Article Text

Abstract
Objective: To examine differences in short- (28 days) and long-term (5 years) risk of death in patients hospitalised for the first time for various cardiovascular diseases (CVD) by country of birth and/or parental country of birth.
Design: A nationwide prospective cohort of CVD patients.
Settings: Entire Netherlands.
Patients: 118 691 patients hospitalised for the first time for various CVDs were identified through the national hospital discharge, the Dutch population and the cause-of-death registers.
Main outcome measures: Differences in short-term and long-term risk of death. Cox proportional hazard models were used to estimate the mortality hazard ratios.
Results: After adjusting for age, compared with Dutch patients, Turkish, other non-Western and Western migrants had both a short- and long-term higher risk, while Suriname patients had only a long-term higher risk of total-mortality and combined-CVD mortality. These higher rates were driven mainly by an increased risk of short-term (hazard ratio 3.21; 95% CI 1.03 to 10.03) and long-term (2.29; 1.14 to 4.60) mortality following congestive heart failure (CHF) among Turkish; short-term (1.56; 1.10 to 2.20) and long-term (1.50; 1.11 to 2.01) mortality following cerebrovascular accident (CVA) among the other non-Western migrants; short-term mortality following CVA (1.10; 1.01 to 1.19) and long-tem mortality following CVA (1.10; 1.03 to 1.17), and, to a lesser extent, CHF and myocardial infarction among Western migrants; and a long-term mortality following CVA (1.29; 1.05 to 1.57) among Surinamese patients.
Conclusion: Higher mortality after a first episode of CVD was found in ethnic minority patients than in Dutch patients. These differences hardly changed after adjusting for possible confounders, suggesting that treatment and secondary prevention strategies may be less effective in these groups. More research is needed to explain the possible causes of these inequalities.
Statistics from Altmetric.com
Cardiovascular disease (CVD) is the most common cause of death in Western societies.1 Variations in mortalities of CVD have been observed among different ethnic groups, with most studies showing higher rates in ethnic minority groups than in the host populations.2–4 Recent mortality data in The Netherlands, for example, showed that compared with European Dutch people, mortality from CVD was higher among Surinamese, Antillean/Aruban and Turkish ethnic groups.2 Studies on ethnic differences in mortality risk following CVD events are limited in Europe, and the limited data in the UK show inconsistent results. While some authors have found better survival after initial admission with stroke5 and acute myocardial infarction (AMI),6 others, in contrast, have found poor survival after initial admission with AMI7 among ethnic minority groups. Similar inconsistent results have also been reported among the USA ethnic groups.8–11 However, many of these studies were either based on localised populations5 7 11 or short-term in their follow-up.7 10 It is also unknown whether ethnic differences in mortality risks differ in short- and long-term after initial admission with CVD in other European countries with large proportions of ethnic-minority groups such as The Netherlands. In addition, there is no information on mortality risk following CVD events in some of the largest ethnic groups such as Turks in Europe. Understanding the various stages where ethnic disparities in CVD mortality are discernible is crucial for addressing ethnic disparities in CVD mortality. The main object of our nationwide study was to assess differences in short- and long-term mortality risks following first hospitalised admissions for cerebrovascular disease (CVA), peripheral arterial disease (PAD), AMI and congestive heart failure (CHF) between ethnic groups in The Netherlands. Ethnic groups were identified on the basis of country and/or parental country of birth.
METHODS
To construct a cohort of patients first hospitalised for CVD that is being followed for events, information from the national hospital discharge register (HDR), the Dutch population register (PR) and the causes of death register of Statistics Netherlands were linked. The method used for the linkage of Dutch registers has been described previously for a cohort of AMI patients.12 Data on hospital admissions were derived from the HDR. Since 1986, all general and academic hospitals and most single-specialty hospitals participate in the hospital discharge register. For each hospital admission, a new record is created in the HDR, including information on date of birth, sex, numeric part of postal code (since 1991), hospital-specific patient identification code, type of hospital, admission date and principal diagnosis of the admission. The principal diagnosis is determined at discharge and is coded using the ninth revision of the International Classification of Diseases (ICD-9-CM).13 The HDR is a database on admissions, not persons. Following individuals over time based on HDR information alone is troublesome due to difficulties in identification of different admissions from the same person in time and admission for the same condition at a different hospital (due to referral or to address changes). Yet, linkage with the PR may overcome these aspects.
