Article Text

Abstract
Background: American and Australian studies indicate that domestic violence is common among patients attending for emergency care. It is not clear whether this applies to patients attending emergency departments in the UK.
Methods: A single centre cross sectional study. Adult patients attending the emergency department of Addenbrooke’s Hospital, Cambridge were interviewed in randomly allocated time blocks, using validated questions from a US study. Potential participants were excluded if they (1) were unwilling (2) had an altered mental status (3) had a companion who refused to leave (4) were too ill (5) were unable to speak English (6) personal contacts of the interviewer.
Results and Conclusions: 256 completed interviews were returned out of a possible 307 (84.8%). The incidence of domestic violence was 1.2% (95% CI 0.2% to 3.4%). The lifetime prevalence of domestic violence was 22.4% (95% CI 15.6% to 30.4%) among men and 22.1% (95% CI 15.1% to 30.5%) among women. The incidence and prevalence rates of domestic violence were considerably lower than in the US study, but similar to prevalence rates recorded in British community surveys. A significant association was found between reported domestic violence and reported deliberate self harm in women (odds ratio 75.4 95% CI 13.1% to 433.7). There was no significant association between higher use of medical care and domestic violence.
Interpretation: Domestic violence is common among patients attending for emergency care in the UK. There is a significant association between domestic violence and deliberate self harm in women, further work is required to see if this association is causal. Larger emergency department surveys are required to confirm these results.
- domestic violence
- epidemiology
- deliberate self harm
Statistics from Altmetric.com
A merican1 and Australian2 studies have shown that domestic violence is common among patients attending for emergency care. Domestic violence research is hampered by lack of an accepted definition. In this paper, domestic violence is defined as “illness or injury resulting from the deliberate actions of an intimate partner”. The definition is restricted to adults. Police reports suggest that domestic violence is a fact of life for millions of women in the UK.3 Evidence from the USA1 and Australia4 indicates that substantial proportions of patients who present in emergency departments are suffering ongoing domestic violence, but the data reported are not easily compared because the studies differ in terms of populations, data extraction, methods, and definitions. Domestic violence may often not be reported to health care professionals.1,5 While homicide by a partner is uncommon in Britain6 there are many health consequences of domestic violence. There is evidence from a Swedish cohort study that victims of domestic violence have increased use of medical care in all specialties, not just emergency care.7 There is also some evidence that victims of domestic violence are more likely to abuse their children.8
There has been little research in the UK on the epidemiology of domestic violence. The British Crime Survey is a continuing cross sectional community survey.9 The data have been re-analysed with a definition of domestic violence that includes physical and non-physical assault.3 This analysis found that 26% of women reported domestic violence at least once in their lifetime and 4.2% reported domestic violence within one year. Most of the studies on violence conducted in UK emergency departments relate to acute presentations of physical assaults.10–,12 These report much lower incidence rates of domestic violence than US studies.
The reported incidence (11.7% to 30%) and prevalence rates (about 50%) of domestic violence in US emergency departments appear much higher than published UK rates and do not accord with clinical experience.1,11,12 The principal aim of this study was to identify the incidence and prevalence of domestic violence among patients of both sexes attending a UK emergency department. Other aims were to test the hypotheses that reported domestic violence was associated with deliberate self harm, alcohol misuse, and increased use of medical care. Victims of domestic violence are more likely to report deliberate self harm than those who deny domestic violence, though the strength of this association has not been reported.1 It is not clear whether this association is causal or not. There is debate whether ongoing domestic violence is associated with alcohol dependence and if this association is causal.
METHODS
A cross sectional interview based survey was performed in the emergency department of Addenbrooke’s Hospital, University of Cambridge over a two week period in 2001. Patients were interviewed by a single interviewer during randomly allocated time blocks of six hours on consecutive days. Patients were approached after triage and asked to answer a few questions while they were waiting for treatment. To improve comparability with other studies, the questions about domestic violence were those used in a widely cited US study.2 These questions are well validated13,14 and inquire about physical and non-physical domestic violence and are similar to those used by the British Crime Survey.3 These questions had high internal consistency in the present study (Cronbach’s α=0.84.) The CAGE questionnaire was used to identify problem alcohol drinking.15 Deliberate self harm and use of medical care was assessed by direct report. All patients were interviewed alone. “Walking wounded” patients were interviewed in a separate room, where there was no possibility that they could be overheard. Trolley bound patients were interviewed in a cubicle. Any accompanying friends or relatives were escorted out of earshot. Refusal of friends or relatives to leave led to the interview being abandoned.
