Article Text

Statistics from Altmetric.com
An Olympic year brings intensified interest in sport and exercise,1 with the anticipation of competitors reaching new feats of athletic performance. But what recent progress has been made in the field of physical activity and health research? The last 50 years or so of epidemiological research in physical activity have provided strong evidence for the beneficial effects of physical activity on a range of health outcomes. The promotion of physical activity for health is supported by at least 39 different disease-specific clinical guidelines,2 including the National Institute for Health and Clinical Excellence. However, there remain several clinically relevant and interrelated issues in the field that have been the topic of much research and debate in recent years; these include, but are not limited to defining the minimal dose of physical activity required for health benefit; investigating the emerging role of sedentary behaviour in the physical activity—health area; developing interventions to effectively promote habitual physical activity in the general population.
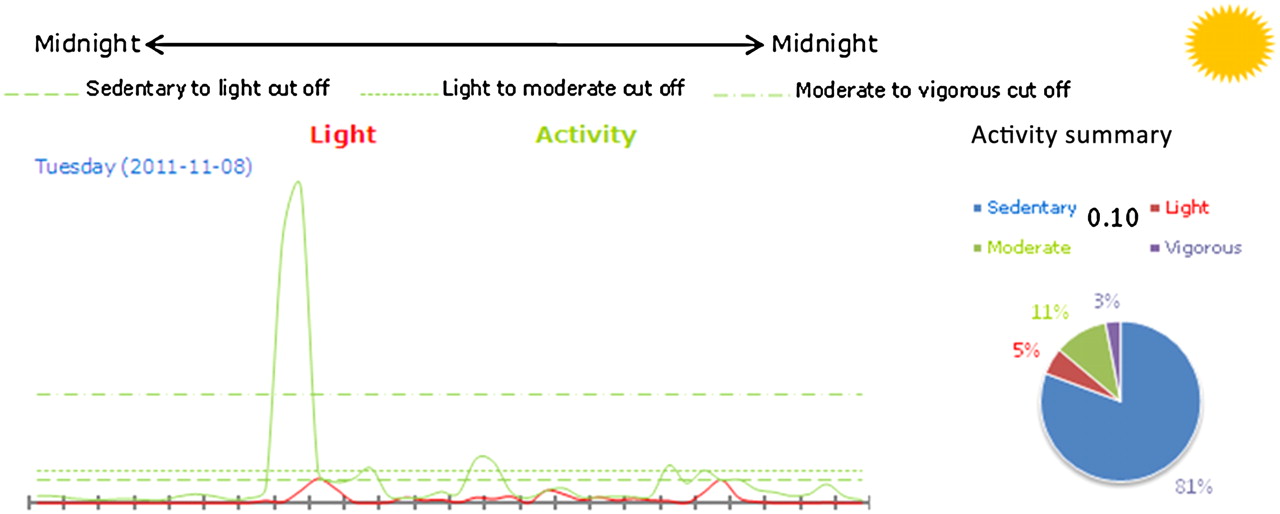
One of the most significant developments in the field over the last decade has been the introduction of small solid-state accelerometer devices that now permit physical activity to be assessed objectively over several days at low cost, thus making it is feasible to incorporate such measures in large-scale population studies, such as the National Health and Nutrition Examination Survey and the Health Survey for England. Physical activity epidemiologists have traditionally employed self-report measures, which have the possibility of introducing reporting biases and making it more difficult to precisely define the dose-response association between physical activity and health. Objective measures are not only able to assess intensity and duration of activity more effectively, but can also better delineate the duration of continuous bouts of activity and periods of prolonged inactivity (sitting) (see figure 1). Indeed, there tends to be a modest correlation between self-reported and objectively assessed levels of physical activity, as confirmed by the data presented in this edition of Journal of Epidemiology and Community Health.3

{kind=link}
Data from an accelerometry device that was worn by a healthy male participant over a 24-h period. The data emphasises the vast amount of time that the average person spends sedentary.