The PR is a dynamic register and comprises information on all registered persons living in The Netherlands, and contains information on date of birth, sex, current address, postal code, nationality, country of origin (of both the registered person and their parents) and date of emigration. The registry is longitudinal, and all changes since 1995 are traceable with their period of validity. It is known that for the entire Dutch population, approximately 85% of the combinations of date of birth, gender and postal code are unique (ie, occur only once in the registry and thus identify one person).14 Information on the cause of death has been derived from National Statistics. Death has been coded using the tenth revision of the International Classification of Diseases15 (ICD-10).
Cohort enrolment
All hospital admissions for AMI between 1 January and 31 December 1995, (ICD-9-CM code 410), and all hospital admissions for CVA, PAD and CHF between 1 January and 31 December 1997 and 1 January and 31 December 2000, (ICD-9-CM code 430–438, 362.3), (ICD-9-CM code 440–444, 7854) and (ICD-9-CM code 402, 428), respectively were selected. By merging with the population registry, only those patients with a unique combination (linkage variables date of birth, sex and numerical part of postal code) were selected. Next, the first hospital admissions in 1995 for AMI and in 1997 and 2000 for CVA, CHF and PAD were selected. To identify first admissions, the file was merged with a file in which, through the same linkage procedures, information was collected on hospital admissions that occurred previously (1991–1995, 1995–1997 and 1995–2000, respectively) for the same condition. For the years 1991–1994, a different—and slightly less reliable—linkage procedure was used, because the digital population register started only in 1995.12 Those with a previous admission for the same condition were excluded; for example, those with a previous hospitalisation for CVA were excluded from the CVA cohort, but not from the cohorts dealing with PAD, AMI or CHF. This approach left a cohort of patients admitted to hospital for the first time because of the occurrence of CVA, PAD, AMI or CHF. Finally, the cohort was linked with the causes of death register to obtain information of date and cause of death (in-hospital and out-of-hospital) during follow-up. Patients were censored if they migrated out of The Netherlands during follow-up.
Comorbidity
The presence of comorbidity was based on discharge diagnosis of previous admission (up to 5 years earlier) or on secondary diagnoses present at the index admission.
Approval for the use of the anonymised patient data was covered by a general agreement between Statistics Netherlands and Prismant. Additionally, the Dutch association of hospitals (NVZ) approved the use of the hospital registration data for this study. No separate ethical approval was necessary for the use of these data. We followed the principles of existing data protection legislation of The Netherlands at Statistics Netherlands.14
Minority groups in The Netherlands
The groups were classified according to country of birth and/or the country of birth of the parents in accordance with The Netherlands Statistics definition.16 The main minority groups in The Netherlands include Surinamese, Antilleans/Arubans, Turkish, Moroccans, Western and other non-Western migrants.16 Suriname was a former Dutch colony. The Surinamese population is ethnically diverse and mainly consists of people who originate from West Africa, South Asia and mixed origin people. The Antillean/Aruban population is predominantly of West African, European and mixed origin, and its migration to The Netherlands has been relatively stable over time. Turkish and Moroccan men came to The Netherlands as labour migrants in the 1960s and 1970s, and were later followed by their families. The term “Western migrants” is used to refer to people who came to The Netherlands via other European countries, North America, Australia, Indonesia and Japan. The term “other non Western migrants” comprise people who came to The Netherlands from other parts of the world, including China, South Asia, Sub-Saharan Africa, Caribbean islands, Middle East and South America.16
Data analysis
Cox proportional hazard models were used to study differences between ethnic minority and Dutch patients in their risk of deaths. Mortality in three different periods was examined: short-term (from admission to 28-day), 1-year (from admission to 1 year thereafter) and long-term (from admission to 5 years thereafter). For each period, two successive models were fitted to adjust for potential confounders and comorbidities: model I adjusted for age and sex, and model II adjusted for age, sex, province, degree of urbanisation and history of CVA, PAD, AMI, CHF, other cardiovascular diseases (other than the disease of the index admission) and diabetes. Results were presented as hazard ratios (HR) with 95% CIs. Kaplan–Meier plots, with comparisons between the ethnic groups were produced using survival function. All the Kaplan–Meier plots were adjusted for age and sex. Data were analysed with SPSS software, version 13.0 (SPSS, Chicago).
