Article Text

Abstract
OBJECTIVES To assess whether patients with heart disease in a single UK hospital have equitable access to exercise testing, coronary angiography, and coronary artery bypass graft surgery (CABG).
METHOD Retrospective analysis of patients' medical case notes (n = 1790), tracking each case back 12 months and forward 12 months from the patient's date of entry to the study.
SETTING Single UK district hospital in the Thames Region.
PATIENTS Patients (elective and emergency) with a cardiac ICD inpatient code at discharge or death, or who were referred to cardiology or care of the elderly unit over a 12 month period in 1996–7 (new episodes) were included.
RESULTS Analysis of 1790 hospital case notes revealed that, despite having indications for intervention identical to those of younger patients, older patients (that is, those aged > 75 years) and women, independently, were significantly less likely to undergo exercise tolerance testing (exercise ECG) and cardiac catheterisation. The similar trends for age and access to CABG did not achieve significance. While clinical priority scores also independently predicted access to cardiac catheterisation and CABG, considerable numbers of patients in high clinical priority groups were not referred for either procedure.
CONCLUSIONS The management and treatment of older patients and women with cardiac disease may be different from that of younger patients and men. Given the similarity of the indications for treatment and the lack of significant contraindications or comorbidities as a cause for these differences, one possible explanation is that these patients are being discriminated against principally because of their age and sex. Although clinical priority scores independently predicted access to catheterisation and CABG, large proportions of patients in high priority groups were not referred. This implies that the New Zealand priority scoring system may be more equitable than UK practice. The cost implications of redressing these inequities in service provision would be considerable.
- age
- equity
- revascularisation
- health service priorities
Statistics from Altmetric.com
The UK has one of the highest rates of heart disease in the developed world but one of the lowest surgical intervention rates (for example, coronary artery bypass grafting (CABG)).1 Recent National Health Service (NHS) performance indicators have illustrated the inequity of provision of CABG, as patients with heart disease in some parts of England may be up to four times more likely to obtain heart surgery as patients in other health districts.2 Reasons for this variability are unclear.
Decisions to investigate patients invasively and subsequent management decisions about revascularisation involve issues of clinical appropriateness, patients preferences, and the personal preferences and bias of the physician.3 ,4 The potential for a subjective element in clinical decision making, and consequent scope for bias, strengthens the case for using clinical priority scoring systems for CABG. The system developed in New Zealand identifies patients most likely to derive substantial health benefit from CABG.5 ,6Initially, it was judged that government funding levels permitted surgery to be offered to patients scoring at or above 35 points, which resulted in denial of CABG to patients with a lower score unless their disease worsens and they are regraded. Although all clinical scoring systems inevitably generate controversy, this system was welcomed by many clinicians despite concerns about inadequate total levels of funding, the arbitrary nature of the cut off point below which surgery would not be funded, and the scope for patients and doctors to exaggerate symptoms to achieve a higher grading.7
Recently, the National Service Framework has set standards for prevention, diagnosis and treatment for coronary heart disease in the UK.8 The aim is to reduce deaths from circulatory diseases. To achieve this aim there must be substantial increases in rates of revascularisation using percutaneous techniques or CABG. To achieve this and deliver an equitable distribution of health care, it is necessary to measure the size of the gap between clinical indications for an intervention and the financially affordable level of intervention.
This study provides data on a cross section of hospital patients in a single district general hospital in the UK. The hospital does not have access to either onsite angiographic facilities or cardiothoracic surgery. The aim of this study was to analyse access to exercise testing, coronary angiography, and CABG for patients with diagnosed heart disease by age and sex. Indications for investigation and treatment were then compared with internationally accepted guidelines including referral for CABG by the New Zealand priority score. Target end points for the study were whether the patient received appropriate interventions where indicated, based on appropriateness criteria, after taking into consideration documented contraindications. This study was performed by retrospective external review, thus removing any potential bias among the treating clinicians (in terms of influencing their practice by the effects of being studied).
Methods
The study was a case note analysis of all inpatients (elective and emergency) with a cardiac International classification of diseases, 10th revision (ICD-10) code and new cardiac outpatients (new episodes) attending cardiology or care of the elderly clinics. This wide catchment ensured that eligible patients were not missed and enabled equity of treatment to be explored from a broader perspective. The participating hospital trust was situated in the Thames area and served a catchment population of 185 000 in a socially deprived urban area by national standards (based on Jarman index scoring). Analysis of national hospital inpatient statistics, available from the Department of Health, shows that the intervention rate for CABG in the local population catchment area was comparable with the national average. The focus of this research was on ischaemic heart disease. Other cardiac conditions were included to ensure that eligible patients were not missed (for example, patients with more than one cardiac condition).
