Article Text

Abstract
Objectives: To quantify changes in 30 day and one year mortality among patients with acute myocardial infarction in southern Derbyshire (population 560 000) in each of five consecutive years (1995–1999) before the publication of the National Service Framework for coronary heart disease, and to assess the proportion of one year survivors in whom serum lipids were measured and were below target values.
Design: All hospital admissions coded on the patient administration system (PAS) as “AMI” (ICD codes I-21, I-22, and I-23) and with a creatine kinase measurement in the pathology database were identified over a five year period (n = 4912). All deaths in the district are automatically notified to the PAS. Total mortality after acute myocardial infarction (30 days and one year) and lipid levels were analysed by year of admission, age group (35–74 years v ≥ 75 years), and sex using unconditional logistic regression analysis.
Setting: An acute hospitals trust and pathology laboratory, as sole service providers for a catchment population of 560 000.
Results: The number of admissions for acute myocardial infarction was similar in each of the five years (n = 4912, 62% male, 63% < 75 years old). Overall, among patients aged 35–74 years there were 396 deaths (13%) at 30 days and 585 (19%) at one year; mortality was higher in women (1.28-fold at 30 days, p = 0.02) and in subjects aged 75 years or more (3.26-fold at 30 days, p < 0.0001). There was a progressive reduction in 30 day mortality of 9%/year over the five year period (95% confidence interval, 4% to 13%, p = 0.012). The proportion of one year survivors (35–74 years) in whom serum lipids were measured at least once increased from 74% in 1995 to 88% in 1999; of these, 27% of men and 23% of women had a total serum cholesterol of < 5 mmol/l in 1995, increasing to 65% and 74%, respectively, in 1998 and 1999 (p < 0.0001).
Conclusions: In the five year period 1995–1999, there was a significant year on year decline in 30 day and one year mortality after admission for acute myocardial infarction, and progressively more patients achieved cholesterol levels below 5 mmol/l. Men were more likely than women to have their lipids measured after myocardial infarction. Mortality at one year was 1.32-fold higher among women than among men.
- myocardial infarction
- blood lipids
- mortality
Statistics from Altmetric.com
Coronary heart disease accounts for over 110 000 deaths a year in England (41 000 are under 75 years of age) and approximately 3% of all hospital admissions. About 1.4 million people in the United Kingdom have angina, and each year 300 000 suffer an acute myocardial infarct.1 The National Service Framework (NSF) for coronary heart disease, published by the United Kingdom government in March 2000, describes a 10 year programme to reduce morbidity and mortality from coronary heart disease in England.2 As part of the NSF strategy, regional health providers are charged with monitoring key outcomes—for example, deaths in hospital within 30 days of admission for acute myocardial infarction—in order to identify geographical variations across the United Kingdom and thus target resources to areas of greatest need.
The highest priority is given to secondary prevention, and with respect to cholesterol reduction the NSF specifies therapeutic targets based on the joint British recommendations3 and the evidence from major outcome studies such as 4S (the Scandinavian simvastatin survival study)4 and CARE (the cholesterol and recurrent events study).5 In patients with established coronary heart disease, statins and dietary advice should be used to lower serum cholesterol concentrations either to less than 5 mmol/l (low density lipoprotein (LDL) cholesterol less than 3 mmol/l) or by 30% from pretreatment levels, whichever involves the greatest absolute reduction.2
Auditing the extent to which various NSF standards and targets are met represents a major challenge. Individual health authorities have already published in-hospital 30 day mortality rates following acute myocardial infarction,6 but these data exclude patients who are discharged and subsequently die in the community, and very little information is available on the proportion of survivors achieving target lipid levels in routine clinical practice. In the ASPIRE study (action on secondary prevention through intervention to reduce events),7 a national survey of secondary prevention practice undertaken by the British Cardiac Society shortly after the 4S study was published, 78% of men and 86% of women with established coronary heart disease had a total cholesterol concentration of 5.0 mmol/l or above.
