GPs’ workload climbs as government austerity agenda bites
BMJ 2014; 349 doi: https://doi.org/10.1136/bmj.g4300 (Published 02 July 2014) Cite this as: BMJ 2014;349:g4300
- Gareth Iacobucci, news reporter, The BMJ
- giacobucci{at}bmj.com
Nearly all general practitioners in a new survey carried out by The BMJ said that their workload had risen in the past year as a result of their patients’ financial hardship.
Over 1000 GPs responded to the survey, the results of which showed that doctors working in the country’s most deprived inner city areas were the worst affected by the recent reorganisation of the benefits system and other austerity measures. The findings also indicate that people receiving welfare support because of illness or disability are struggling to cope with cuts to their financial support and are turning to their GPs for support.
The findings come after a recent analysis published by the think tank the High Pay Centre said that the poorest fifth of British households were now among the most economically deprived in western Europe.1
This first part of The BMJ’s investigation focuses on how changes to the employment support allowance (ESA), introduced by the Labour government in 2008 to replace the old incapacity benefit, have affected patients with long term illnesses or disabilities. Many doctors in our survey said that the ESA had increased their workload in the past 12 months, after the coalition government introduced stricter criteria for receiving benefits in the Welfare Reform Act 2012.
As well as being asked more often to provide medical information for their patients’ work capability assessments (WCAs), GPs are also being asked to help an increasing number of patients appeal against the removal of their benefits under the new system, which many believe has wrongly judged them as fit for work.
WCAs are carried out by medical advisers, often nurses, employed by the private company Atos. The firm has been contracted to run the assessments since 2008, but it recently negotiated an early withdrawal from the contract after criticism of its operation of the assessments. A new provider is due to be appointed early next year.2
Alongside its survey The BMJ interviewed doctors, advisers, and patients at general practices in three towns and cities, who raised major concerns about the way the system was working (box 1).
What The BMJ’s survey found
Of 1056 GPs who responded to the survey (see box 2 for details of the survey methods), 94% said that their workload had risen to some degree in the past 12 months because of financial hardship among their patients (fig 1⇓).

The impact seemed to be deepest in inner city areas. Nearly half (46%) of GPs who identified themselves as working at an inner city practice said that their patients’ financial problems had “significantly increased” their workload. The proportion was 39% in towns, 38% in suburban areas, and 33% in rural areas.
Overall, 91% of GPs said that the ESA had increased their workload to some degree in the past 12 months. Within this, more than a quarter (27%) said that the ESA had “significantly increased” their workload, 41% said it had “increased” their workload, and 23% said it had “slightly increased” their workload.
More than half of GPs (57%) said that they had filled in more WCAs for their patients in the past 12 months than in the previous year, while 15% said that they had not filled in more. This increased workload included providing medical information for initial assessments, as well as helping patients with appeals. A further 28% said they were not sure if the number had increased.
The findings reflect the most recent statistics published by the Department for Work and Pensions, which show that the number of appeals against WCA rulings that were subject to a tribunal hearing rose from 181 137 in 2011-12 to 327 961 in 2012-13.3 Of the 224 375 appeal tribunals concluded in 2012-13, 43% were overturned in favour of the claimant.