RESULTS
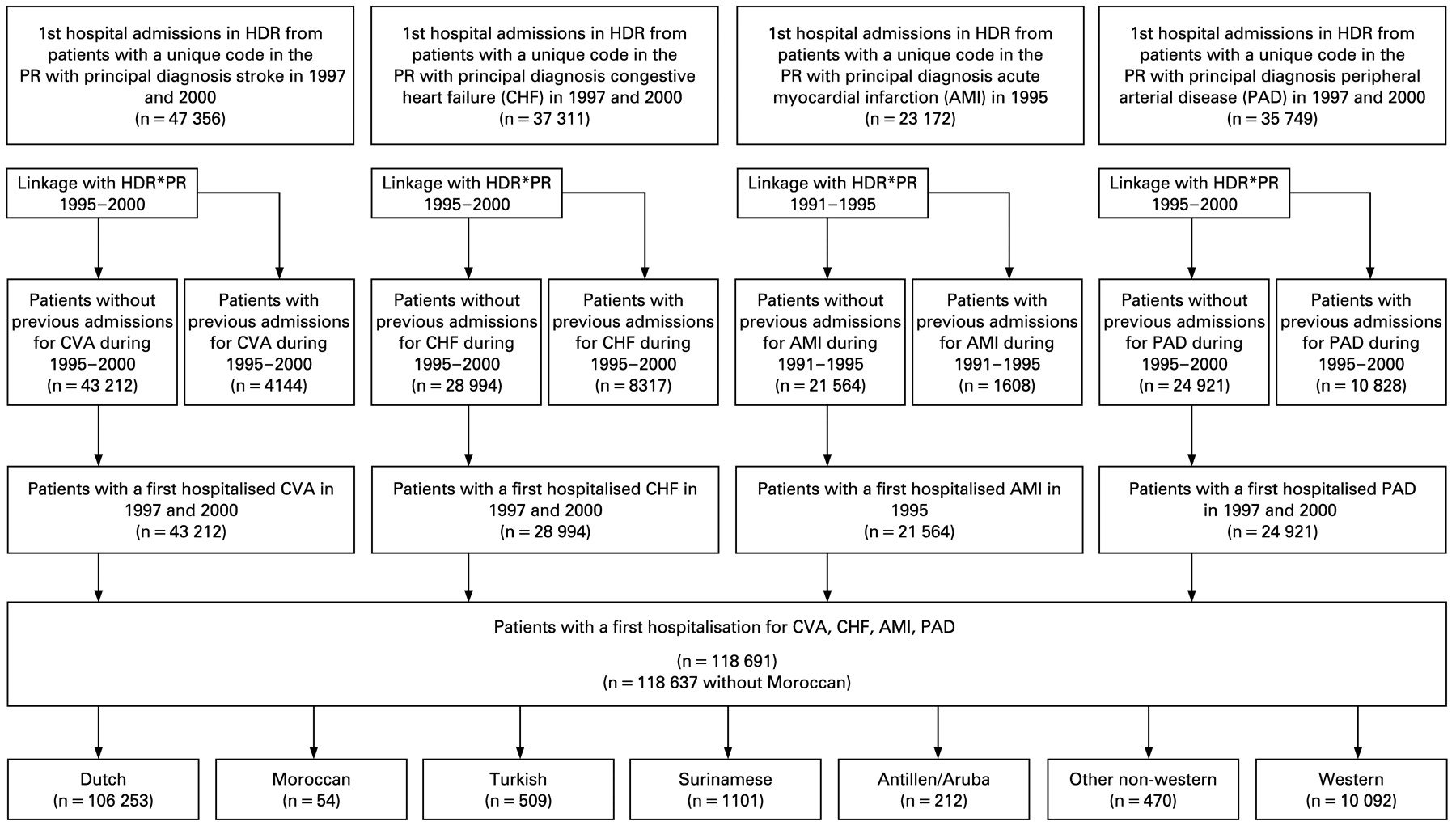
Figure 1 shows a flow chart of the selection process and the number of patients first hospitalised with CVD. In total, 118 691 patients of different ethnicities (Dutch, Moroccan, Turkish, Surinamese, Antillean/Aruba, other non-Western and Western) were included in the cohort. However, only a limited number of patients (n = 54) were Moroccans, and they were therefore excluded from the analyses. About 89.5% were Dutch, and 11.5% were from minority background. The ethnic minority patients were younger and were more likely to live in an urban setting than their Dutch counterparts (table 1). Previous hospitalisations for type 2 diabetes mellitus were more common in non-Western patients than in Dutch patients. In total, 20 718 (17.5%) patients died within 28 days, 32 879 (27.7%) within a year, and 56 540 (47.7%) within 5 years.

Flow chart of the selection process of patients with a first hospitalisation for cerebrovascular accident (CVA), congestive heart failure, acute myocardial infarction and peripheral arterial disease in The Netherlands. HDR, hospital discharge register; PR, population register.
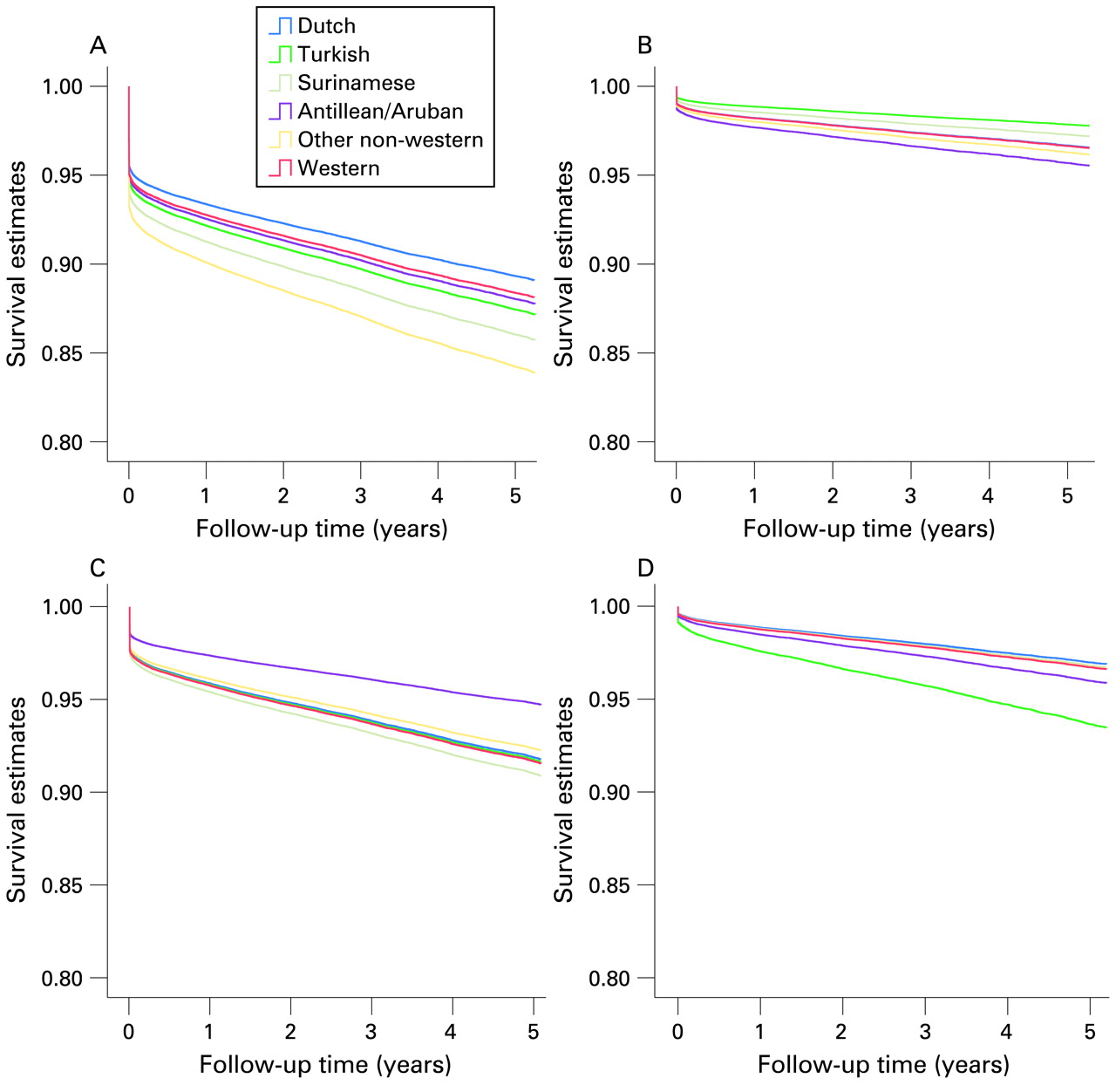