Our aim in this study—in which we used methods that should be applicable elsewhere in the United Kingdom—was to analyse changes in total mortality and the attainment of lipid targets among patients admitted to hospital with an acute myocardial infarct. To do this, we studied a single English health district over a five year period (1995 to 1999) following publication of the 4S study (in 1994) and before the publication and implementation of the NSF (in 2000).
METHODS
Southern Derbyshire is a large health district with a population of 560 000, served by one Acute Hospitals Trust consisting of two hospitals using a single computerised patient administration system (PAS) and pathology service. All deaths among patients registered with a general practitioner in southern Derbyshire are automatically notified to the Acute Trust PAS.
The PAS database was searched using International Classification of Disease (ICD) codes to identify all patients admitted to hospital with an acute myocardial infarction in each of five consecutive years (January 1995 to December 1999). Specifically, this included ICD codes I-21 (“AMI”), I-22 (“subsequent MI”), and I-23 (“complication following current MI”). Admissions coded I-21, I-22, or I-23 on the PAS were then used to interrogate the pathology database for evidence of a serum creatine kinase (CK) measurement being requested. The purpose of searching for evidence of a CK measurement request was simply to give independent corroboration for the likely correctness (and plausibility) of the ICD coding; it also allowed the date of the infarct to be confirmed. Over 85% of CK measurements were above the reference limit, providing direct biochemical confirmation of acute myocardial infarction, but the criterion for inclusion in the study was that the patient had a hospital admission coded as “AMI” and at least one CK measurement recorded (irrespective of the CK result) (n = 4912). We excluded from the analysis 35 to 45 patients in each annual cohort whose admission was coded as “AMI” but without any evidence of a CK measurement, as this cast doubt over the correctness of the coding (this accounted for less than 4% of coded acute myocardial infarction admissions each year).
The pathology database was also searched for evidence of serum lipid measurements (total cholesterol, high density lipoprotein cholesterol, triglycerides, and calculated LDL cholesterol) among patients admitted each year with an acute myocardial infarct. Among patients who survived at least one year (n = 3382), the most recent set of lipid measurements in the 12 months post-infarction follow up period was used for the lipid analyses by age, sex, and year of admission. For the analysis of survival and lipid measurements, the maximum period of post-infarction follow up for each patient was 12 months.
Statistical analysis
The data were analysed retrospectively, but the inclusion/exclusion criteria, definitions, and statistical methods were defined before beginning the work. Patients were categorised according to age (35 to 74 years, and 75 years or more) and sex. Mortality was calculated by year of admission based on death within 30 days or one year after an acute myocardial infarct. Among those patients who survived at least one year, the proportion in whom serum lipids had been measured at least once and the number with total and/or LDL cholesterol concentrations of < 5 and < 3 mmol/l, respectively, was calculated for each year of admission.
Unconditional logistic regression analysis was used to develop a model relating the odds of each outcome to the variables of age group, sex, and year of admission. The fit of each model was acceptable (assessed on residuals and using the Hosmer and Lemeshow goodness of fit statistic). Thus the 95% confidence intervals and p values quoted for any one factor are simultaneously adjusted for the other factors.
RESULTS
Over the entire five year period, 5166 patients were admitted with acute myocardial infarction; 62% were male and 63% were under 75 years of age. Laboratory CK measurements were requested on 4912 patients (95%).
