Article Text

Abstract
Background Sedentary behaviour is associated with risk of depression. We review and quantitatively summarise the evidence from observational studies in a meta-analysis.
Methods We searched the PubMed, Web of Knowledge, Chinese National Knowledge Infrastructure and Wanfang databases for observational studies related to the association of sedentary behaviour and depression risk up to 15 January 2014. Summary relative risks (RRs) were estimated by the use of a random effects model.
Results Thirteen cross-sectional studies with 110 152 participants and 11 longitudinal studies with 83 014 participants were included in this meta-analysis. The summary RR of depression for the highest versus non-occasional/occasional sedentary behaviour was 1.25 (95% CI 1.16 to 1.35, I2=50.7%) for all included studies. The pooled RRs of depression for sedentary behaviour were 1.31 (95% CI 1.16 to 1.48) in cross-sectional studies and 1.14 (95% CI 1.06 to 1.21) in longitudinal studies. In subgroup analysis by different types of sedentary behaviour, the pooled RRs of depression were 1.13 (95% CI 1.06 to 1.21) for long-time TV viewing and 1.22 (95% CI 1.10 to 1.34) for prolonged computer or internet use.
Conclusions This meta-analysis of observational studies indicates that sedentary behaviour is associated with increased risk of depression.
- Epidemiology
- Psychology
Statistics from Altmetric.com
Introduction
Sedentary behaviour typically refers to activities of less than 1.5 metabolic equivalent units and can operationally be defined as sitting or lying down like watching television or working at a computer.1 ,2 Sedentary behaviour is distinct from physical inactivity (ie, not meeting sufficient levels of moderate-to-vigorous physical activity).3 Opportunities for sedentary behaviour are ubiquitous and US adults spend 50–60% of their day in sedentary pursuits.4 Thus, even small adverse health effects of this behaviour may have profound effects at the population level.5–7