Age- and sex-adjusted Kaplan–Meier plots of survival by ethnic group are shown in fig 2A–D for each CVD. Table 2 shows differences in short-term (28 days), 1-year and long-term (5 years) hazard ratios for total-mortality (all-cause) and combined-CVD mortality following hospital admission with CVD. Table 3 shows the differences in short-term, 1-year and long-term hazard ratios for CVA, PAD, AMI and CHF following hospital admission.
{kind=link}
{kind=link}
Age- and sex-adjusted Kaplan–Meier plots of survival following admission for (A) cerebrovascular accident, (B) congestive heart failure, (C) acute myocardial infarction and (D) peripheral arterial disease by ethnicity.
Twenty-eight-day risk of death
In a Cox regression model, the age- and sex-adjusted hazard ratio for total-mortality and combined CVD mortality following admissions for CVD were significantly higher in Western migrant patients than in Dutch patients (table 2). These differences persisted after further adjustments for potential confounding factors (province, degree of urbanisation, comorbidities and diabetes), which were chiefly driven by higher risks of deaths following CVA and AMI among Western migrant patients. Turkish and other non-Western migrant patients also had (non-significantly) higher risks of total-mortality and combined CVD mortality than Dutch patients. These were mainly driven by a higher risk of mortality following CHF among Turkish patients and a higher risk of mortality following CVA among other non-Western migrant patients (table 3). There were no differences in the risk of death between Surinamese, Antillean/Aruban and Dutch patients following admissions for CVD.
One-year risk of death
At year 1, except for Antillean/Aruban patients, all the minority groups had higher hazard ratios for total mortality than Dutch patients, although only the other non-Western and Western migrant patients’ differences were statistically significant (table 2). Turkish patients also had a non-significantly higher risk, while Western migrant patients had a significantly higher risk of combined CVD mortality than Dutch patients. These increased rates were largely driven by a higher risk of mortality following CVA and CHF among Turkish patients; a higher risk of mortality following CVA among Surinamese and other non-Western patients, and a higher risk of mortality following CVA and AMI among Western migrant patients (table 3).