Total mortality
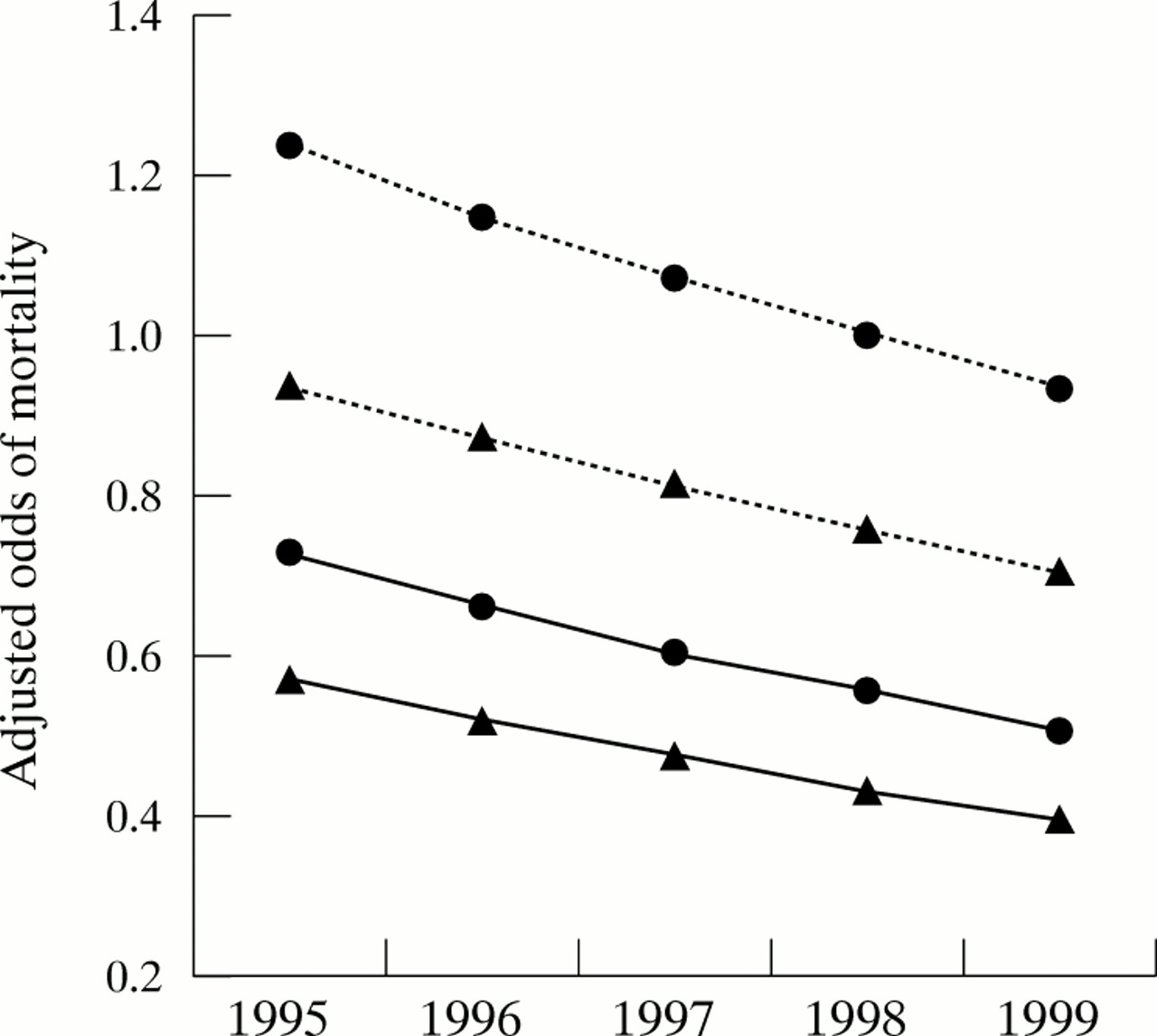
Overall, there were 396 deaths (13%) at 30 days and 585 deaths (19%) (cumulative) at one year among those patients with acute myocardial infarction aged 35 to 74 years. The 30 day mortality figures for each year showed a significant year on year decline, with an annual reduction of 9% a year (95% confidence interval (CI), 4% to 13%; p = 0.012) from 1995 to 1999 (figs 1 and 2). The 30 day mortality among women was 1.28-fold higher than among men (CI, 1.11 to 1.48; p = 0.02), and patients aged 75 years and over were 3.26 times more likely to die than patients aged 35 to 74 years (CI, 2.82 to 3.78; p < 0.0001). Mortality at one year was also significantly higher for women (1.32-fold; p = 0.004) and those aged 75 years and over (3.98-fold; p < 0.001) (table 1).
