Article Text

Abstract
Objective To study the impact of resting heart rate and leisure time physical activity at middle age on long term risk of drug treated lone atrial fibrillation (AF).
Design Longitudinal cohort study of 309 540 Norwegian men and women aged 40–45 years examined during 1985–1999 followed from 2005 through 2009.
Setting Data from a national health screening programme were linked to the Norwegian Prescription Database (NorPD).
Patients The cohort comprised 162 078 women and 147 462 men; 575 (0.4%) men and 288 women (0.2%) received flecainide and 568 men and 256 women sotalol and were defined as patients with AF.
Interventions No interventions.
Main outcome measures The outcome was lone fibrillation defined by having at least one prescription of flecainide or sotalol registered in NorPD between 2005 and 2009. Cox proportional hazard regression models were used to assess time to first prescription.
Results The risk for being prescribed these drugs increased with decreasing baseline resting heart. Adjusted hazard ratio (HR) per 10 beats/min decrease in resting heart rate for flecainide prescription was 1.26 in men (95% CI 1.17 to 1.35) and 1.15 (95% CI 1.05 to 1.27) in women. Similar effects were seen for sotalol in men, but not in women. Men who reported intensive physical activity were more often prescribed flecainide than those in the sedentary group (adjusted HR=3.14, 95% CI 2.17 to 4.54).
Conclusions This population based study supports the hypothesis that the risk of drug treated lone AF increases with declining resting heart rate in both sexes, and with increasing levels of self-reported physical activity in men.
Statistics from Altmetric.com
Introduction
The majority of atrial fibrillation (AF) cases occurs among patients who have concomitant cardiovascular disease: hypertension, a history of heart failure, coronary artery disease, or valvular pathology.1 Physical exercise is an important measure to prevent these diseases. There are, however, a number of AF cases that lack evidence of structural heart disease—the patients with ‘lone AF’. These have a fair long term prognosis,2 and clearly differ from the general AF population.
In 1998, a Finnish study of high ranking male orienteers showed an association between exercise and AF.3 Several subsequent studies have confirmed these results by comparing the prevalence of AF in top athletes versus various control groups.4 ,5 The findings of two population based cohort studies,6 ,7 which more likely reflect the general population, were less consistent. The American Physicians’ Health study, comprising 16 921 healthy men originally recruited from among more than 200 000 American physicians, suggested a dose–response relationship between strenuous physical activity and risk of AF. The risk of AF increased by >50% among high intensity exercisers aged below 50 years.6 However, another US cohort comprising members of Medicare aged above 65 years did not show any significantly increased risk of AF with increasing levels of physical activity.7 A review of this topic from 1995 to 2011 showed that many of the previous studies are not directly comparable because of different definitions of physical activity and AF, and differences in study design and population composition.8 The most recent reviews, by Delise et al as well as Müller-Riemenschneider et al,9 ,10 critiqued the published studies on sport practice and AF. They concluded that there is no evidence to suggest an increased risk of AF in subjects with normal hearts. The evidence of resting heart rate, in addition to fitness, as a predictor of total mortality adds to this heterogeneity.11 The purpose of the present study was to investigate the impact both of resting heart rate and self-reported leisure time physical activity on the risk of lone AF in the general population, based on data linkage between the nationwide age-40 programme with more than 300 000 Norwegian men and women and the Norwegian Prescription Database (NorPD) using the prescription of flecainide or sotalol as proxy for paroxysmal and persistent lone AF.
Methods
The age-40 programme
From 1985 to 1999, Norwegian health authorities conducted a screening programme among women and men aged 40–42 years in 18 Norwegian counties. The programme was based on regular visits by a health examination team to all municipalities, every third year. All residents aged 40–42 years were invited, and a few counties also included a broader age range.
Details on study procedures have been published previously.12 Height, weight, resting heart rate, and blood pressure were measured. Participants were also asked to fill out a questionnaire about their lifestyle and previous and current illness. All surveys were carried out by trained personnel from the National Health Screening Service, now incorporated into the Norwegian Institute of Public Health. Information about education was obtained from Statistics Norway (http://www.ssb.no/en/), while information on medication was retrieved from NorPD via record linkage using the 11 digit encrypted unique person identification number assigned to all persons living in Norway.13 Record linkage was approved by the Norwegian Data Inspectorate and the Regional Committee for Medical Research Ethics.