Patients' case notes were eligible for inclusion in the study if they were admitted or first attended (new episodes) the study hospital during 1 April 1996 to 31 March 1997 (again, retrospective to ensure data completeness and no Hawthorne effect on clinical practice). Patients' medical casenotes were analysed retrospectively (n = 1790) by tracking each case back 12 months and forward 12 months from the patient's date of entry to the study. Thus, the last patient follow up date was 31 March 1998. Waiting lists for interventions were checked throughout the study period to ensure that study patients with the indications for intervention, without contraindications, and who were referred for them during the study period were not missed. The 12 month forward tracking period was sufficient to take waiting list times for procedures into account (for example, the maximum for angiography and for CABG was 7–12 months, depending on urgency).
Of 5479 case note numbers provided, 1790 case notes were both traced and included as eligible for study, 185 were untraced after three searches over 18 months, and 3504 were screened and discarded as ineligible for inclusion in the study. This was because of overinclusivity of symptoms screened for by the research team to avoid missing eligible patients, rather than ICD miscoding by trust ICD coding clerks. They were judged ineligible for inclusion after checking their notes (for example, the notes revealed that their symptoms were not caused by cardiac conditions but, for example, by chronic obstructive pulmonary disease, gastrointestinal bleeding, obstetric related problems, or viral pneumonia).
Indications for percutaneous transluminal coronary angioplasty (PTCA) were not analysed because it was not the policy of the trust to provide these, nor the policy of the cardiologists on the study site to perform or cross refer for them. This was because of their belief in a weak evidence base in support of PTCA.
DATA COLLECTION
The data collected from hospital case notes were specialty and patient's date of birth, sex, symptoms, diagnoses, results of all recorded tests and investigations, interventions, severity and pattern of disease, comorbidity, and indications for and contraindications to investigations or treatment. Waiting lists were checked throughout the study to ensure that patient referrals for investigations and procedures were not missed.
Severity of condition, risk, and criteria for intervention were measured by the following systems: Canadian Cardiovascular Society functional classification for angina related limitation on activities9; New York Heart Association scale10; Parsonnet 1 and 2 clinical risk scores for heart surgery11 ,12 (versions with and without the age correction (bias) were used for comparison); De Bono clinical priority criteria for cardiac catheterisation and PTCA13; and the New Zealand priority scores for urgency of CABG.5 ,6 The cardiologists and cardiac surgeons who developed and tested the New Zealand criteria agreed to accept a specific numerical threshold as indicative of reasonable levels of public service provision. The New Zealand criteria are based on the results of published outcome studies, with the weighting determined by meta-analysis and regressions, and represent the clinical factors (for example, coronary artery obstruction) considered to be associated with the degree of benefit obtained from surgery. The New Zealand scores do not correct for age and are therefore not inherently age biased. The scores reflect clinical severity (reduction in life expectancy without surgery)—that is, the extent and type of vessel disease, angina, diagnostic testing (exercise stress test), and role functioning (25–34 points: 4–8 months' reduction of life expectancy, intermittent pain or breathlessness when undertaking activities; 35–54 points: 8–12 months' reduction in life expectancy, much reduced quality of life mainly through pain on exertion; > 55 points: 1–2 years' reduction in life expectancy, considerably reduced quality of life because of chest pain, breathlessness on almost any physical activity). Contraindications including relevant comorbidity were taken into account.
The American College of Cardiology/American Heart Association (ACC/AHA) indications for cardiological investigations and interventions, appropriate for 1996–8, were applied using subsections of the fairly restrictive class 1 indications only, which have general international agreement.14-16 For example, the table for exercise testing relates only to patients who fulfil ACC/AHA class 1 criteria (to assess functional capacity and prognosis of patients with known coronary artery disease): group 1 (functional capacity assessment for selected patients after acute myocardial infarction); group 2 (prognostic testing for selected patients with stable angina, without contraindications). The tables presented here for cardiac catheterisation relate only to ACC/AHA class 1 group 1 (post acute myocardial infarction) and group 2 patients (symptomatic patients with unstable angina not responding to medical treatment, without contraindications). These catheterisation patients were then analysed by clinical priority and severity scoring in relation to receipt of CABG. The ACC/AHA scores do not correct for age and thus contain no inherent age bias.