Mortality at 30 days and one year after acute myocardial infarction
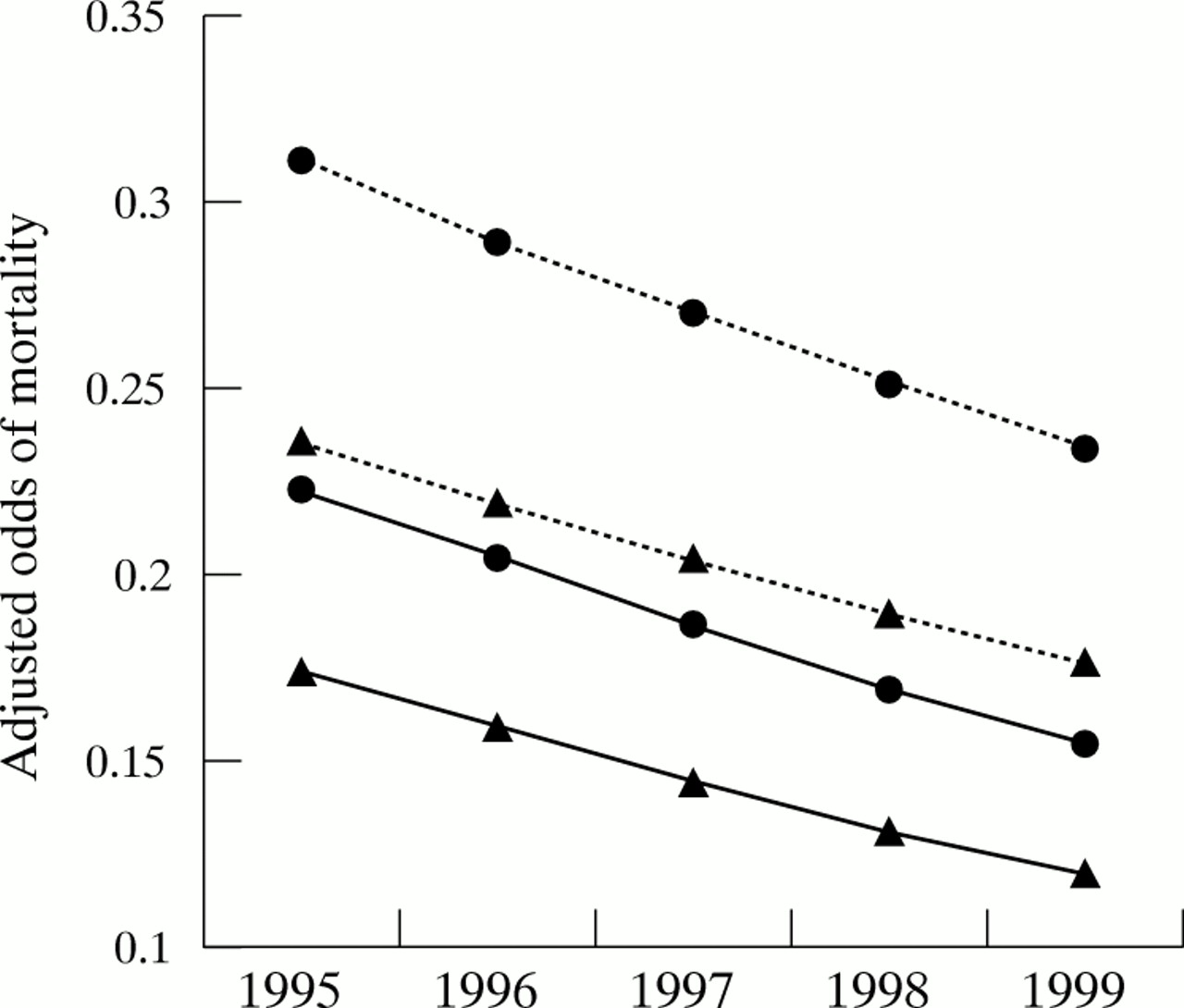
Year on year adjusted mortality odds at 30 days (solid line) and one year (dotted line) for men (triangles) and women (circles) aged 35 to 74 years.