Study sample
Our main study sample comprised men and women aged 40–45 years at the time of screening (1985–1999), with valid information on resting heart rate and relevant covariates such as height and weight, level of education and self-reported smoking habits, and with no registered prescription of flecainide or sotalol in 2004. We performed additional analyses including only the 233 784 ‘heart healthy’ individuals reporting no cardiovascular disease at screening (ie, self-reported previous myocardial infarction or angina pectoris) and with no cardiovascular prescription drugs dispensed in 2004.
Exposure
The main exposure variables were resting heart rate recorded at baseline and self-reported level of leisure time physical activity. Resting heart rate, and systolic and diastolic blood pressures were assessed by DINAMAP (Criticon, Tampa, USA), which measured the blood pressure and heart rate automatically by an oscillometric method. After 2 min of rest, three recordings were made at 1 min intervals. Mean values of the second and third measurements were used in the present study. Participants were asked to tick ‘YES’ on the questionnaire beside the most fitting description of their leisure time physical activity level. If activity varied a lot—for example, between summer and winter—they were asked to give an average covering the previous 12 months. The four mutually exclusive response categories were:
-
Sedentary: reading, watching TV, or other sedentary activity
-
Moderate: walking, cycling, or other forms of exercise at least 4 h per week (including walking or cycling to the workplace, Sunday walking, etc)
-
Intermediate: participation in recreational sports, heavy gardening or similar activities for at least 4 h per week
-
Intensive: Participation in hard training or sports competitions, regularly and several times per week.
Health outcomes
The main outcome was paroxysmal or persistent lone AF defined as having at least one prescription of flecainide or sotalol registered in NorPD between 1 January 2005 and the end of the follow-up in 31 December 2009. NorPD includes prescription data from the entire population in Norway since 2004. It contains information on all prescriptions dispensed at pharmacies, regardless of whether they were reimbursed or not. Patient identity is strictly protected through encryption. The drugs are classified according to the Anatomical Therapeutic Chemical (ATC) classification system.14 Data included in the present analyses are: the patient's unique identifying number (encrypted), sex, age, date of dispensing, and drug information (ATC code). Information on dispensing of flecainide (ATC code C01BC04), sotalol (C07AA07), and other cardiovascular drugs (ATC group C) was included.
Other variables
Based on their potential status as risk factors for AF, and also because they are factors that may influence resting heart rate and level of leisure time physical activity, we included the following variables measured or registered at the time of screening as confounders: self-reported previous myocardial infarction or angina pectoris, body height, body mass index (measured as kg/m2), daily smoking (yes/no), education (low: primary or lower secondary; middle: higher secondary or high school; high: university/college), and age (years). We also included year of screening in the model. Bodyweight in kg and height in cm were measured according to a standard protocol. The possible confounding effect of underlying cardiovascular disease was further adjusted for in the analyses by including use of cardiovascular medicine during 2004 as an indicator in the multivariate model. We also performed separate secondary analyses of the ‘heart healthy’ group by excluding participants with self-reported previous myocardial infarction or angina pectoris or with at least one cardiovascular prescription drug (ATC group C) dispensed in 2004.
Statistics
In all analyses, we studied ‘new’ users of flecainide or sotalol, defined as patients who had no prescription of these drugs in 2004. In the first analysis, the time from 1 January 2005 to first prescription of flecainide was the outcome, whereas in a secondary analysis the time to first prescription of sotalol was used. The Cox model was used to model the association with resting heart rate and leisure time physical activity. The analyses were run for the two genders separately. When testing for interaction with gender, both genders were included in the model. Participants were censored at time of death, emigration or end of follow-up by 31 December 2009, whichever came first. Dates of death and emigration were obtained from the National Population Register.