The current guidelines recommend that the general population undertake at least 30 min of moderate to vigorous physical activity on five or more days of the week, although recent evidence has suggested that a lower volume of activity (3.75–7.49 MET-h/wk ∼ 15 min a day) may be protective.4 The dose-response gradient tends to be curvilinear with the largest health gains seen in the first 1–2 h of activity a week, and this trend was highlighted by data presented in this edition of Journal of Epidemiology and Community Health that examined the dose-response association between physical activity and measures of health-related quality of life in a large cohort of Australian women.5 These issues are particularly relevant for clinical practice because, given the barriers to physical activity, it would be desirable if patients could gain benefit from incorporating a relatively low level of physical activity into their treatment modalities. Objective measures will help further refine the physical activity guidelines and dose-response associations in the future.
Another area in which objective measures have contributed is to the emerging science of sedentary behaviour. A rapidly accumulating body of evidence from observational studies has identified sedentary behaviour (time spent sitting) as an important risk factor for chronic disease. Recent evidence from some,6 but not all7 studies using accelerometry-based measures have observed detrimental, linear associations of sedentary time with various metabolic risk factors after controlling for physical activity. Thus, there appears to be some evidence to suggest distinct, yet overlapping pathways involved in the adverse health outcomes associated with sedentary time beyond that which is due to a lack of physical activity per se. Indeed, because time spent in moderate to vigorous physical activity is such a small component of the overall waking day, a large amount of the variance in sedentary time across the population is related to the balance between sedentary time and light-intensity activity. Therefore, in addition to the benefits of moderate to vigorous activity, health gains might be observed by rectifying the imbalance between sitting time and light-intensity (‘lifestyle’) activity.
The vast majority of the population in England live largely sedentary lives, and this becomes even more apparent when measured objectively.8 In this edition of JECH, a meta-analysis of 22 studies highlighted the problems of poor adherence to exercise-referral schemes,9 demonstrating a pooled level of adherence of 49% (95% CI 40% to 59%) across the observational studies, and 43% (95% CI 32% to 54%) across the controlled trials. It is becoming clear that action is required on several different fronts to successfully promote and maintain physical activity in the population. Much interest has focused on promoting lifestyle activity in order to displace sedentary time, which crucially might involve making changes to our environment to make it more activity friendly. Recent data has suggested that taking breaks from sedentary time is linked to improved metabolic health, thus novel approaches, such as changing the layout of offices to promote more movement (eg, moving printers so that office workers must walk to collect their printing) may prove effective.
Active commuting has also gained interest in this area,10 although infrastructures of towns and cities are often not conducive to such activity. Physical activity epidemiologists have recently been involved in designing tools for the economic assessment of the health benefits of walking and cycling to assist developers in planning new infrastructure,11 which might prove hugely beneficial in providing an incentive to develop activity-friendly cities. One of the crucial issues is targeting those populations that are most in need of behaviour change, such as the elderly, socially deprived and ethnic minorities. There are, however, further barriers to physical activity behaviour change in deprived areas, such as unsafe streets, dilapidated parks and lack of resources and facilities. Changing health behaviours in low-income groups can, therefore, be challenging and complex. Indeed, at present, there is limited available evidence on the efficacy of community-based physical activity interventions, which tend to produce small effects that are difficult to sustain over the long term.12 The recent white paper (Healthy lives, healthy people) that encourages individuals to take more responsibility for their own health behaviour, and introduces concepts such as ‘nudging’ and ‘incentives’ for increasing physical activity, has proved controversial. Thus, the puzzle of how to promote health-enhancing physical activity in the general population is still far from solved. Although athletes may reach new athletic feats at London 2012, we still have much progress to make in persuading people to be more active and sit less in their daily lives.
Footnotes
Funding MH is supported by the British Heart Foundation (RE/10/005/28296).
Competing interests None.
Provenance and peer review Commissioned; internally peer reviewed.