Depression is a major mental disorder. By 2020, depression is predicted to be the second leading cause of disability, immediately behind cardiovascular diseases.8 Observational studies have investigated the association between sedentary behaviour and depression, and the results were inconsistent.9–28 A prospective study reported that long-time TV viewing (≥6 vs <2 h/day) was related to higher risk of depressive symptoms.27 However, another prospective cohort study showed no significant association between prolonged computer use (>4 vs <2 h/day) and depression.26 Other studies about the association between sedentary behaviour and the risk of depression have also provided conflicting results.9–25 ,28
Therefore, we systematically conducted a meta-analysis by combining all available data of observational studies to: (1) derive an estimation of the association between sedentary behaviour and depression; (2) explore the potential between-study heterogeneity and (3) investigate the potential publication bias.
Materials and methods
Literature search strategy
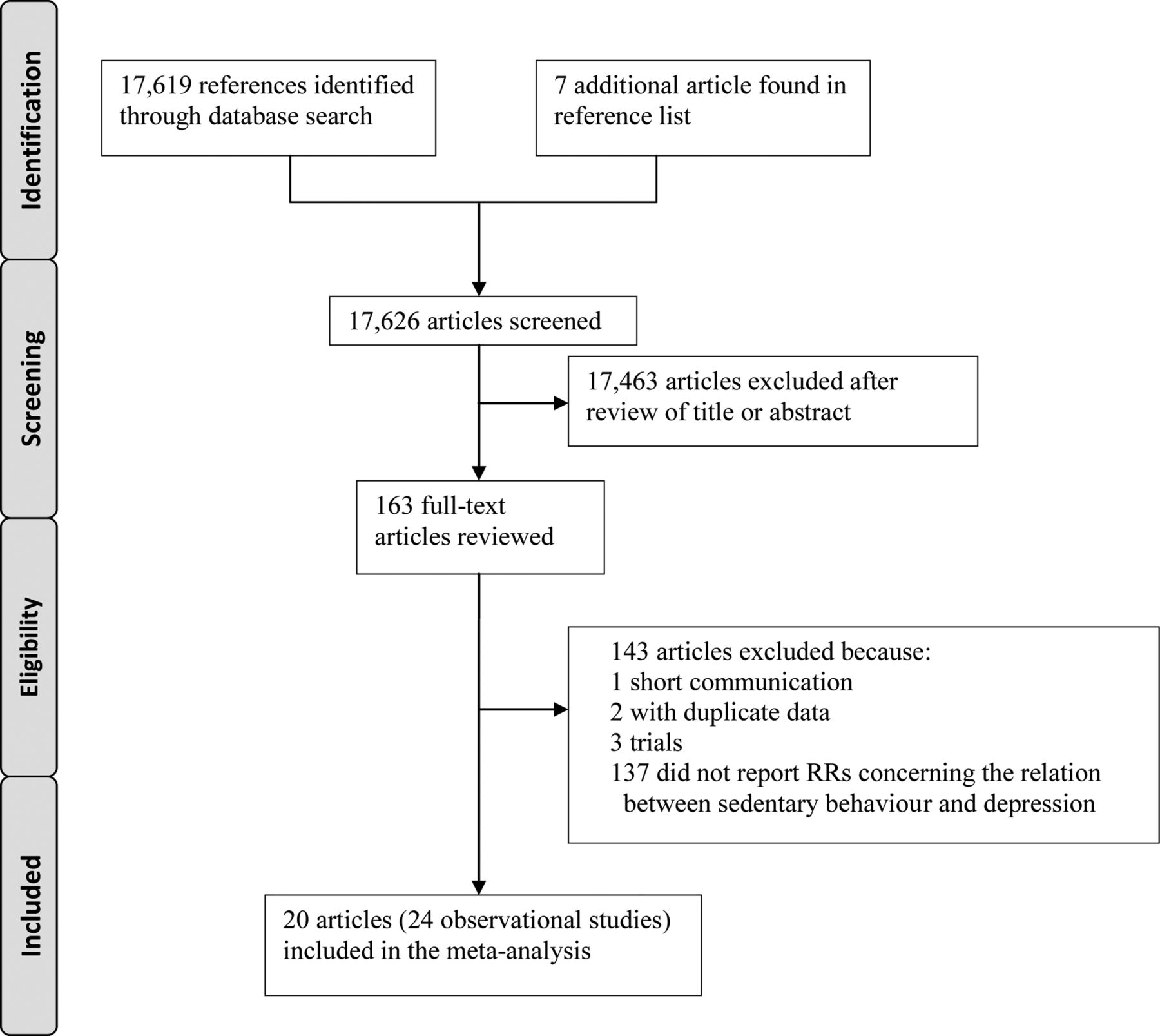
We followed the PRISMA guidelines.29 The available published studies reported in English or Chinese were identified by extended computer-based searches from PubMed, Web of Knowledge, Chinese National Knowledge Infrastructure and Wanfang databases up to 15 January 2014. Search terms included inactivity, computer use, sitting time, television viewing, screen time, media use, car driving and sedentary behaviour combined with depression and mental health. We also reviewed the reference lists from retrieved articles to identify additional studies not captured by our database search. The detailed steps of the literature search are shown in figure 1.