All patients more than 16 years old on the day of the interview, who registered as a patient at the emergency department and arrived inside a randomly allocated time block were eligible for inclusion in the study. Patients were not admitted to the study if they (1) had suffered a life threatening injury or illness that required immediate treatment, (2) had altered mental status of any cause (for example, dementia or alcohol intoxication), (3) were personal acquaintances of the interviewer, (4) had companions who refused to leave, (5) had been referred directly to another specialty by their general practitioner, but had been directed to wait in the emergency department.
Incident cases were those who gave affirmative answers to the questions “Are you here today because of injuries from your current partner?” and “Are you here today because of illness or stress related to threats, violent behaviour or fear from your current partner?”
Prevalent cases were those who reported abuse at any point in the past. Further questions found when abuse had most recently occurred.
Data were analysed using STATA statistical software, version 7. Student’s t test was used for continuous data. Unconditional logistic regression was used for multivariate analysis. Likelihood ratio tests were considered significant at the 5% level.
Ethical approval was sought and gained from the local research ethics committee.
Role of the funding source
The funding source of this research was not involved in the methods.
RESULTS
Response rates: 307 patients were eligible during the study period to be interviewed. Thirty two patients were classified as non-responders and five excluded because it was their second attendance. Table 1⇓ shows the reasons. Most patients who could not respond because of altered mental status were demented and living in residential care. The patients who were too ill did not appear to have illnesses or injuries resulting from acute domestic violence. All seven patients presented after cardiac arrests or road traffic accidents. The unwilling patients presented after deliberate self harm and may have suffered recent abuse. All three language difficulty patients were language school students who apparently fell off bicycles. Five questionnaires were excluded because they were repeat completions by multiple attenders. This left 270 questionnaires. There were 14 questionnaires with incomplete data. To check whether excluding those with missing data would be a source of bias, analysis was performed twice, once with these questionnaires included and once with them excluded.16 This made minimal difference, and this paper is based on results with incomplete results excluded. After questionnaires with missing data had been excluded, the response rate was 84.8%, 256 questionnaires from a possible 302.
Sample approached
The mean age of men attending the emergency department in the sample was 38.5 years and for women 47.6 years, a significant difference (p<0.001).
Figure 1⇓ shows the mean age of those reporting abuse.

Mean age of patients reporting abuse.
Men who reported abuse appeared younger than men who denied abuse, though this difference was not significant (t=1.2, p=0.16). Women who reported abuse were younger and this difference was significant (p<0.01).
Incidence and prevalence
Incidence
Three of 170 patients who reportedly had partners answered “yes” to one or both of the questions “are you here today because of illness or stress related to threats, violent behaviour or fears from your current partner?” or “are you here today because of injuries from your current partner?” Thus the incidence of acute domestic violence among patients with partners attending the emergency department is 1.8% (95% confidence intervals 0.3% to 5.1%). Out of the whole study sample of 256, the incidence is 1.2% (95% CI 0.2 to 3.4). If the non-responding patients who were unwilling to be interviewed were included as incident cases, then the incidence of acute domestic violence out of the whole sample would be greater, 6 of 256=2.3% (95% CI 0.9 to 5.0). None of those classified as incident cases in this study had domestic violence recorded by medical or nursing staff on case note review.
Prevalence
Table 2⇓ and figure 2⇓ show the prevalence rates. These are compared with the prevalence rates in the re-analysed British Crime Survey3 and the US study1 that used the same questions.
Prevalence rates

Incidence and prevalence of reported domestic violence among patients attending Addenbrooke’s emergency department.
Deliberate self harm and domestic violence
On inspection there appeared to be a relation between deliberate self harm and sex (effect modification) and so analysis was stratified by sex.
The association between reported domestic violence and reported deliberate self harm was examined in a logistic regression model. This adjusted for age, alcohol misuse, and various demographic variables (table 3⇓). There is a strong association between reporting domestic violence and reporting deliberate self harm.
Logistic regression model
Alcohol and domestic violence
There was a significant association between three or four affirmative responses on the CAGE questionnaire and reported domestic violence (odds ratio (OR)=3.2 (95% CI 1.3 to 8.2). This association was not significant when stratified by sex (male OR=1.7, 95% CI 0.6 to 4.8: female OR=0.8, 95% CI 0.12 to 5.2) This association was not significant when adjusted for deliberate self harm and socioeconomic status (OR=1.3, 95% CI 0.5 to 2.9). There was no significant association between one or more, or two or more affirmative responses on the CAGE questionnaire and reported domestic violence.