Results
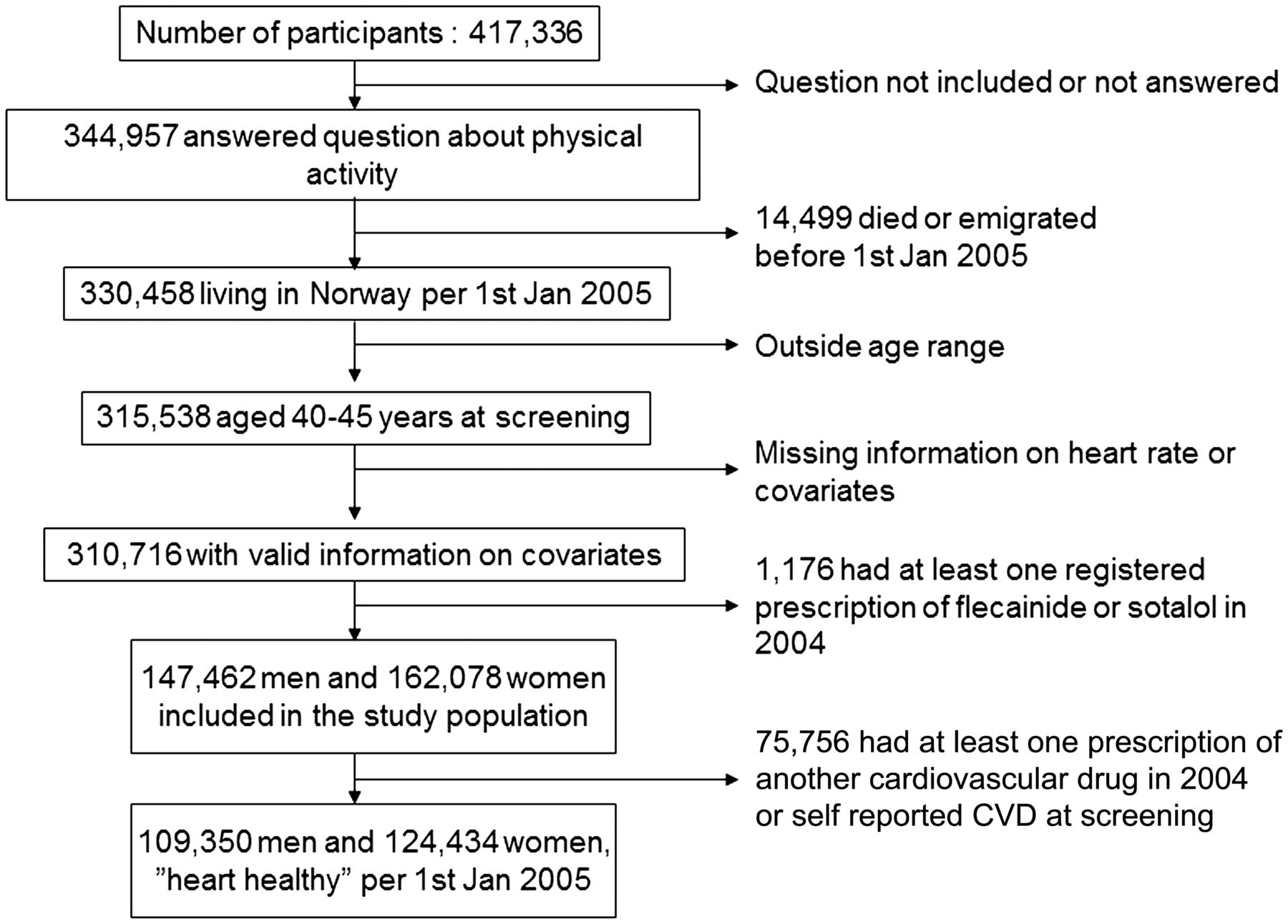
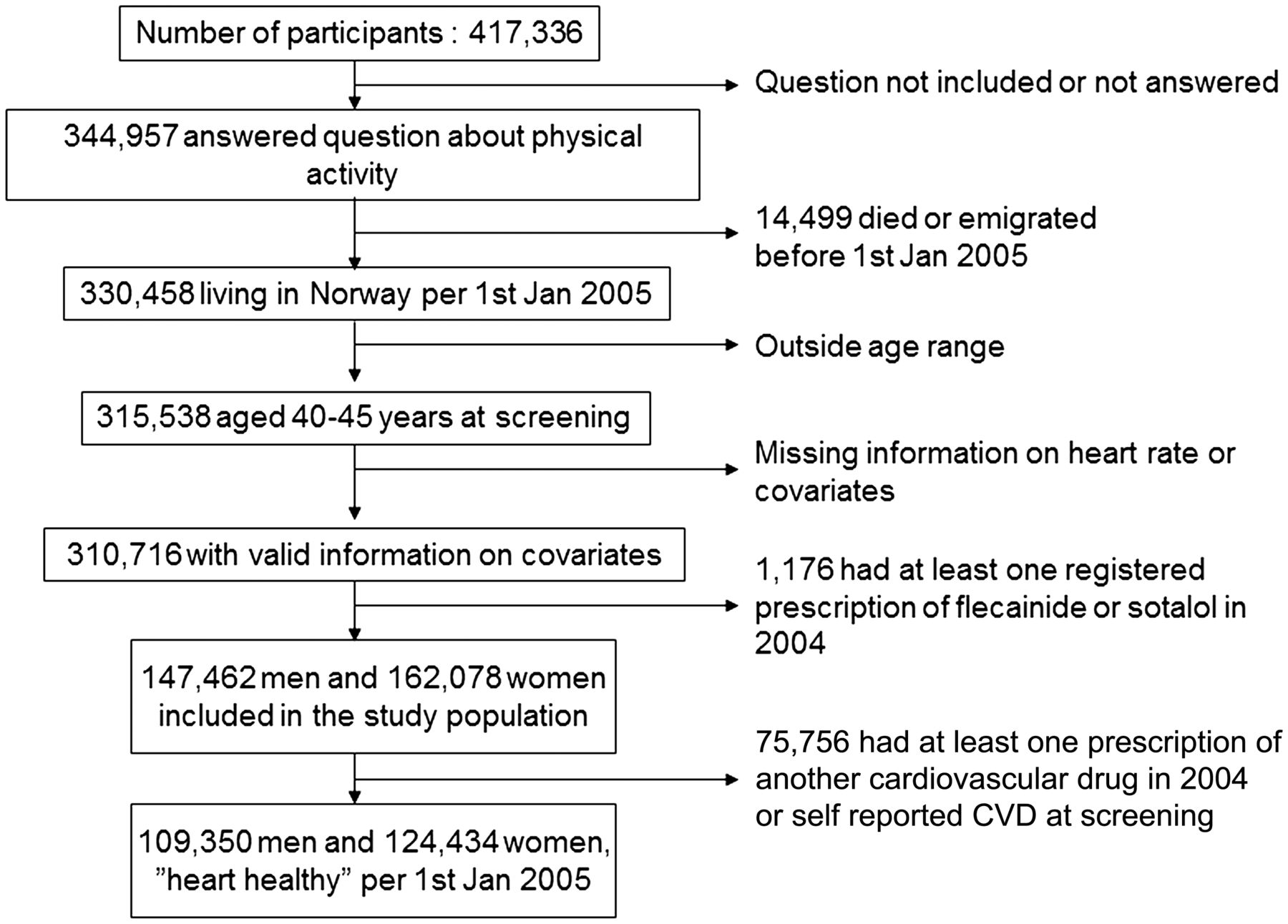
The total number of individuals who participated in the screening was 417 336. Participation rate declined over time, from 81% in 1985 to 52% in 1999, with an average participation rate of 70% for the entire period. Our main study sample consisted of 147 462 men and 162 078 women (figure 1). There were 233 784 ‘heart healthy’ individuals. The average age at screening was 41.4 years in our study population. Table 1 shows the baseline characteristics of the participating men and women, and the distribution of possible confounders. Women had a lower frequency of intensive and intermediate leisure time physical activity and a higher heart rate than men.
Baseline characteristics of 147 462 men and 162 078 women aged 40–45 years at screening (age 46–62 years at 1 January 2005)
{kind=link}
Flowchart showing the total number of participants in the screening 1985 to 1999, and the subsequent exclusions ending with 309 540 subjects aged 46–62 at start of follow-up, and eligible for the present analysis. CVD, cardiovascular disease.
A total of 575 (0.4%) men and 288 (0.2%) women were prescribed flecainide for the first time during follow-up (table 2). The risk of being prescribed flecainide increased gradually with decreasing heart rate in both genders. The crude hazard rate per each 10 beats/min decrease in heart rate was 1.29 in men and 1.12 in women. In a model including both genders a statistically significant interaction with gender was found (p=0.02). The hazard ratios remained virtually unchanged after adjustment for potential confounding variables. Restricting the sample to the ‘heart healthy’ gave similar results for flecainide among men.