Year on year adjusted mortality odds at 30 days (solid line) and one year (dotted line) for men (triangles) and women (circles) aged 75 years and over.
Lipid measurements among survivors
Approximately three quarters (74%) of the one year survivors presenting with an acute myocardial infarct in 1995 (aged 35 to 74 years) had their serum lipids measured during the 12 month period after their admission. This proportion increased significantly, year on year, to 88% in 1999 (fig 3). The corresponding values for patients aged 75 years and over were 22.5% in 1995 and 53.6% in 1999. The year on year trends in both age groups were highly significant (p < 0.0001). Men overall were 1.60-fold more likely than women to have their lipids measured (p < 0.0001), and in the 35 to 74 year age group men were 6.10-fold more likely to have serum lipid measurements (p < 0.0001; table 2).
Measurement of serum lipids among patients surviving at least one year after acute myocardial infarction

Year on year adjusted odds of having serum lipids measured at least once during the first 12 months following acute myocardial infarction among those who survived at least one year (overall n = 3382). Data are for men aged 35 to 74 years (triangles, solid line), women aged 35 to 74 years (circles, solid line), men of 75 years and over (triangles, dotted line), and women of 75 years and over (circles, dotted line).
Lipid targets among those surviving one year after infarction
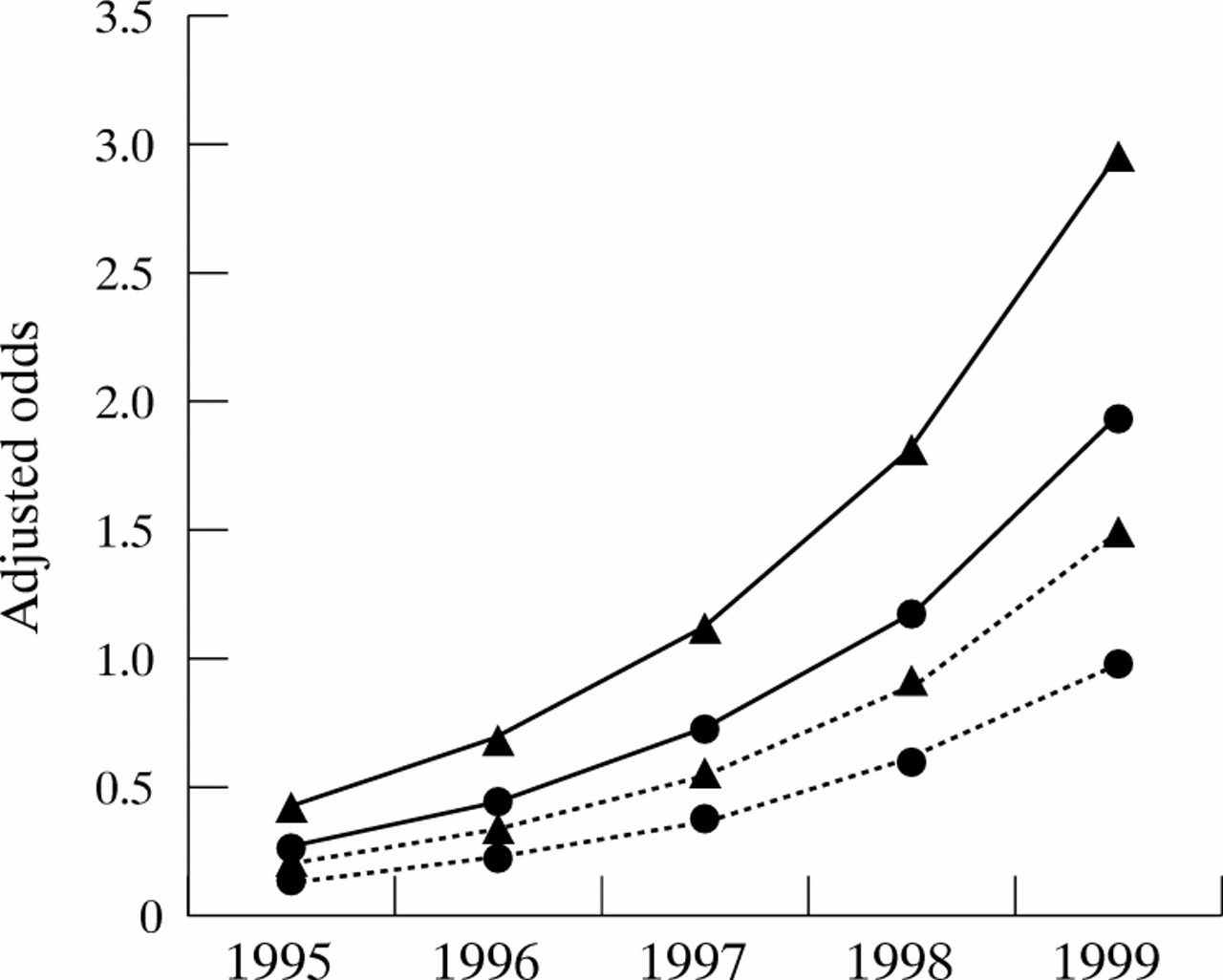
Among patients admitted with acute myocardial infarction in 1995 who survived one year and had their lipids measured, 27% of men and 23% of women achieved the recommended target for total cholesterol (< 5 mmol/l). For those admitted in 1999, the corresponding figures had risen to 74% for men and 53% for women (fig 4). With respect to achieving the LDL cholesterol target (< 3 