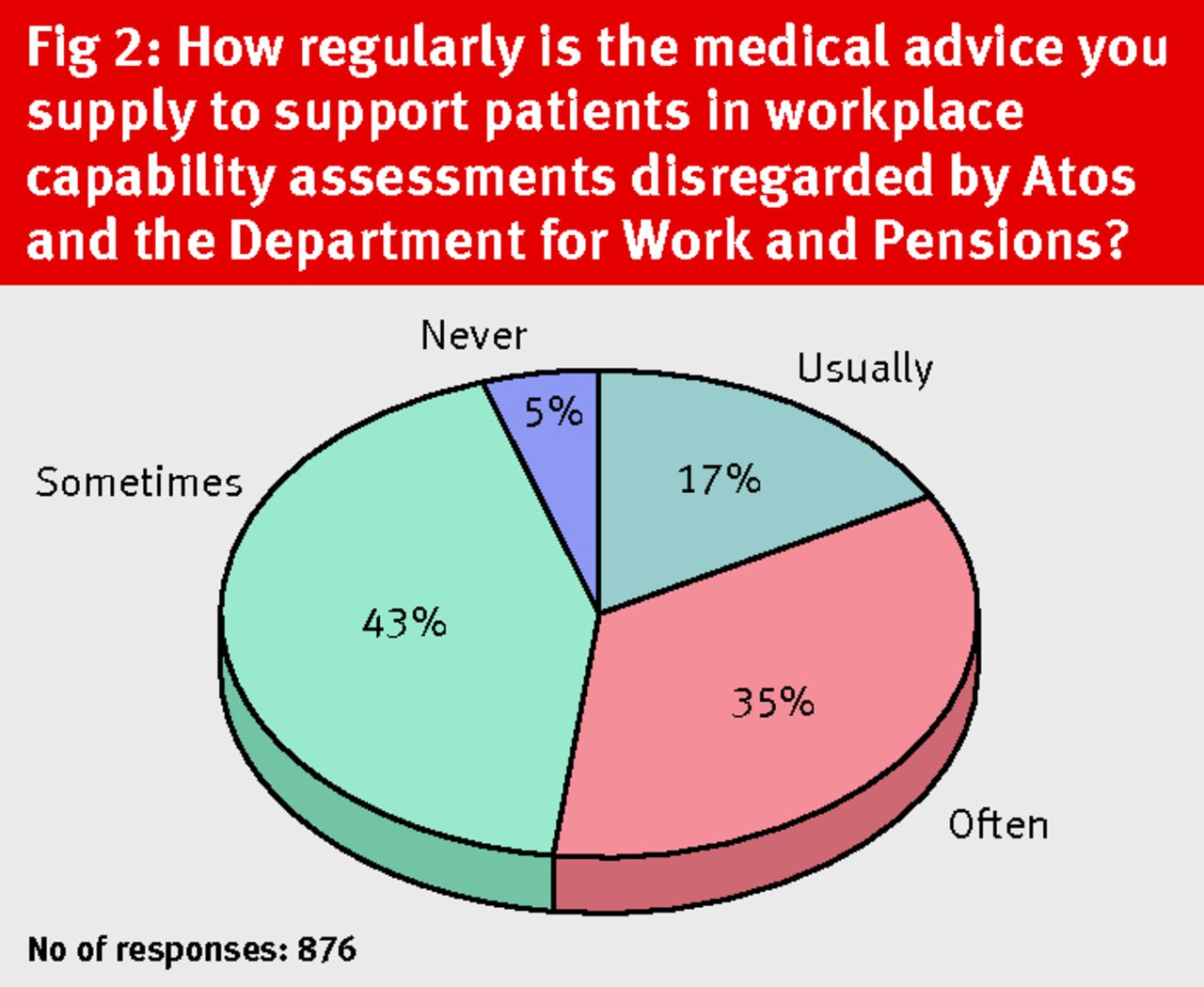
To compound the surge in workload, many GPs thought that their professional opinion was regularly disregarded by the agencies assessing people’s ability to work. More than half of the GPs surveyed (52%) said that the advice they supplied was either “often” or “usually” ignored by Atos and the Department for Work and Pensions (fig 2⇓).

When GPs were asked whether they had seen evidence that their patients’ health was being harmed by reductions to their benefits, 68% of those who responded to the question said that they had. The proportion was highest among GPs who identified themselves as working in inner city areas (77%), followed by those in towns (71%), suburban areas (65%), and rural areas (58%) (fig 3⇓).

{kind=link}
{kind=link}
{kind=link}
Changes to disability and employment support benefits
Doctors are increasingly being asked to provide medical information for the controversial WCAs, which people who are ill or disabled must undergo to assess their eligibility for ESA. They are also dealing with the effects on health among people who have had their benefit payments cut, many of whom have mental health problems or disabilities.
The WCAs have been heavily criticised by doctors,4 patients, charities,5 and MPs, who claim that they are inflexible and punitive towards sick and vulnerable people. Reports have surfaced of people committing suicide after being incorrectly assessed as fit to work.6 The government and the company it contracted to run the assessments, Atos, negotiated an early end to the contract in 2014 after heavy criticism.