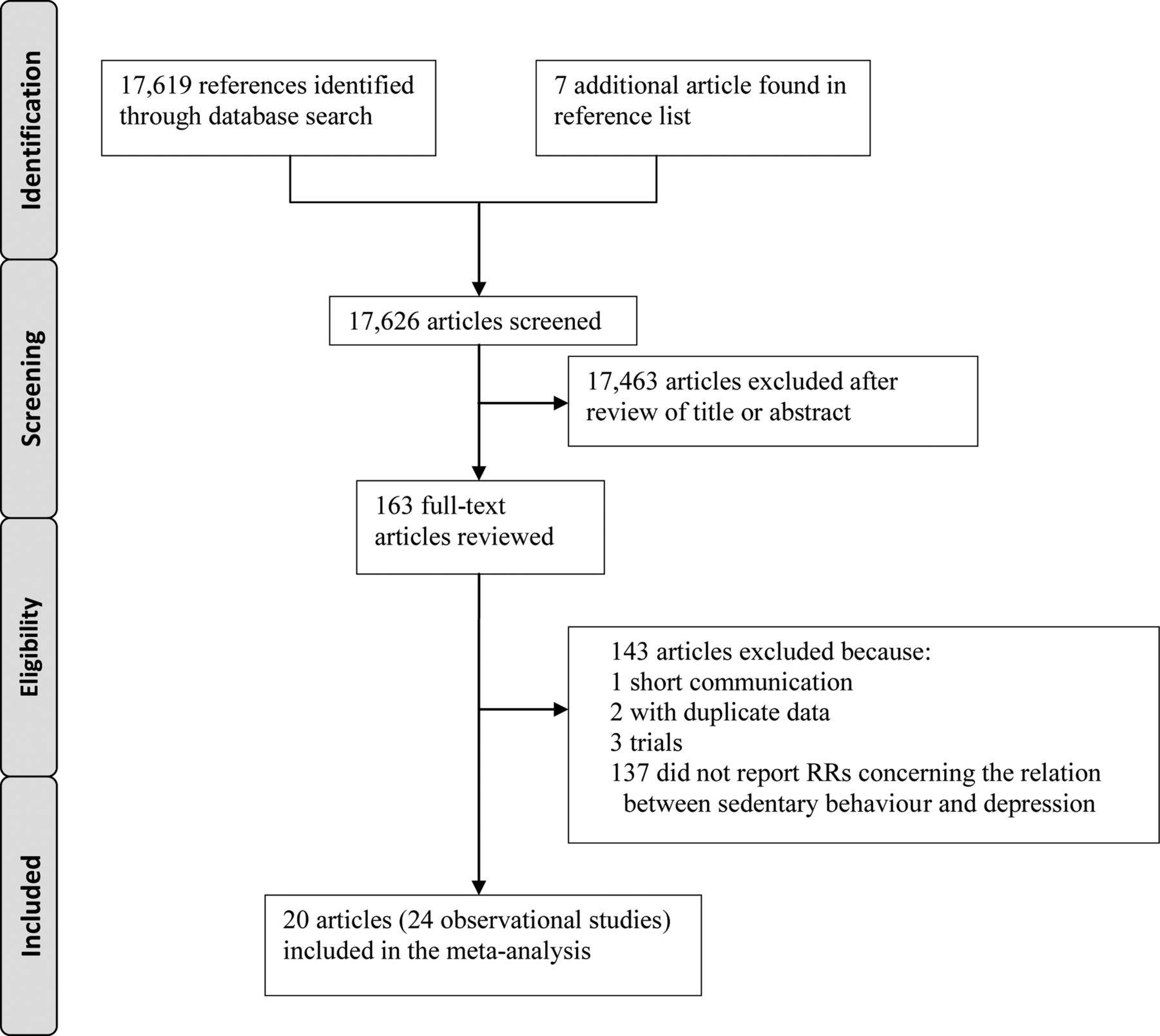
Flow of the literature (RRs, relative risks).
Inclusion criteria
The inclusion criteria were as follows: (1) observational studies published as an original study to evaluate the association between sedentary behaviour and risk of depression, (2) relative risks (RRs) with 95% CIs (or data to calculate these) were provided. Depression was defined as reporting a doctor's diagnosis of depression, beginning regular use of antidepressant medication, or identified by interview or depression rating scales. Studies examining general mental well-being or psychological distress rather than depression were excluded. If one data from the same population had been published more than once, the most recent and complete studies were chosen. Two investigators searched articles and reviewed all retrieved studies independently. If the two investigators disagreed about the eligibility of an article, it was resolved by consensus.