Reliability checks were carried out by an independent coder on decisions to discard and confirmed that all of the discarded cases were ineligible. Hospital ICD coding was validated by researchers' ICD coding from the notes, with good concordance at 80% (Cohen's κ 0.667; standard error (SE) 0.05; confidence interval (CI) 0.57 to 0.77). Intercoder reliability was tested on a sample of 251 casenotes and showed high levels of consistency on all recorded data.
STATISTICAL ANALYSIS
χ2 and χ2 trend tests were used to compare discrete variables to assess their independent influence on the dependent variables of interest (access to cardiac catheterisation and to CABG). Interactions between potentially predictive variables were tested using logistic regression analyses (odds ratios). Age, sex, severity score, and specialty were entered as the independent variables in each model on the grounds of theoretical significance. Each model adjusted for indications for, and contraindications to, the procedures of interest (dependent variables), and 95% CIs were used in each. All variables were entered simultaneously. The goodness of fit statistic that was used was the −2 log likelihood for the model containing only a constant compared with the −log 2 likelihood for the model with all variables entered. In bivariate and multivariate analyses, attention was drawn to differences that achieved a minimum 5% level of significance.
Results
PATIENT CHARACTERISTICS
Fifty one per cent (911) of the 1790 patients were men and 49% (879) were women; 47% (838) were aged under 65 years, 22% (389) were aged 65–75, 10% (183) were 75–80 and 21% (380) were over 80 years old. Fifty two per cent (926) entered through cardiology or care of the elderly outpatient clinics, and 48% (864) were elective or emergency admissions. All were under the care of specialists in care of the elderly, cardiology, or general medicine.
Twenty five per cent of patients (447) had a primary diagnosis of ischaemic heart disease (including angina). Other main diagnoses were heart failure (31%, 546), cardiac conduction disorder (29%, 525), chest pain unspecified (21%, 376), and acute myocardial infarction (7%, 131).
Table 1 shows the sample's distributions on the functional status, clinical risk, and severity (priority) classification scales used. The clinical scales took account of relevant comorbidity and contraindications for intervention.
Functional and clinical severity classifications of sample
EXERCISE TOLERANCE TESTING (EXERCISE ECG) AND CARDIAC CATHETERISATION (CORONARY ANGIOGRAPHY)
While 265 patients in total underwent exercise tolerance testing, just 26% (155) of the 596 patients who met the ACC/AHA criteria, and for whom an exercise tolerance test was not contraindicated, had one.
Thirty three per cent (148) of patients aged under 75 who met the ACC/AHA criteria for exercise tolerance testing had this test compared with just 5% (7) of those aged 75 and over (p < 0.01). Thirty two per cent (115) of men and 17% (40) of women who fulfilled ACC/AHA criteria had this test (p < 0.01).
Age, sex, and specialty were entered into a logistic regression model and all achieved significance. Table 2 shows that the odds of having an exercise test were multiplied by 0.96 for each additional year of age, indicating a decrease with older age; and the odds of a man getting the test were 1.63 times that of a woman. The model included cardiology and general medicine, with care of the elderly as the referent.
Logistic regression analysis of whether patient had exercise tolerance test if they met ACC/AHA criteria