Long-term follow-up (5-year risk of death)
Except for the Antillean/Aruban group, all the minority patients had a higher risk of total mortality and combined CVD mortality than Dutch patients (table 2). These differences persisted after further adjustment for other potential confounders, though the combined CVD mortality difference between Turkish and Dutch patients was only borderline non-significant (p = 0.07). The increased risks of total mortality and combined CVD mortality were driven predominantly by an increased risk of mortality following CVA among Surinamese and other non-Western patients; an increased risk of mortality following CHF and, to a lesser extent, CVA among Turkish patients; and an increased mortality following CVA and, to a lesser extent, AMI and CHF among Western patients (table 3).
DISCUSSION
This study provides the first nationwide estimate of short- and long-term risks of death after initial admission with various cardiovascular diseases by country and/or parental country of birth. Our findings demonstrate that, overall, minority patients had an increased risk of death compared with Dutch patients except for Antillean/Aruban. Furthermore, the patterns of the short- and long-term mortality differed between the groups.
Turkish, other non-Western and Western patients had both a short- and long-term increased risk of death, while Surinamese patients had only a long-term increased risk of death compared with Dutch patients. These findings contrast the recent studies in the UK.5 6 In Wolfe and colleagues’ study in South London, for example, although African descent patients were more likely than White patients to be admitted with stroke, they had a substantial survival advantage in both the short- and the long-term.5 Fischbacher et al’s retrospective cohort study in Scotland6 also found that South Asians were more likely than non-South Asians to be admitted with AMI, but South Asians had comparatively better survival rates in both the short- and long term. Mukhtar and Littler found no differences in survival rates during the 4 years after an acute myocardial infarction,17 whereas Wilkinson and others, in contrast, found poor survival among South Asians compared with White people during the 6 months after initial admission with AMI.7 The USA studies have also shown inconsistent results,8–11 although it seems, generally, that the survival rate is poorer in African–Americans than in White Americans.8 The reasons for these inconsistent results are unclear. However, many of the earlier studies in both the UK and the USA were based on localised samples or were short-term in their follow-up. Differences in care and local circumstances may contribute to these inconsistent results. By contrast, our current study was based on a nationwide sample with both short- and long-term follow-up.
The explanations for the higher long-term risk of death among ethnic minority groups are not completely clear. However, several factors may contribute to these differences.18–23 It is possible that differences in health service utilisation and quality may contribute to these mortality risk differentials. Evidence in The Netherlands suggests that some ethnic-minority groups use more general practitioner care than Dutch people do.18 However, they are less likely than Dutch people to use specialised care. Although there is no specific information on ethnic differences in healthcare use regarding very specialised invasive procedures such as cardiac catheterisation, coronary-artery bypass graft surgery, angioplasty and carotid endarterectomy in The Netherlands, evidence from the UK and the USA shows important ethnic groups differences in these procedures.19 20 One study in the UK, for example, showed that among patients deemed appropriate for coronary artery bypass grafting, South Asian patients were less likely than White patients to receive it.20 Our present findings warrant further studies to determine whether ethnic inequalities in specialised invasive procedures exist and, if so, the extent to which these differences in these procedures contribute to mortality risk differentials.
Differences in comorbidities/severity of the conditions may also contribute to the differences. However, the differences persisted, even after controlling for comorbidities and other covariates. In addition, if the severity of the condition were worse in minority patients than in Dutch patients, clear differences in the short-term risk of mortality between the groups would be expected in all the minority groups. However, there were no differences in short-term mortality between Surinamese and Dutch patients, which indicate that the differences in severity are unlikely to contribute to these observed differences.