Data extraction and quality assessment
The following data were extracted from each study: the first author's last name, publication year, source of population, country where the study was conducted, study design, sample size, age at baseline years, sedentary behaviour measurement, depression ascertainment, sedentary category, RRs and 95% CIs and variables adjusted for in the analysis. We extracted the unadjusted RRs and RRs adjusted with the most confounders in the original studies. Data were independently extracted by two investigators with disagreements resolved through discussion. Inter-reviewer agreement was assessed using the kappa statistic, and the data were reviewed by a third investigator. The study quality was assessed using the Newcastle-Ottawa quality assessment scale (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp).
Statistical analysis
We weighted the study-specific log relative risks by the inverse of their variance to calculate a summary estimate and its 95% CI. The DerSimonian and Laird random effects model was used to combine study-specific RRs (95% CIs), which considers both within-study and between-study variation.30 The Wilson and Lipsey random effects model was also included to strengthen the analytical model by comparison.31 Non-occasional/occasional sedentary behaviour was regarded as the reference category. For studies14 ,20 ,25 ,27 that did not choose non-occasional/occasional sedentary behaviour as the reference category, we used the floating SE32 ,33 to recalculate RRs. I2 of Higgins and Thompson was used to assess heterogeneity among studies34 and I2 values of 0%, 25%, 50% and 75% represent no, low, moderate and high heterogeneity,30 respectively.
Univariate and multivariate meta-regression analyses by study quality, study design, study region, number of participants and whether adjusted for physical activity were conducted to investigate the potential sources of heterogeneity. The leave-one-out sensitivity analysis35 was carried out to evaluate the key studies that have a substantial impact on the between-study heterogeneity.
Publication bias was assessed with visual inspection of the funnel plot and Egger's test.36 We also conducted subgroup analyses by study region (Europe, America, Asia and Australia), study design (cross-sectional studies and longitudinal studies), type of sedentary behaviour (television viewing and computer or internet use), whether adjusted for physical activity (yes and no) and type of depression ascertainment (diagnosis and scales or questionnaires). All statistical analyses were conducted by Stata V.12.0 (Stata Corp, College Station, Texas, USA). A two-tailed p<0.05 was considered statistically significant.
Results
Literature search and study characteristics
We identified 17 619 articles by our literature search, of which 17 463 were excluded after review of titles or abstracts (figure 1). Seven additional articles11 ,12 ,14 ,17 ,20 ,24 ,37 were found in reference lists of retrieved studies. We reviewed 163 possibly relevant articles in full text. One short communication, two articles with duplicate data, three trials and 137 articles without RRs concerning the relation between sedentary behaviour and depression were excluded. Thus, 24 observational studies on 193 166 participants from 20 articles9–28 were included in the analysis (see online supplementary table S1).
Overall, 13 studies were cross-sectional11 ,12 ,14 ,16–21 ,24 ,25 and 11 studies were longitudinal.9 ,10 ,13 ,15 ,22 ,23 ,26–28 With regard to the study region, 2 studies were conducted in Australia,19 ,28 4 in Asia,16 ,17 ,21 ,25 7 in America11 ,12 ,14 ,22–24 and 11 in Europe.9 ,10 ,13 ,15 ,18 ,20 ,26 ,27 Four studies11 ,15 ,22 ,23 used the physician's diagnosis (or beginning regular use of antidepressant medication) as depression ascertainment and 19 studies9 ,10 ,12–14 ,16–21 ,24 ,26 used scales or questionnaires, while in one study28 depression was assessed by interview. The major adjustment confounding factors included age, gender, race, education, social class, smoking, alcohol use, body mass index and physical activity. The kappa statistic ranged from 0.69 to 1 (median 0.84). Quality assessment showed that the Newcastle-Ottawa score of each study was not less than 7, indicating that the methodological quality was generally good (see online supplementary table S2).