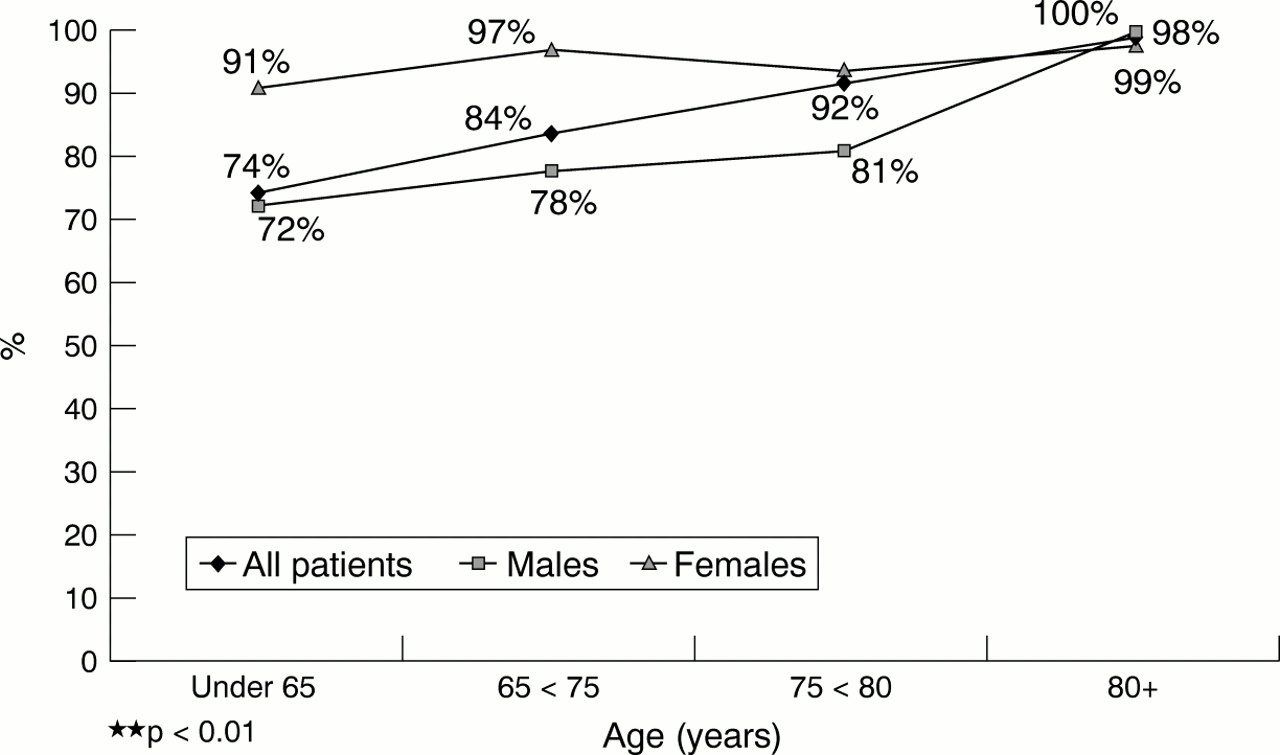
One hundred patients were referred for cardiac catheterisation and angiography. We analysed only patients for whom cardiac catheterisation was indicated, without contraindications, including relevant comorbidity, using ACC/AHA criteria for angiography (n = 320). A large proportion (83% (266)) of all these 320 patients who fulfilled the ACC/AHA criteria did not receive cardiac catheterisation, across all age groups. Thus, just 17% (54) were referred for catheterisation. There was a significant decline after age 65 in the proportion of patients receiving cardiac catheterisation where indicated: 26% (36) of those aged < 65 were referred compared with 16% (14) of those aged 65–75, 8% (3) of those aged 75–80 and 2% (1) of those aged over 80 (p < 0.01). Women were also less likely than men to be referred for this procedure where indicated: 25% (49):4% (5), respectively (p < 0.001). The trends are shown in fig1.
{kind=link}
Patients who were not given cardiac catheterisation and met the ACC/AHA criteria (%)
Logistic regression analyses were carried out, with cardiac catheterisation or angiography as the dependent variable, and age, sex, De Bono clinical priority score, Parsonnet 2 (without the age weighting) risk score, and specialty of entry as the independent variables. Age, sex, and de Bono clinical priority score were significant, independent predictors of cardiac catheterisation. Table 3shows that the odds of undergoing cardiac catheterisation were multiplied by 0.96 for each additional year of age, thus indicating a decrease by age. The odds of a man undergoing a cardiac catheterisation were 5.33 times the odds of a woman undergoing the procedure. The odds of undergoing a cardiac catheterisation were multiplied by 1.03 for each unit increase in de Bono clinical priority score (see table3).
Logistic regression of predictors of cardiac catheterisation (patients were with treated symptoms of ischaemic heart disease and met appropriateness criteria)
CORONARY ARTERY BYPASS GRAFTING
Of the 100 patients who were referred for cardiac catheterisation, just 24 were referred for CABG (four cases had missing data for the clinical priority and severity coding, thus 20 are analysed here), and two had PTCA.
Of the cardiac catheterisation patients, 18% (13) who were aged under 65 were referred for CABG compared with 24% (6) of those aged 65–75 and just one of the eight patients who were older than 75; 22% (18) of men and 11% (2) of women were referred. There were no differences with Parsonnet 1 or 2 risk scores or specialty and referral for CABG. The likelihood of receiving a CABG following catheterisation was greater for patients with a New Zealand clinical priority score of 35–54; 18% of those with a low score of < 25 and 15% of those with a higher score of 25–34 had CABG compared with 30% of those with a score of 35–54 (p < 0.05). None of the study patients achieved a New Zealand priority score of over 50. However, these results show that the majority of those in the high clinical priority group (70%) were still not referred. Of the study patients who underwent CABG, 50% achieved a high New Zealand clinical priority score of 35–54 (1–2 years' reduction in life expectancy) compared with 33% of those who did not get CABG. However, 50% of those who were denied CABG also met the clinical threshold of 25 recommended by the developers of the New Zealand scale for undergoing CABG. The row and column percentages are shown in table 4.