Domestic violence and use of medical care
We classified the number of medical visits into high or low on the basis of four or more visits to a doctor in the past year. Women were more likely to be high users of medical care than men (χ2=7.83, df=1, p<0.01). There was also a significant association between age and high use of medical care (χ2=17.02 df=6 p<0.01). There was no significant association between high use of medical care and reporting domestic violence (χ2<0.01 df=1 p=0.96). Logistic regression revealed there was no significant relation even when adjusted for age and sex (OR=0.7, 95% CI 0.3 to 1.6).
DISCUSSION
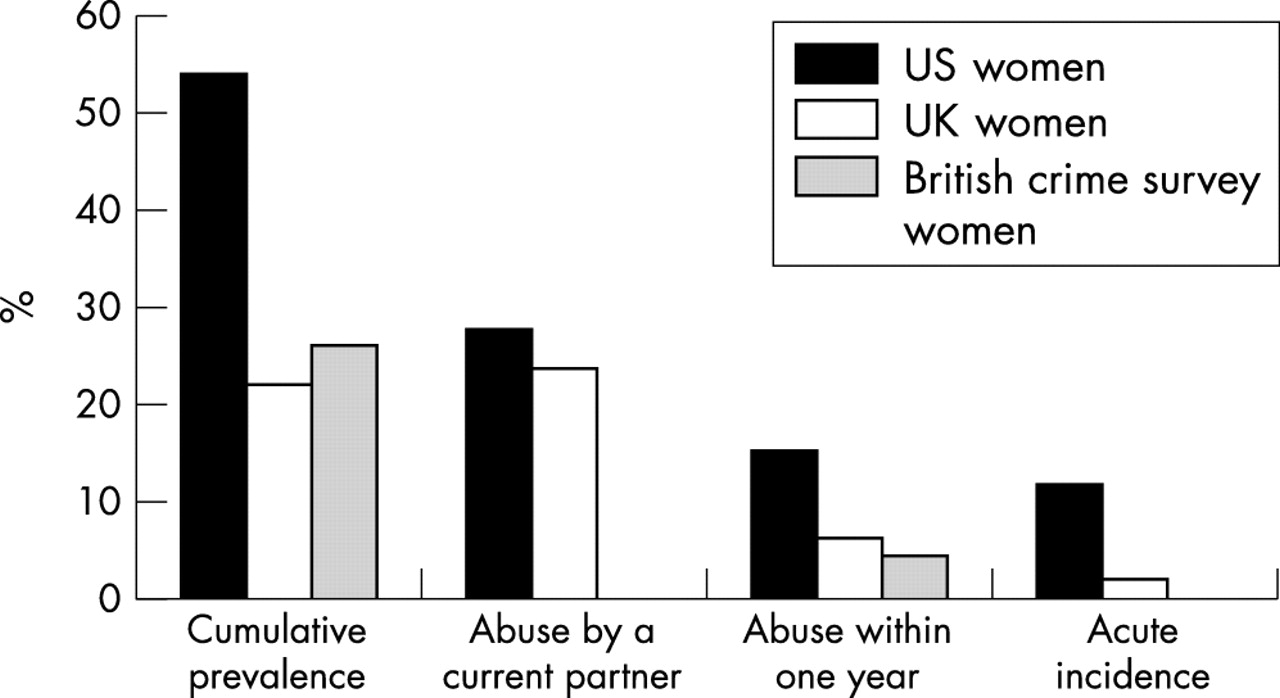
This is the first British prospective study to consider specifically domestic violence in emergency departments, though there are many studies that consider assaults and their aetiology.13,14,17 This study differs from these because the definition of violence used includes non-physical assaults, though threatening and controlling behaviour seem to correlate well with physical assault. This study also differs because it considers the prevalence of domestic violence. The incidence and prevalence of domestic violence seem to be considerably lower than in the US, although using the same questions and methods.1 (See fig 3⇓). The incidence of domestic violence in this survey is slightly higher than in previous UK studies. These differences probably relate to methodological differences11,17,18 The most conservative incidence was 1.2% among adults. This implies that an emergency department that has 55 000 patients of all ages attending a year would see about 500 adult patients a year suffering acute domestic violence. (Roughly one quarter of all emergency department patients are under 16). The prevalence of abuse by a current partner seems to be similar between the women in the American study and this study. The cumulative prevalence and prevalence of abuse within one year seem to be consistent with the re-analysed British Crime Survey data.3
{kind=link}
{kind=link}
{kind=link}
Reported abuse in the USA and UK.
