzheimer's disease/dementia1 ,2 and cancer.3 Endocrine physiology, immune and inflammatory processes as well as important risk factors such as hyperglycaemia and health-related behaviours are shared by most chronic diseases. As a consequence, non-communicable diseases may be conceptualised as a continuum of conditions with phenotypic overlapping between the traditional clinical categories (cancer, neurological diseases, cardiovascular disease, metabolic syndrome), shared risk factors and underlying mechanisms. Not surprisingly, the observed commonalities between diseases and their shared physiological pathways have demonstrable molecular links.4
Another important notion that has revolutionised the conceptualisation of non-communicable diseases is that of ‘action at a distance’, in which early-life exposures have long-term consequences, as highlighted by work on the developmental origins of adult disease.5 ,6 This is a novel idea in medicine, which has traditionally viewed causes of disease as proximal events.
A third important development is the representation of health as a ‘trajectory’ instead of conferring a static status on it. Under this concept, across the life course, some individuals progress rapidly towards (multiple) disease states while others remain healthy, as a consequence of an accumulation of positive/adverse exposures from early through adult life and old age. There is now considerable evidence that socioeconomic circumstances across the life course (from in utero to old age) are among the most powerful determinants of ageing trajectories in the population. In fact, healthy ageing involves a progressive differentiation across groups representing different levels of SES from conception to old age.7 Low SES across the life course is associated with early death and poor ageing,8 ,9 and this fate is in part dependent on early life experiences.10
Life trajectories and health capital
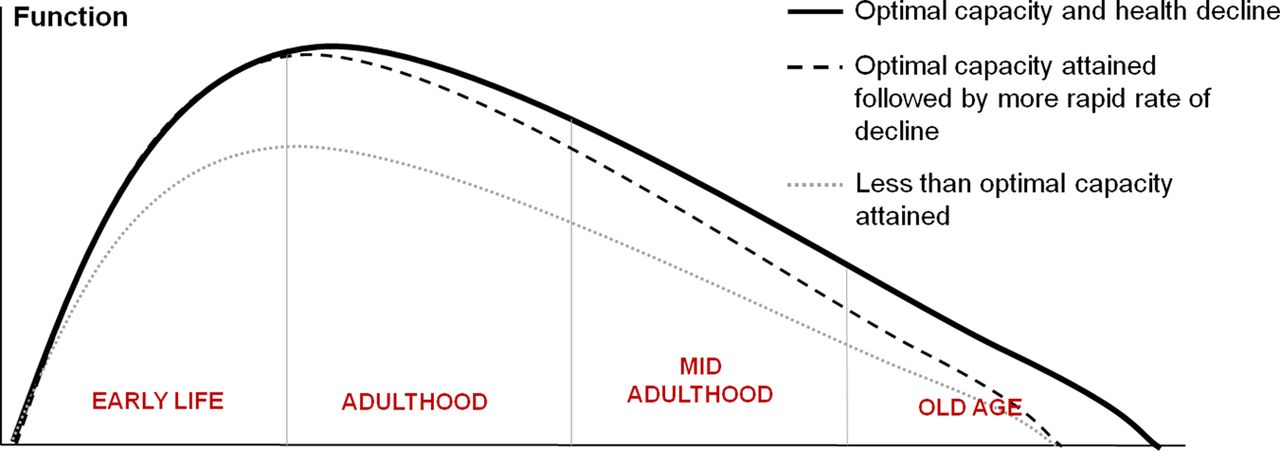
The revised Strachan-Sheikh model of life course functioning provides a useful illustration of ageing that permits SES to be viewed as a major driver of ageing trajectories.11 In this model, ageing is broadly conceptualised as a two-stage process: build-up and decline.12 The ‘build-up’ stage, which begins at conception and early intrauterine life and ends with late adolescence, is characterised by rapid successions of developmentally13 and socially sensitive periods.14 Exposures in this stage strongly determine the maximum attained health, with an impact on subsequent ageing trajectories (figure 1, dotted line). The second stage, starting in early adulthood, is defined as the period of ‘decline’ from maximum attained capacity to loss of function, disease and death. Exposures during the second stage can influence the rate at which functioning is lost (figure 1, dashed line).