New Zealand clinical priority score by receipt of CABG
Referral for CABG was entered into a logistic regression model as the dependent variable, with age, sex, New Zealand clinical priority score, Parsonnet 2 risk score (without the age weighting), and specialty as the dependent variables. Table 5 shows that the odds of having a CABG was multiplied by 1.21 for each unit change in New Zealand clinical priority score. The remaining variables did not achieve significance in the model. However, the table shows that, while not significant, the odds of undergoing CABG were multiplied by 0.96 for each additional year of age (a figure comparable with that for age in relation to catheterisation, which did achieve significance), suggesting that the reduced sample size weakened the power of the study.
Logistic regression analysis of predictors of CABG
The local trust price for CABG in 1996–7 was £5238 per patient. Thus, the cost of providing CABG to the 21 patients with a New Zealand score of 35 or more who did not receive CABG would have been £109 998, and the costs of providing CABG to the 11 patients with a New Zealand score of 25–35 who did not receive CABG would have been a further £57 618.
Discussion
The analysis of more than 2000 hospital case notes presented here revealed that, despite indications for intervention identical to those of younger patients, older patients and women were, independently, less likely to undergo exercise testing and cardiac catheterisation. Lack of access to catheterisation inevitably limits their access to revascularisation procedures. Given the similarity of the indications for treatment between the younger and older men and women in this study and the lack of significant contraindications or comorbidities as a cause for these differences, it appears that that these patients were treated differently because of their age and sex. It is unknown whether this was because of valid clinical considerations that were not documented in patients' case notes, an age or sex bias, or simply a more cautious approach to treatment of older people and women, perhaps reflecting clinicians' more limited awareness of the evidence base for older people and older women, who have been generally excluded from major clinical trials.17 Reduced access to essential diagnostic testing where indicated, by age and sex, probably explains the lack of significant differences with age and sex and receipt of CABG among patients who had undergone cardiac catheterisation, although smaller sample sizes may also have been responsible.
A major strength of the present study is in its design: retrospective analysis of patients' case notes ensured that clinical practice was not influenced by the research process, thereby biasing and invalidating findings. However, the weakness of the study was also this reliance on retrospective case note analysis, with reliance on information documented in the notes. It is possible that relevant comorbidity and contraindications to tests and treatments were not fully documented by medical staff. It is, however, unlikely that omissions would have increased with the age of the patient or for women. It was unfortunately not possible to question clinicians retrospectively about their decisions not to intervene. The extent to which doctors are influenced by the visual cues their patients give them and that are unrecorded is unknown (for example, perceived frailty). Also, 10% of the case notes were not traced, despite three searches over 18 months. This untraced rate is within the range reported by other investigators and would be fairly small within diagnostic groups. It is therefore unlikely to be a source of significant sample bias. A final weakness of the study is also the single site design, with unknown external validity. It has been documented that the chances of receiving an intervention are greater with increased proximity of a patient's residence to a specialist centre.18 The results reported here showing low intervention and cross referral rates from a district general hospital are consistent with this. The intervention rates are likely to be at the lower end of the range of average clinical practice because, as the cardiac team openly acknowledged during the feedback of results, they were “low interventionist” cardiologists. The study is thus one of clinical practice in such a centre.
In New Zealand, in theory, all of those patients who underwent cardiac catheterisation with a score of 35 or more would have been placed on the waiting list for CABG. However, in the present study, 70% of those with a high New Zealand priority score of 35–54 did not receive CABG, and 85% of those with a lower New Zealand priority score of 25–34 (the clinically preferred threshold) did not receive CABG. This implies that the controversial priority scoring system in operation in New Zealand, despite criticism, is more equitable than UK practice as represented by this site, which is subject to individual clinician's thresholds and value judgements. The cost implications of redressing the inequities in service provision would, of course, be considerable.