Hazard ratios for first time use of flecainide and first time use of sotalol during 2005–2009, per 10 beats/min decrease in resting heart rate measured at baseline in 147 462 men and 162 078 women aged 40–45 years
The risk of being prescribed sotalol showed a weaker association with resting heart rate, with an adjusted hazard ratio of 1.12 in men and no association in women.
There was also a decline in heart rate with increasing level of leisure time physical activity; 76, 74, 69, and 62 beats/min in the various activity categories among men, and 79, 77, 74, and 69 beats/min among women. The percentage of flecainide users increased gradually by increasing level of physical activity in men (table 3; p value for trend <0.001). No such association was seen in women. Adjustment for covariates had a minor impact on hazard ratios for leisure time physical activity among men. Men reporting intensive activity were also at increased risk of using sotalol (data not shown).
Hazard ratios for first time use of flecainide during 2005-2009 among 162 078 women and 147 462 men aged 40–45 years, by leisure time physical activity at baseline
The effect estimate for heart rate remained virtually unchanged when adjusting for physical activity in men, from 1.26 to 1.21, whereas adjusting for heart rate on the effect of physical activity reduced the estimate for intensive activity from 3.14 to 2.54.
Discussion
This population based longitudinal study showed that the risk of being prescribed flecainide—an antiarrhythmic drug mainly used for prevention of recurrence of lone AF—increased with decreasing resting heart rate, both in men and women. The risk of being prescribed flecainide also increased with increasing level of self-reported leisure time physical activity among men. The findings are robust and remained unaffected by adjustment for several confounding factors.
The present study is as far as we know the first study to analyse both heart rate and level of leisure time physical activity as risk factors for AF. Our results suggest that low resting heart rate and high physical activity are both associated with AF without structural heart disease.
A number of studies suggest that athletes are more prone to AF, although some controversies exist.3–9 The differing conclusions in the literature on the relationship between endurance physical activity and AF8 ,9 may be due to heterogeneity of the study populations. To avoid such confusion we restricted our AF cases to middle-aged people with lone AF.
The present data does not permit analysis of pathophysiological mechanisms. However, a likely causal chain is that physical activity is related to heart rate, and that lower resting heart rate increases the risk of lone AF. Adjusting for heart rate on the effect of physical activity in men reduced the estimates, which is to be expected. This corresponds with Grundvold et al who recently demonstrated that among presumably healthy middle-aged men, a heart rate of <100 beats/min during a 100 W exercise load conferred a 60% higher risk for future AF compared to those who attained faster heart rates at this low exercise load (personal communication, 2013). In a recent analysis from the Copenhagen Study where the emphasis was risk of death associated with resting heart rate, they adjusted for fitness, but not the other way around.11 In our study the effect of heart rate was only slightly reduced when taking physical activity into account, suggesting that heart rate is closer to the pathophysiological mechanism.
Patient groups with lone paroxysmal and persistent AF are heterogeneous; some have arrhythmia mainly at rest, others upon adrenergic stimulation during exercise, and many have no distinct pattern. The balance between parasympathetic and sympathetic activity is considered to be involved both in the initiation and maintenance of AF, as supported by the fact that catheter ablation targeting intrinsic cardiac ganglia may increase the success rate of AF ablation.15 An increased vagal tone shortens the atrial refractory period facilitating re-entry circuits in the atria, and bradycardia increases stroke volume, augments myocyte stretch and facilitates increased automaticity, all favouring AF induction.16
The major weaknesses of our study are the use of drug treatment as proxy for AF, and the fact that heart rate and physical activity were only assessed at one point in time and with a considerable time lag between health examinations and start of follow-up. From the NorPD we find that 65–70% of the sotalol and flecainide prescriptions are attributed to AF and/or flutter, 25% to ‘arrhythmia not otherwise classified’, and the rest to paroxysmal tachycardia. The potential misclassification most likely underestimates the effects.