{kind=link}
The modified Strachan-Sheikh model of life course health trajectories. Adapted from Strachan and Sheikh.11
The build-up stage—from early intrauterine life to late adolescence—is characterised by heightened sensitivities to biological and social environments, and encompasses multiple life phases. The concept of sensitive periods in life-course epidemiology is borrowed from notions originally identified in neurobiology and physiology.15 During a phase of rapid development, a biological system is more sensitive to environmental exposures and especially to deviations from ‘normal’ exposures.16 In fact, developmental processes occurring earlier in a human life course are linked to the most fundamental biological functions such as growth and neurodevelopment. Later, during the development of higher functions such as socioemotional behaviours, sensitive periods are likely to be longer and to vary greatly between individuals.17 In any case, SES appears to be a powerful determinant of an individual’s maximum attained level of health.18 ,19
Although some of the views on the long-term consequences of early life may be overly deterministic, a better understanding of sensitive periods may elucidate mechanisms that contribute to the production of health inequalities.20
Recent research—including our own—suggests that early life socioeconomic conditions during sensitive periods may be stored in cells through epigenetic modifications that can be sustained for decades.21 ,22 This notion is complicated by the fact that epigenetic modifications may also be inherited at birth, with the implication that individuals may be affected by the socioeconomic circumstances experienced by their parents and grandparents.23 ,24 The identification of sensitive periods, as well as determining when adverse socioeconomic circumstances and their health consequences actually start, are still matters of debate.
Regarding the second stage of ageing that begins in early adulthood, SES (with its associated exposures) appears to be a strong determinant of the rate of decline. In high-income countries, adverse socioeconomic circumstances are no longer associated with food restriction and physical fatigue, but more often correlate with food abundance (albeit of poor quality), lack of physical exercise and psychosocial stress (including sleep deprivation and mental problems).9 ,25–27 Other factors potentially explaining the impact of low SES on health are higher exposure to environmental hazards in living and work places, social and financial stress, or access to and utilisation of healthcare.
The exposome and its connections to inequality
Interestingly, the actual biological pathways linking low SES to phenotypic expression have hardly been explored. We propose that socioeconomic circumstances across the life course affect human physiology and disease processes through a myriad of exposures derived from exogenous and endogenous sources. As shown in table 1, the totality of exposures, also called the ‘exposome’,28–30 is related in many ways to SES and other complex variables, including diet, inactivity, urbanisation and regular medical care, that are in turn related to SES.
The human ‘exposome’ and its relationship to indicators of SES in high income countries
Depending on the particular combination(s) of sources and mediating factors involved, exposures can influence both the build-up and decline phases of ageing. Moreover, as shown in table 1, associations between particular classes of exposures and SES can be either positive or negative, also depending on the specific context being investigated. Looking first at exogenous exposures that are generated by chemicals and particulate matter from external media, smoking, occupation and environmental pollution, are generally associated with lower SES, but this is not always the case. For example, low SES has been associated with higher exposures to traffic pollution (eg, polycyclic aromatic hydrocarbons and lead) while high SES has been associated with greater exposures to toxicants from seafood (arsenic, mercury and some perfluorinated compounds).31 Likewise, although cumulative exposures of poor urban residents to specific allergens during the first 3 years of life was associated with increased respiratory atopy, exposures to particular allergens in the same population during the first year of life—when the immune system is established—significantly reduced atopy.32 Moving next to endogenous exposures that are generated inside the body, blood levels of high-density lipoprotein (ie, ‘good’) cholesterol that reduce cardiovascular-disease risks are associated with high SES while those of inflammatory proteins and homocysteine that increase risks are associated with low SES.33 Also, factors affecting the microbiome—diet, urbanisation, antibiotic use, caesarean birth and breast feeding—can alter the constellation of important signalling molecules produced by the gut and can be differentially related to SES.34 And, finally, inactivity and psychosocial stress affect blood levels of endogenous molecules—sugars, lipids, inflammatory proteins and reactive oxygen species—which profoundly increase chronic disease risks and are generally associated with low SES.12
Although the exposome elaborated on in table 1 is undoubtedly responsible for variation in the life course trajectories embodied in figure 1, the complex interplay of individual risk factors and their connections with SES present challenges for establishing causal pathways.
Conclusions
Health is socially and biologically constructed from the earliest moments of life and travels across the life span along complex trajectories where dynamic processes are in continuous interaction. It is possible to examine these processes within a framework that merges the life-course approach with the aetiological concept of a disease network and thereby promote understanding from the molecular to the societal level. Such an approach allows us to examine the roles that exposures play in healthy ageing and enable all of us, regardless of social position, to improve our lives. It is clear that late-life approaches to prevention are often ineffective because they cannot influence the trajectory. Thus, particular attention should be paid to discovering those early-life exposures that are most discriminating for life course trajectories.
The rising economic inequality we currently confront35 raises profound implications for human health that must be addressed. Given the plethora of exposures—derived from exogenous, endogenous and social sources—that can be associated with income inequality, we encourage investigators to move away from traditional strategies that focus on individual exposures or sources, towards exposomic approaches, which embrace the full milieu.28 Since the instability of global markets and lack of growth may be accompanied by instability of health indicators and ageing trajectories, it is essential that we develop these strategies soon.
References
Footnotes
Twitter Follow Michelle Kelly-Irving at @shell_ki
Funding This work was supported by the Swiss National Science Foundation (Ambizione grant n° PZ00P3_147998 to SS) and by the European Commission (Horizon 2020 grant n° 633666).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.