Most work on clinical priority and risk scoring systems has been carried out in relation to cardiac services.6 ,19-21While none of the systems developed have 100% accuracy, the New Zealand priority scoring system for CABG is the most developed and is considered to be the best available, despite criticism.19 ,20 ,22 ,23 However, while it correlates strongly with the Ontario urgency score, it still underweights symptoms in its scoring system19. Consistency in assessment of urgency would be a step forward, especially given the evidence on variations between patients placed in the same waiting list priority categories in the UK when based on the subjective judgements of clinicians.24 Langham and colleagues25 argued that a two stage scoring system is preferable, which would select those who are likely to benefit from surgical intervention and then allocate an urgency score related to risk of immediate adverse events.
The Royal College of Physicians has stated: “in assessing the ability to benefit from treatment, chronological age is less important than other factors concerned with the biological ageing process and the presence of associated disease.”26 Efficacious treatments have their greatest impact when applied to patients at with the greatest risk.27 Although older patients are at higher risk of acute myocardial infarction and other cardiovascular events, they are less likely to receive potentially beneficial investigations. Thus, differences with age of a patient result in a “care gap”—that is, the gap between the actual and optimal application of effective treatments to the whole population at risk.27There may be a tendency to select low risk and younger patients for intervention rather than those at high risk who would benefit most. Negative, and incorrect, assumptions are often made about the quality of life of older people28 and “ageist” attitudes are common both across society generally29 and in medicine, despite education.30
A growing body of research indicates that older people are more likely to have more severe coronary artery disease and to be treated less vigorously and less effectively than younger people, to be treated medically rather than surgically, to be denied access to cardiac facilities (including admission to coronary care units and to cardiac rehabilitation), and to be more likely than younger people to undergo emergency or urgent cardiac interventions.31-37 It has been suggested, on the basis of such literature, that implicit age based prioritisation policies are operating in health care.38
Trials and follow up studies that have included older people have reported that most of them are likely to experience substantial benefit from appropriate therapeutic and surgical cardiac interventions when risk factor comorbidity is absent.39-43 Some, however, continue to argue that surgical intervention is less beneficial (prognostically) in older patients—a view that is not supported by the evidence.43 While the risks of surgery (for example, stroke or death) increase with age, early mortality and major morbidity are still relatively low for cardiac surgery in older patients and there is potentially much to be gained prognostically. For example, in a non-randomised group of patients aged 65 years or older, the six year survival rate following surgery was 79% compared with a survival rate of 64% among the control group receiving medical treatment only.44 Among patients with triple vessel disease, the absolute mortality reduction was 28%. Combined data from the controlled trials in patients younger than 65 years found that survival at five years following surgery was 89.9% compared with 84.2% in the (medical) control group; this equated to a smaller (5.6%) absolute reduction in mortality.45 In a study of octogenarians undergoing cardiac surgery in the USA, although there were increased perioperative risks, the longer term gains were such that at three years after surgery, the survival of surgically treated patients at 71.2% was almost equal to that of similarly aged US citizens as a whole, at 73.4%.46 The literature, then, supports the benefits of surgical revascularisation for older people where indicated.47 Functional capacity and severity of premorbid conditions are more important than age in predicting survival and morbidity of patients. Coronary revascularisation can also improve the quality of life of older people, in comparison with medical treatments, although CABG and angioplasty both have different types of beneficial effects.48-51 The overall conclusions of the published literature on older people, then, are that the risks to the few are greatly outweighed by the benefits to the many. In fact, the benefits of CABG are greater with increased age because the symptoms of older people are more severe (possibly because older people often present in an atypical manner or because diagnosis and referral are delayed).34 ,47 From the point of view of efficiency of outcome, the case for treatment of older people is strong—and even stronger than that for young people in relation to prevention of heart disease.52 On the other hand, the benefits in terms of increased quality of life and length of life, as well as the impact of future life threatening morbidities (such as cancer) on efficiency and duration of benefit, have yet to be carefully investigated in the much longer term (for example, beyond five year follow up periods).
In conclusion, apparent inequities in service provision by age are likely to have several causes, but these are largely undocumented, beyond speculation, and merit further investigation.
Acknowledgments
We would like to thank Alison Abery for developing the earlier versions of the coding forms; Lee Marriott, Gillian Hoose, Dr Galia Sperber, and the medical students at UCL for their help with the coding and data entry; Dr Rosaire Gray for interpretation of angiogram films; the clinicians, trust executives, medical records managers, and staff for their assistance with accessing case notes; and Mr Conner Burke and Age Concern England for suggesting the study. University College London is a member of the MRC Health Services Research Collaboration. Funding body: NHS Executive, North Thames Regional Health Authority:Care of Older People Programme.