Findings from a small survey carried out in a single department should be viewed with caution. The lower reported cumulative prevalence and prevalence of abuse within one year among women in Cambridge than women in Denver may be attributable to many reasons. There may be a reporting bias that women in the US are more prepared to volunteer a history of domestic violence than their UK counterparts. This bias may be exacerbated by having a male interviewer in the UK study. The women in the Cambridge study were older, (mean age 47.5) than the US study (median age 34.4). Both studies found that women who reported domestic violence were younger than those that denied domestic violence. This could be interpreted that domestic violence is becoming more common or that younger women are more prepared to report domestic violence but we cannot be certain that this is not just statistical variation. There may also be differential recall of events at different ages. The finding that the cumulative prevalence and prevalence of abuse within one year was similar to those in the re-analysed British Crime Survey suggests that the population attending emergency departments in the UK differ little from the community with respect to reported domestic violence. However, whatever incidence and prevalence rates are reported, they are likely to be underestimates. There is evidence that many victims of domestic violence will not report domestic violence even if asked by a health care professional.5
The prevalence rates were similar in both men and women. This is consistent with the British Crime Survey data,3 but at odds with work from Australia where women report higher rates of domestic violence than men.2 This may be attributable to the differing methodology used in these studies or may reflect a real difference in abuse between populations. A weakness of this study is that there is no measure of the severity of abuse. There is evidence that women tend to suffer more frequent and severe domestic violence than men but we did not measure the severity of injury. A cross sectional study in Bristol showed that similar proportions of female victims of assault were admitted to hospital as male victims of assault.18 However, victims of domestic violence differ very much from other assault patients and the severity of physical injury is only one part of a complex social disorder, which includes controlling behaviour, verbal humilitation, and sexual assault. The similar prevalence of domestic violence between men and women is unexpected and surprising. The measure of domestic violence used has no indication of the severity of domestic violence. The measure used may have less construct validity in men than in women. For instance, one of the questions concerns slapping. A man slapping a woman may have more intent to cause injury and harm than a (relatively weaker) woman slapping a man
There is a strong relation between reporting deliberate self harm and domestic violence in women but not in men with female self harmers being 75-fold more likely to report domestic violence than those who did not report deliberate self harm. This may be attributable, at least in part, to a reporting bias. Though this finding is consistent with case-control19 and retrospective cohort studies,7 none of these study designs eliminate reporting bias. It is plausible that suffering domestic violence leads to deliberate self harm. However, it is also plausible that reporting deliberate self harm is associated with personality traits that confer an increased risk of entering an abusive relationship. Another explanation might be that in interview these women may have blamed injuries on their partner although we have no evidence that this is the case. Cross sectional studies cannot easily establish the temporal sequence between deliberate self harm and domestic violence. The differing odds ratios between the sexes indicate effect modification with sex. If we assume that deliberate self harm is a consequence of domestic violence, then the much greater odds ratios might indicate that domestic violence is more severe among women.
The lack of significant association between reported domestic violence and two or more affirmative answers on the CAGE questionnaire, or three or more affirmative answers (adjusted) is unexpected, despite this association being found in some US studies.1,20 This may be because the sample is too small to detect a relation between alcohol dependence and domestic violence. Alcohol dependence may be a consequence of domestic violence, though the cross sectional and case-control studies that have looked at this cannot entirely eliminate recall bias.1,20 Acute assaults, regardless of aetiology, are associated with binge drinking.21–,23 The lack of a significant association between use of medical care and reported domestic violence is also unexpected but again is likely to be related to the power of this study. Significant associations with reported use of medical care were found with increasing age and female sex, consistent with previous work.24 Relying on self report may introduce measurement error, this may obscure any weak but significant association. This could be improved by a more objective measure of the use of medical care such as hospital case note and GP case note review. Such an approach may be useful in future research.
In conclusion, large proportions of both male and female patients attending emergency departments suffer ongoing domestic violence. This is often not disclosed to medical staff. The findings from this small single centre survey need to be confirmed in a larger study carried out across other emergency departments with diverse socioeconomic and demographic characteristics. The incidence and prevalence rates of domestic violence seem to be lower than in the US study1 and consistent with British Crime Survey data.3 A significant association was found between domestic violence and reported deliberate self harm. No significant association was found with either alcohol, high use of medical care, and domestic violence. Future work should also consider the severity of abuse and establish the temporal link between deliberate self harm and domestic violence.
This study needs to be replicated in different emergency departments and with interviewers of both sexes. In the meantime, emergency department staff need to be aware that domestic violence is common and often undisclosed.
Acknowledgments
Dr S Robinson facilitated the study.
REFERENCES
Footnotes
Funding: this work was supported by a Health Services Research grant from the NHS executive (Eastern).
Conflicts of interest: none declared.