Highest versus Non-occasional/occasional analysis
Ten of all included studies showed a significant association between sedentary behaviour and depression10–12 ,14 ,15 ,18 ,19 ,21 ,22 ,27; while the other 14 studies indicated no relation between them.9 ,12 ,13 ,16 ,17 ,20 ,23–26 ,28 The pooled RR of overall data was 1.25 (95% CI 1.16 to 1.35) for the highest versus non-occasional/occasional sedentary behaviour, with moderate heterogeneity (I2=50.7%, Pheterogeneity<0.01) (figure 2). Results from the Wilson and Lipsey random effects model were identical (data not shown).

Forest plot for the pooled relative risk of depression (RR, relative risk).
Meta-regression and subgroup analyses
As seen in figure 2, moderate heterogeneity (I2=50.7%, Pheterogeneity<0.01) among all included studies was demonstrated for sedentary behaviour with depression. p Values of univariate meta-regression analysis with the covariates of study quality, study design, study region, number of participants and whether adjusted for physical activity were 0.36, 0.18, 0.85, 0.28 and 0.004, respectively. In multivariate meta-regression, p values were 0.73, 0.49, 0.82, 0.30 and 0.04, respectively, for the covariates of study quality, study design, study region, number of participants and whether adjusted for physical activity, respectively. A joint test for all five covariates gave a p value of 0.17 indicating no evidence for their interactions. When we restricted the analysis to the 7 studies14 ,20 ,22 ,24 ,27 ,28 that adjusted for physical activity and 17 studies9–13 ,15–19 ,21 ,23 ,25 ,26 without modifying for physical activity, the heterogeneity decreased to 0% (Pheterogeneity=0.87) and 33.7%, (Pheterogeneity= 0.09), respectively.
Table 1 showed the results from subgroup analyses. Sedentary behaviour was associated with a statistically significant increased risk of depression in all subgroup analyses. For example, the pooled RRs were consistent for studies adjusting for physical activity (RR=1.12, 95% CI 1.06 to 1.18) and studies not adjusted for physical activity (RR=1.34, 95% CI 1.22 to 1.48). When we stratified studies by different types of sedentary behaviour, the pooled RRs of depression were 1.13 (95% CI 1.06 to1.21) for long-time TV viewing and 1.22 (95% CI 1.10 to 1.34) for prolonged computer or internet use.
Subgroup analyses of sedentary behaviour and depression risk
Sensitivity analysis
Two studies11 ,21 were found to be key contributors to this moderate between-study heterogeneity by the leave-one-out sensitivity analysis. After further excluding these studies, no heterogeneity (I²=0, Pheterogeneity=0.65) was found, and the pooled RR was 1.15 (95% CI 1.10 to 1.20).
In a sensitivity analysis, we pooled the unadjusted RRs from 16 studies.9 ,10 ,13 ,15–19 ,21 ,22 ,24–26 ,28 The pooled RR was 1.32 (95% CI 1.24 to 1.41) for the highest versus non-occasional/occasional sedentary behaviour, with low heterogeneity (I2=9.6%, Pheterogeneity=0.34).
Publication bias
The visual inspection of the funnel plot (figure 3) and Egger's test (p=0.20) showed no evidence of publication bias for all included studies.

{kind=link}
{kind=link}
{kind=link}
Funnel plot with pseudo 95% confidence limits for all included studies (SE, standard error).
Discussion
Before focusing in on depression, we note that sedentary behaviour is associated with numerous chronic diseases; a meta-analysis of 18 studies found that sedentary time was associated with an increased risk of diabetes, cardiovascular disease as well as cardiovascular and all-cause mortality.38
Sedentary behaviour is negatively associated with mental well-being39/health.40 ,41 Depression is a common form of mental distress.