mmol/l), among the 1995 admissions the proportions were 20% for men and 22% for women, and among the 1999 admissions these had risen to 74% and 65%, respectively (table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Year on year adjusted odds of serum total cholesterol level being less than 5.0 mmol/l among one year survivors from acute myocardial infarction in whom lipids were measured at least once during the 12 months after the infarction. Data are for men aged 35 to 74 years (triangles, solid line), women aged 35 to 74 years (circles, solid line), men of 75 years and over (triangles, dotted line), and women of 75 years and over (circles, dotted line).
Year on year trends for achieving both the total cholesterol and the LDL cholesterol targets were significant (p < 0.0001); for example, the likelihood of attaining the total cholesterol target increased each year by 1.63 times relative to the previous year (CI, 1.53 to 1.74), and for LDL cholesterol the odds of achieving < 3 mmol/l increased annually by 1.93 (CI, 1.79 to 2.09) (table 2).
DISCUSSION
There is very little up to date information about regional or national mortality following acute myocardial infarction in the United Kingdom,8 especially outcome data reflecting routine clinical care in the 1990s after interventions such as the use of thrombolytic treatment, angiotensin converting enzyme (ACE) inhibitors, and statins became widely established. Most of the published information about infarct survival and secondary prevention relates to selected patient populations enrolled in multinational randomised controlled trials, but there is an increasing demand for health care providers to audit and publish outcome data reflecting everyday practice within a local health care network or geographical area. Such data have not been routinely collected or made widely available in the United Kingdom.