The ESA was first introduced in October 2008 by the then Labour government to replace incapacity benefit, which was paid to those below the state pension age who could not work because of illness or disability. The allowance was initially paid only to new benefit claimants but was extended by the coalition government from 2011, with the aim that all existing claimants would be migrated to the new system and reassessed by 2014.
Stricter assessments
The key difference between ESA and its predecessor was the introduction of the stricter WCAs to replace the personal capability assessment. The Department for Work and Pensions said that the new system would be more rigorous and would help more people into work.
In this system claimants who score 15 points or more in WCAs are considered unable to work. These claimants then receive a basic ESA weekly payment of £72.40 (for those aged 25 years or over) or £57.35 (16-24 year olds), plus an additional £35.75 a week for those who attend support groups.
Claimants who don’t meet the 15 point threshold receive less money overall: the same £72.40 or £57.35 basic payment, but with an additional payment of £28.75 a week for attending “work related activity groups.” Claimants in this second group must be seen to be taking immediate steps towards moving into work to avoid sanctions. Before the coalition’s Welfare Reform Act 2012, claimants in this group who did not comply with this requirement lost 50% of the work related activity component (£28.75) for the first four weeks of non-compliance and all of it for all weeks of non-compliance thereafter. None of their basic payment was docked.
Tougher sanctions
But the Welfare Reform Act introduced tougher sanctions for those who breached the terms of their benefits (box 3).7 Claimants can now immediately lose their entire basic rate (£72.40 or £57.35) if they do not demonstrate that they are trying to seek work. Although those in breach now retain the full work related activity component (£28.75), the changes mean many people in this group are now substantially worse off financially.
The act also introduced a stricter time limit of one year on claiming ESA for those who were either in work related activity groups or the initial assessment phase.8 Charities say that this change has resulted in thousands of people losing some or all of their benefit support.9
To compound matters, there are lengthy ongoing delays in the initial assessment process, with hundreds of thousands of people waiting in limbo for decisions on whether they are eligible for support.10
Against the backdrop of these tougher sanctions, many more patients are appealing against the decision to remove their benefit payments. This has created additional work for GPs, who are often asked to support appeals.
Many GPs surveyed by The BMJ thought that their professional opinion was too often disregarded by assessors sticking to a crude scoring system.
Box 1: What GPs, other staff, and patients told us
The BMJ spent three days visiting three centres in England to observe at first hand the effects of austerity policies and the changes to benefits and to ask doctors, other healthcare and related staff, and patients about their experiences.
Hackney, northeast London
Jonathan Gore, GP partner, Lawson Practice
The Lawson Practice serves 13 000 patients in Hackney, one of the most deprived local authorities in England. The population is ethnically diverse, and most of the practice’s patients are from low income households. The practice has seen a growing number of patients requesting help with the employment support allowance (ESA).
It [the ESA] has definitely generated more work. It’s not part of NHS work, and you would normally charge a fee, but these are people that are struggling with their money, so you might feel that you couldn’t ask them to pay a fee. It’s really a reduction in our income to provide a service for nothing. Plus, if you do that, you can’t be doing something else. It’s a patient contact that’s generated that would otherwise not have happened. It’s a 10 minute consultation, 15 minutes writing a report and planning it, and the secretary’s time.
There is definitely some truth that not a great deal of attention is given [to the information GPs provide]. What they [the assessments] are not able to do is to see how cumulative problems—often physical and psychological—interact to create disability.
As a GP, I do see work as a healthy option. It’s probably more use than your “five a day” [the recommended number of portions of fruit and vegetables]. There are tremendous health benefits to being in work. Yet, [although] some people may be able to change their outlook and employment, it’s a bridge too far for a lot of people, and it makes them more stressed and worried because it’s another pressure in their life.
The most vulnerable are the most affected, partly because they don’t have the same abilities to deal with this sort of thing and because it may then be the straw that breaks the camel’s back. This will leave them with stress and anxiety and creates more work for health professionals and GPs. And you wonder about other family members and how it impacts them.
Anonymous patient, 58, Lawson Practice
The patient has been “in and out of hospital” since the age of 16 with arthritis and is also a carer to her partner, who has had an amputation. Having previously being classed as having limited capability for work, she was reassessed last year and had her benefits reduced. She believes that she is not fit for work and is currently appealing the sanction on her benefits.