The higher rate of short- and long-term risk of mortality among migrants from other Western countries is surprising and difficult to explain. However, unlike major non-Western groups,2 18 information on CVD and risk factors among the Western groups is lacking. This lack of data may be due in part to the fact that, traditionally, Western migrants have been regarded as being similar to the Dutch people.24 One report, for example, found that of all the minority groups in The Netherlands, Western migrants have the fewest hospital admissions.24 Based on this finding, the Western migrants were regarded as a relatively healthy group. While it is reasonable to interpret fewer hospital admissions as healthy, it could also be interpreted as a lack of access to adequate healthcare, which might contribute to their unfavourable mortality outcomes. These high mortalities underscore the urgent need to study this group to unravel the possible determinants that might contribute to their high mortalities in The Netherlands.
It is worth emphasising, however, that although minority groups had an increased risk of CVD death, these high rates were driven mainly by an increased risk of death following specific types of CVD. Among the Turkish group, for example, the increased risk of CVD death was driven predominantly by an increased risk of death following CHF and CVA. The risk of death following PAD and AMI (short-tem) was, by contrast, non-significantly lower in Turkish patients than in Dutch patients. Similarly, the increased risk of CVD deaths in Surinamese and other non-Western patients was driven mainly by an increased risk of death following CVA. The risk of death following PAD in Surinamese patients, and CHF in other non-Western patients, was non-significantly lower than in Dutch patients. These findings indicate that different strategies may be required for each minority group in addressing mortality differentials.
Limitations/strengths
There are some limitations to this study. As in numerous studies, the classifications of the various groups were based on country of birth. Country of birth may reflect ethnicity reasonably well among some ethnic groups but is likely to be an unreliable proxy measure of ethnicity for other groups such as Surinamese.25 Nonetheless, our recent SUNSET study findings showed that CVD and risk factors such as hypertension and diabetes are higher in both Surinamese groups (ie, African-Surinamese and Hindustani-Surinamese) than in Dutch people.26 27 The Western and other non-Western groups also comprised people from different countries with varying migration histories. There is clear a need to disaggregate the current populations in The Netherlands to facilitate better understanding of health differences between populations. The number of Antillean/Aruban was relatively small, which makes it difficult to draw firm conclusions among this group. The cause-of-death information used in our study was not validated by medical records or autopsy reports. As a result, the degree of misclassification in our estimates of mortality risk is unquantifiable. However, as in almost every study using data from vital statistics, some degree of misclassification is inevitable. In addition, several studies published in the 1980s have shown that the validity of the Dutch national cause of death statistics was higher than the average validity of eight countries of the European community.28
The strength of our current study is the validity of the registries, the linkage methods, the large sample size and the lack of selection of the cohorts. It has been shown recently that 99% of the personal, admission and discharge data, and 84% of the principal diagnoses (validated through medical record review by medical specialists) were correctly registered in a random sample of all hospital admissions registered in the hospital discharge register.29 In addition, over 97% of the uniquely linked hospital admissions resulting from linkage of the hospital discharge register with the population register were shown to be correctly linked.30
Conclusion
Our results demonstrate that, overall, minority groups have an increased risk of death after initial admission with CVD. However, the patterns of the short- and long-term risk of death differ between groups. In addition, the risk of death following each CVD also differs between groups. More research is needed to explain the possible causes of these inequalities so that appropriate public health and clinical interventions can be implemented to address these inequalities in both short- and long-term survival. For example, more work is needed on ethnic differences in specialised invasive procedures such as carotid endarterectomy and their contributions to mortality risk differentials.
Acknowledgments
We thank R Bhopal (Edinburgh University) for his useful comments on an earlier draft. We thank the two anonymous referees, who provided comments that helped to improve an earlier version of this paper.
REFERENCES
Footnotes
Funding: This study was supported by a grant from The Netherlands Heart Foundation (grant number 31653251). The study was part of the project “Cardiovascular disease in The Netherlands: figures and facts” of The Netherlands Heart Foundation. CA was supported by a VENI fellowship (grant number 916.76.130) awarded by the Board of the Council for Earth and Life Sciences (ALW) of The Netherlands Organisation for Scientific Research (NWO).
Competing interests: None.