More recently, however, individual United Kingdom health authorities, prompted by the National Service Framework for coronary heart disease, have published in-hospital 30 day mortality figures for acute myocardial infarction,6 though these exclude deaths in the community and provide no information about longer term outcome or the clinical implementation of effective secondary prevention. The present study, using information technology that is currently available in most hospital Trusts, provides the first report of all-cause mortality at 30 days and one year for patients admitted to hospital with acute myocardial infarction in a single health district over a five year period (1995 to 1999). Overall, the 30 day mortality was 15% for those aged less than 75 years and 38% for those aged 75 years or more. By comparison, in the United Kingdom component of the World Health Organisation MONICA study (“monitoring trends and determinants in cardiovascular disease”)—undertaken in Belfast and Glasgow in the 1980s and including patients with acute myocardial infarction managed in the community—28 day mortality was between 40% and 49%.9
Analysis according to the year of admission showed a progressive decline in 30 day and one year mortality of approximately 9% a year, with a linear trend that gives no indication of levelling out. The explanation for this annual improvement in survival among those patients reaching hospital with acute myocardial infarction is likely to be multifactorial, but the period 1995 to 1999 is particularly informative. The use of thrombolytic treatment and ACE inhibitors was well established, but the 4S study4—a major landmark in secondary prevention and cholesterol awareness—was published in late 1994, and our data usefully document mortality trends in the five year period between the appearance of that paper and the publication of the United Kingdom National Service Framework for coronary heart disease in 2000. A further comparison in five to 10 years will assess whether key components of the NSF strategy, for example the focus on reducing “door to needle” times and improving delivery of secondary prevention, have had any additional impact on the already declining mortality in patients admitted to hospital with acute myocardial infarction.
Our study included 4912 patients admitted to hospital with a clinical diagnosis of acute myocardial infarction in whom laboratory CK measurements were requested but were not necessarily diagnostic of infarction. The primary criteria for inclusion in the analysis was the ICD code, but the plausibility and correctness of the coding was supported by searching a separate database for evidence of a CK measurement request. In practice, over 85% of these CK measurements were diagnostic of acute myocardial infarction, and we excluded a small number of admissions (less than 4%; 30 to 40 a year) in whom the coding of “AMI” was unreliable in the absence of a CK measurement. These criteria for inclusion may, in part, explain the higher 30 day mortality among women. Similar sex differences in outcome have been reported in previous studies,9–12 including a recent large American cohort,13 and there is good evidence from the ARIC study (atherosclerosis risk in communities) that a larger proportion of men die before hospital admission.10 While this might account for the sex differences in short term survival in the present study, the higher mortality among women at one year post-infarction is more likely to reflect differences in secondary prevention practice, in particular the finding that women are less likely to have their serum lipids measured after an infarct and are even less likely to be treated to the target level of total cholesterol of < 5 mmol/l. The survival benefits of statin treatment correlate closely with cholesterol reduction, and in the 4S study each additional 1% reduction in LDL cholesterol reduced the incidence of a major coronary event (coronary heart disease death or non-fatal acute myocardial infarction) by 1.7%.14 Thus our results suggesting that both primary and secondary care physicians adopt a less intensive approach to the measurement and treatment of lipids in women, even after acute myocardial infarction, would be consistent with the better one year survival among men. A recent cross sectional survey of patients with established coronary heart disease in general practice showed that significantly more men than women are prescribed statins.15
The sex differences with respect to lipid measurements and the attainment of target cholesterol values were apparent throughout the five years of the study, but other aspects of secondary prevention also seem to be implemented unequally between the sexes. For example, there is evidence that women with angina are less likely to be referred to a specialist,16 or to undergo a revascularisation procedure,17 and among established coronary heart disease patients aspirin use18 and blood pressure control15 tend to be less satisfactory in women.
Current guidelines recommend that for secondary prevention, statins, and dietary advice should be used to lower total cholesterol levels to less than 5 mmol/l (LDL cholesterol < 3 mmol/l), or by 30%, whichever is greater.2 In practice, it is often easier to achieve a total cholesterol concentration of less than 5 mmol/l than a 30% cholesterol reduction, and the clinical services seldom record percentage reduction in a form that is readily accessible for audit. Thus many of the patients with total cholesterol values of less than 5 mmol/l may not be optimally treated according to the targets specified in the National Service Framework.