In Norway, the drugs used for rhythm control of AF in the study period include flecainide, sotalol, disopyramide, and amiodarone. The prescription of disopyramide is minimal (<3% of all patients using class I antiarrhythmics13), and amiodarone is little used for lone AF. The access to catheter ablation for AF was limited in the study period. Flecainide has proarrhythmic effects that may increase mortality in patients with structural heart disease, and is therefore contraindicated in patients with underlying heart disease.17 In Norway, this drug treatment must be initiated by a specialist in internal medicine or cardiology. Consequently, almost only lone AF patients will be prescribed flecainide.
Sotalol is a non-selective β-adrenoreceptor blocking agent with both class II and class III antiarrhythmic properties. Its main indication is also prevention of recurrent AF, which has been best documented in patients with concomitant coronary heart disease, but the drug also has some use in the treatment of ventricular arrhythmias. Hence the sotalol group is less pure with respect to lone AF. This fits well with our observation that the relationship between exercise and drug use was stronger for flecainide than for the sotalol group.
The NorPD covers the entire Norwegian population, and all those having these drugs dispensed during the follow-up period were registered. The outcomes are thus virtually complete. In our main analysis, we excluded 1177 subjects with prevalent use of flecainide or sotalol in 2004, in order to capture only new cases of drug treated AF as the outcome. We did, however, include these subjects in an additional analysis (data not shown), and the results were similar to those reported in this paper. We do not know the extent to which our estimates are affected by the lack of inclusion of cases with asymptomatic AF and those who had symptoms, but who did not seek medical advice in Norway. Physically active individuals might more often seek medical advice for symptoms of AF. However, active people might also prefer to avoid the ‘sick role’ and medication. Because flecainide only modestly reduces heart rate and does not affect exercise capacity, it is the preferred drug among physically active AF patients.18 However, using sotalol as the outcome gave similar results.
Heart rate was measured in a standardised way in all studies using the same staff and equipment.12 Repeated heart rate measurements at 10 year interval have been shown to be relatively strongly correlated,19 supporting the use of one single assessment even after a long time interval. The physical activity questionnaire was developed by Swedish physiologists during the 1960s.20 ,21 This questionnaire has shown consistent validity over time, also in terms of its predictive power for chronic disorders as varied as coronary heart disease and breast cancer.22–24 Furthermore, level of physical activity at baseline was associated with resting heart rate. Similar relations between resting heart rate and physical exercise capacity have also been described previously.25 Tracking of physical activity was assessed in the Tromsø study, where repeated examinations after 7 and 28 years showed that a higher than expected proportion of subjects maintained their physical activity level.26 Being physically active in young adulthood increased the odds of being physically active later in life. We therefore conclude that even if physical activity levels and resting pulse are measured only at baseline and may change over time, this is more likely to underestimate the effects than to create other systematic errors.
The lack of an association between leisure time physical activity and AF in women is intriguing, but the finding may be due to lack of power since we had few female cases. This is supported by the consistent finding regarding heart rate and lone AF in the two genders. The clearly lower effect estimates in women than men also suggest that there are physiological and anatomical differences—for example, in heart size—that may influence the risk of AF as well as clinical presentation.27 ,28
The major strengths of this population based study are: (1) the total coverage of the study population via the NorPD, which secures a complete follow-up regarding the defined outcome variables; (2) the magnitude of the study cohort with high attendance rate and its longitudinal design; and (3) standardised information on the exposure and possible confounding factors.
This population based study supports the hypothesis that the risk of drug treated lone AF increases with declining resting heart rate in both sexes, and with increasing level of self-reported physical activity in men. Future studies should devote more attention to training frequency, duration, intensity, the type and total volume of training, as well as vulnerable age periods and genetic vulnerability as plausible risk factors.29 ,30
References
Footnotes
-
Contributors DST and KG had the original idea and have been active in writing the manuscript. RS was the main statistician together with AT, and also took an active part in writing the manuscript. SS was responsible for retrieving data from the Prescription database, and contributed in writing the manuscript. SG-I, AJ, and WN were all involved in planning and writing the final manuscript. DST, KG, RS and WN are the main authors responsible for the overall content.
-
Competing interests None.
-
Ethics approval Norwegian Data Inspectorate.
-
Provenance and peer review Not commissioned; externally peer reviewed.