I’m appealing it, but I’m worn out by it. I’m attending the hospital. They’ve said [I have] crumbling arthritis and spurs on the knee. I’m going down all the possible routes to help myself, but, realistically, sending me back to work [would mean] taking every second day off work. I will not be able to maintain a job. It’s unrealistic of them. I’m nearing 60. It has an impact on my life: I am incapacitated. They’re not sensitive enough.
If they do find me fit for work I’m not going back [to work]. I’ll have to declare myself bankrupt. I don’t know how they can find me fit for work. They are over-riding my GP’s decision, and if they were to ask the consultant at the hospital he would concur and say, “Look at her knee.”
Hamra Yucel, family support coordinator, Hackney WellFamily Service (part of the charity Family Action)
The Hackney WellFamily Service provides “brief emotional and practical support” to patients in this deprived area of London. The service was first set up by GPs in the 1990s to respond to the many social problems their patients presented with. It is now busier than ever before. Advisers have access to patients’ medical records and can liaise directly with the GPs. Yucel spends one day a week working at the Lawson Practice.
There has been a surge in the number of referrals, and it’s actually an ongoing thing. They are sanctioning people a lot here. We are having meetings with job centres. People who are illiterate, or have dyslexia, or mental health issues, or people who don’t have the motivation, are being sanctioned again and again. Those people suffer a lot when they have to deal with job centres, because they [the centres] don’t seem to understand the underlying issue.
Felixstowe, Suffolk
Paul Driscoll, GP partner, Haven Health
Haven Health is located in a deprived pocket of the coastal town of Felixstowe in Suffolk, close to the largest container port in the United Kingdom. Many of the 6000 patients registered here are of working age, and the practice is seeing more and more people asking for help after their benefits have been removed.
There’s not enough sensitivity at the other end to work out who is entitled [to benefits]. I think there is almost a culture of “fail everybody and then sort them out at tribunal.” It seems a very insensitive way to deal with people.
You’re not necessarily doing anybody any favours by letting them carry on [receiving benefits] indefinitely. But in some instances the way it has been handled has been very insensitive and caused a lot of distress—and undermined our confidence in the whole system. Often the benefits can be stopped quite abruptly, and there doesn’t seem to be any recognition that that is going to cause distress to people if money suddenly stops. I’m very keen to get people back to work where possible, but it can’t just happen overnight, and there is very little structured help to get them back to work.
We’re seeing a lot of quite poor decision making [in assessments], particularly for people with mental health problems. I have patients with chronic fatigue who have been I think very poorly treated. I think there’s a real lack of understanding of mental health in the benefits system. I think judgments are made inappropriately on very flimsy evidence.
Because people are having problems, we’re seeing them more often because of deterioration in their mental health or crisis situations. We can see people several times a week because everything is falling apart for them, which puts quite a strain on it.
I would like a bit of respect as a GP. I do question people before I support them [in appeals]. On one hand we’re being asked to provide reports. But then we’re told via a letter from the minister that as an advocate of the patient, the GP “is not in a position to dispense advice to the decision maker on benefit entitlements.” Then don’t bother asking me for them! It takes quite a lot of time to fill in. I fill them in seriously. But I’d be happy doing other things with my time. For them then not to be taken seriously is slightly dispiriting.
Janet McGregor, outreach worker, Felixstowe Citizens Advice Bureau
McGregor holds sessions at Haven Health once a week. GPs refer patients for advice on many issues, including work capability assessments (WCAs). The volume of people being referred has “increased dramatically” since the recent welfare changes. McGregor said that assessments were often wrongly finding patients fit for work.
When people are assessed [in WCAs] they are either put in a work related activity group [where patients must demonstrate they are looking for work in order to receive their benefits] or a support group if they get to 15 points—the magic number. It’s very strict. You have to fit into a box, and if you don’t fit into this descriptor box you are not going to get any points. There is no leeway.
Every person who I’ve tried to [transfer] from the work related activity group to the support group has been successful, which shows the amount that had been assessed wrongly.
The other sad thing is, when these people go to a tribunal, they actually win their appeal.
Middlesbrough, Teesside
John Canning, GP, Endeavour Practice
Middlesbrough is among the areas with the worst health outcomes in the UK and has high unemployment. Canning, who also chairs the professional fees and regulation subcommittee of the BMA’s General Practitioners Committee, said that GPs were in a difficult position when patients asked them to support their appeals against benefit reductions.