Our meta-analysis included 24 observational studies with 193 166 participants. To the best of our knowledge, this is the first meta-analysis to quantitatively examine the association between sedentary behaviour and depression. We found a statistically significant association between sedentary behaviour and the risk of depression. The summary RRs (95% CIs) for depression did not substantially change in the sensitivity analysis and subgroup analyses by study region, study design, type of sedentary behaviour, whether adjusted for physical activity and type of depression ascertainment. There was no evidence of publication bias.
A biological rationale—loss of social engagement
Several hypotheses have been proposed to describe the association of sedentary behaviour and depression risk.42 One underlying explanation for our findings is that sedentary behaviour may displace physical activity, which has been found to be beneficial in reducing the risk of depression.43 Besides, social/psychological theories, such as the social withdrawal hypothesis, suggest that increased sedentary time may remove individuals from social interactions and thereby increase their risk for depression.44 Hence, people with heavy sedentary behaviour could spend less time on physical activity or social activities and are more likely to be depressed. Further studies in understanding the underlying biological mechanisms linking sedentary behaviour and depression are warranted.
Methodological considerations
Between-study heterogeneity is common in meta-analysis,45 and exploring the potential sources of between-study heterogeneity is the essential component of meta-analysis. Our meta-analysis showed moderate between-study heterogeneity. We used meta-regression and the leave-one-out sensitivity analysis that aimed to explore the potentially important causes of the between-study heterogeneity. Whether adjusted for physical activity was found to influence between-study heterogeneity. In subgroup analyses by studies adjusted for physical activity or not, the heterogeneity decreased to 0% (Pheterogeneity=0.87) and 33.7% (Pheterogeneity=0.09), respectively. Two studies11 ,21 were found to be key contributors to this moderate between-study heterogeneity by the leave-one-out sensitivity analysis. When we excluded these two studies, there was no heterogeneity (I²=0). After reducing the between-study heterogeneity, the results were found to be consistent with the one based on all studies, indicating that our results were stable and reliable.
A major strength of the present meta-analysis is the large number of participants included, allowing a much greater possibility of reaching reasonable conclusions. Second, nearly all included studies had adjusted for potential confounders, increasing the credibility of the results. Third, the relationship between sedentary behaviour and depression risk did not substantially change in sensitivity and subgroup analyses. The pooled RR of 11 longitudinal studies found a statistically significant positive association between sedentary behaviour and depression, which implied a potential causal relationship between them. Fourth, we found little evidence of publication bias in this meta-analysis, which indicated that our results were not affected by small-study effects.
However, the potential limitations of our study should also be considered. First, although the researchers had adjusted for some confounders, other potential confounding factors could not be ruled out completely. Second, the limited information provided in the included studies precluded the possibility of dose-response analysis. Third, as only three studies14 ,15 ,24 used objective measures for sedentary behaviour, the estimation of the true association between sedentary behaviour and depression risk could be influenced by misclassification.46 ,47 Finally, we must acknowledge and consider the possibility of reverse causation, that is, depression causing sedentary behaviour.
Clinical implications
In summary, results from this meta-analysis indicate that sedentary behaviour is associated with increased risk of depression. Physical activity is a distinct domain to sedentary behaviour (as outlined in the Introduction section), but it can contribute to reducing sedentary behaviour. A recent randomised trial of exercise reduced depression in older men.48 Reducing sedentary behaviour should be advocated for the primary prevention of depression.
What are the new findings?
This is the first meta-analysis investigating the association between sedentary behaviour and depression.
This meta-analysis indicates that sedentary behaviour might be positively associated with the risk of depression.
The results are stable and reliable after sensitivity and subgroup analyses.
How might it impact on clinical practice in the near future?
Reducing sedentary behaviour should be advocated for the primary prevention of depression.
More clinical trials are needed to reveal the internal mechanism of this association.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
Contributors LZ and DZ conceived the study and participated in its design and coordination. LZ and YZ carried out the literature search, data extraction and quality assessment. LZ and DZ were involved in the interpretation of the data, as well as in the drafting of the manuscript and its critical revision for important intellectual content.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.