I am becoming increasingly aware of people with physical jobs who are getting into the second half of their 50s who are just not capable of continuing to do their job, because the various bits are wearing out [and] they just can’t sustain it as they could when they were 25. They’ve got concerns about their safety, but they haven’t got the attainments and abilities to move on and do other jobs. It might be possible to do some of these things, but doing it on a sustainable regular basis, seven hours [a day], five days a week is difficult. You might be able to do it once, but doing it at the right speed at the right time can be a problem.
The other thing—particularly for people with physical and mental health problems—is whether they are capable of working consistently. Or do they have an illness which has relapses, so they have to have periods of time off work? The WCA doesn’t look at the individual, it merely looks at the mechanical output of the score. The doctors who do it [for Atos] tell me they aren’t able to apply their professional skills of actually being able to assess the score against the person.
The other problem with the appeals process is when someone comes to see me who has been passed fit for work, and they say, “I’ve been told to appeal and need a note.” If I say, “No, I think you’re capable of working,” and they are one of the 40% who wins their appeal, they will come back to see me later and say, “You told me I was fit for work. You were wrong.” It puts the GP in an impossible position.
Box 2: Investigation background and methods
The BMJ’s investigation was prompted by a series of recent trends in UK general practice. As patient demand continues to outstrip available resources, GPs have faced a surge in their overall workload. More than half (54%) of the GPs who responded to a recent BMA survey said that their current workload was “unmanageable” or “unsustainable.”11
Alongside this, The BMJ heard numerous anecdotal reports from GPs who told us that a rising number of appointments were being taken by patients presenting with non-medical problems relating to issues such as debt and unemployment.
Against the backdrop of the UK government’s austerity programme, The BMJ set out to examine the extent to which recent welfare changes and other austerity measures were contributing to the increase in GPs’ workload, as well as affecting patients’ health and wellbeing.
The BMJ emailed a link to the online survey to 28 602 GPs. The survey was active from 5 June to 16 June 2014. A total of 7151 recipients opened the email, and 1056 responded to the survey.
The BMJ also asked doctors to say which environment best described where they worked. The four options were “inner city,” “town,” “suburban,” and “rural.” Of the 863 who responded to this question, 24% (204 people) said “inner city,” 27% (229) “suburban,” 35% (304) “town,” and 18% (153) “rural.”
Alongside the survey The BMJ interviewed doctors, staff, and patients at three general practices. These took place at Haven Health in Felixstowe, Suffolk (5 March 2014), Endeavour Practice in Middlesbrough (10 April 2014), and the Lawson Practice, Hackney, northeast London (7 May and 20 May 2014).
Box 3: Changes to the welfare system in the UK
Many of the government’s austerity measures were enshrined in the Welfare Reform Act 2012 and are being introduced gradually over the next few years. These include:
The introduction of universal credit, a single benefit payment to replace six of the main means tested benefits and tax credits, to be rolled out gradually between 2013 and 2017.
Changes to the employment support allowance, including reassessing existing claims, tougher sanctions for claimants who do not meet the terms of their benefits, and stricter time limits on receiving benefits for people deemed fit enough to be looking for jobs. Implemented from April 2013.
A cap of £26 000 in total that each household can claim each year in benefits (equivalent to £500 a week after tax for people with children). Implemented from April 2013.
Introduction of personal independence payments (PIPs) to replace the disability living allowance. Gradual rollout between April 2013 and October 2017.
Changes to housing benefit, including the introduction of the underoccupancy penalty (“bedroom tax”). Implemented from April 2013.
Tougher penalties for fraud and error in claiming benefits.
Abolition of national council tax benefit support for people of working age in England. Local authorities to be given responsibility for running their own council tax reduction scheme. Implemented April 2013.
Notes
Cite this as: BMJ 2014;349:g4300
Footnotes
In the second part of its investigation The BMJ looks at the effects on GPs’ workload of the “bedroom tax” and patients’ debt and unemployment (BMJ 2014;349:g4301, doi:10.1136/bmj.g4301).
Provenance and peer review: Commissioned; not peer reviewed.
Competing interests: None declared.