Article Text

Abstract
The objective of this systematic review and meta-analysis is to examine which work-related risk factors are associated with specific soft tissue shoulder disorders. We searched the electronic databases of Medline and Embase for articles published between 2009 and 24 March 2016 and included the references of a systematic review performed for the period before 2009. Primary cross-sectional and longitudinal studies were included when outcome data were described in terms of clinically assessed soft tissue shoulder disorders and at least two levels of work-related exposure were mentioned (exposed vs less or non-exposed). Two authors independently selected studies, extracted data and assessed study quality. For longitudinal studies, we performed meta-analyses and used GRADE (Grades of Recommendations, Assessment, Development and Evaluation) to assess the evidence for the associations between risk factors and the onset of shoulder disorders. Twenty-seven studies met the inclusion criteria. In total, 16 300 patients with specific soft tissue shoulder disorders from a population of 2 413 722 workers from Denmark, Finland, France, Germany and Poland were included in the meta-analysis of one case–control and six prospective cohort studies. This meta-analysis revealed moderate evidence for associations between shoulder disorders and arm-hand elevation (OR=1.9, 95% CI 1.47 to 2.47) and shoulder load (OR=2.0, 95% CI 1.90 to 2.10) and low to very low evidence for hand force exertion (OR=1.5, 95% CI 1.25 to 1.87), hand-arm vibration (OR=1.3, 95% CI 1.01 to 1.77), psychosocial job demands (OR=1.1, 95% CI 1.01 to 1.25) and working together with temporary workers (OR=2.2, 95% CI 1.2 to 4.2). Low-quality evidence for no associations was found for arm repetition, social support, decision latitude, job control and job security. Moderate evidence was found that arm-hand elevation and shoulder load double the risk of specific shoulder disorders. Low to very-low-quality evidence was found for an association between hand force exertion, hand-arm vibration, psychosocial job demands and working together with temporary workers and the incidence of specific shoulder disorders.
- shoulder
- musculoskeletal disorders
- work
- risk factors
- meta-analysis
- aetiology
Statistics from Altmetric.com
Introduction
Shoulder disorders are frequently reported in the working population, with varying prevalence rates for non-specific shoulder pain (SP) of up to 31%; for clinically assessed specific shoulder disorders such as rotator cuff syndrome (RCS) of up to 6.6% for men and 8.5% for women1; and for incidences of surgery for subacromial impingement syndrome (SIS) of 11 per 10 000 person-years.2 Moreover, in numerous countries, work-related shoulder disorders are reported as frequently occurring compensation claims or occupational diseases in various jobs and sectors of industry.3–5
Shoulder disorders represent various clinical diagnoses, varying from ICD-10 (International Classification of Diseases) codes M75.0–75.5, that is, adhesive capsulitis (M75.0), RCS—including tendinitis of the supraspinatus, infraspinatus and/or non-traumatic tears and ruptures—(M75.1), bicipital tendinitis (M75.2), calcific tendinitis (M75.3), impingement (M75.4) and bursitis (M75.5), to unspecified soft tissue disorders related to use, overuse and pressure (M70.9). Non-specific SP may be a precursor of specific shoulder disorders, but may also reflect adverse physical, psychological or psychosocial conditions.6 For work-related specific shoulder disorders, the biomechanical factors seem to be the most important; however, more recent research also stipulates that psychosocial factors may contribute to proximal factors such as biomechanical constraints.5 van Rijn et al 7 concluded in their systematic review, based on cross-sectional studies, that highly repetitive work, forceful exertion in work, awkward postures and high psychosocial job demand are associated with the occurrence of SIS.
In primary clinical practice, however, the specific disease classifications of M75.1 through 75.5 are difficult to diagnose and are often assessed with the same medical interview and the physical tests. Moreover, they often present as mixed forms, for example, impingement and bursitis. In the Netherlands, a multidisciplinary guideline of the Dutch Association of Orthopaedics (2012) was recently developed for the diagnosis and treatment of subacromial pain syndrome (SAPS), including the diagnosis of M75.1–75.5,8 9 which is used as clinical outcome in this systematic review.
Knowledge of work-related risk factors associated with SAPS is important in order to initiate primary and secondary preventive interventions at worksites. Previous systematic reviews to determine work-related risk factors for specific soft tissue shoulder disorders7 10 do not include more recent studies with longitudinal study designs (eg, ref 2) that can assess work-related risk factors for the onset of specific shoulder disorders. This systematic review aimed to examine: (i) which work-related risk factors contribute to the onset of clinically assessed SAPS and (ii) to what extent these risk factors are associated with clinically assessed SAPS.
Methods
Protocol and registration
This review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement and the study protocol was registered at PROSPERO (ID= CRD42016039059), http://www.crd.york.ac.uk/PROSPERO.
Study selection
Eligibility criteria
Primary cross-sectional, case–control and cohort studies were included when outcome data were described in terms of clinically assessed soft tissue shoulder disorder (present or not) and at least two levels of work-related exposure (exposed vs less or non-exposed) among a working population were reported in order to be able to retrieve or calculate a risk estimate.
Based on van Rijn et al,7 we defined six types of exposure: (1) force, (2) posture, (3) movement, (4) hand-arm vibration, (5) shoulder load as combined exposure measure and (6) psychosocial risk factors. Clinically assessed soft tissue shoulder disorders were grouped into SAPS, defined as all non-traumatic, usually unilateral, shoulder problems that cause pain, localised around the acromion, often worsening during or subsequent to lifting of the arm. The different clinical and/or radiological names, such as bursitis, tendinosis calcarea, supraspinatus tendinopathy, partial tear of the rotator cuff, biceps tendinitis (BT) or tendon cuff degeneration, are all part of SAPS.8 9
All types of clinical assessments were eligible for inclusion, such as work anamnesis, physical tests, questionnaires on localised pain and imaging. Studies that described work-related risk factors in terms of job or occupation, physical workload, specific occupational activities such as repetitive arm movements, or postures such as arm elevation were eligible for inclusion. The studies had to describe workers in a real workplace setting and therefore no experimental studies were included. All types of exposure assessment were eligible for inclusion: self-reports, researcher observations or direct measurements. No additional criteria were formulated regarding latency between exposure and the presence or onset of the disorder or adjustment for confounders. The exclusion criteria concerning the outcome of clinically assessed soft tissue shoulder disorders were: nerve compressions, radiating pain from cervical spine, osteoarthritis and systemic diseases.
Data sources and search terms
We searched the electronic databases of Medline and Embase for studies between 2009 and 24 March 2016 as described in online supplementary appendix 1. Our PICO can be stated as: P=working population, I/C exposed/less or none exposed to a priori defined exposure categories, O=SAPS. To construct the search strategy (JGD, HFM) a reference set of 23 potentially eligible studies was collected. Of these, 17 studies were derived from the systematic review by van Rijn et al,7 3 additional studies from a citation check of all these studies in Google Scholar and another 3 additional studies from an orienting (scoping) search. All 23 studies had to be retrieved to validate applied terms and concepts of the search strategy. Eligible studies before 2009 were retrieved from the systematic review by van Rijn et al.7
Supplementary file 1
Data collection and analyses
Study selection process
Titles and abstracts were independently screened by two review authors (HFM, CF or PPFMK) to identify potentially relevant studies. We used an online software tool to screen and assess references (https://www.covidence.org). The full texts of potentially relevant articles were assessed for eligibility against the inclusion criteria. Disagreement between review authors on the selection of studies for inclusion occurred in relation to about 5% of the references screened and was resolved by discussion.
Data extraction and management
Data were extracted by two review authors (HFM and CF) and checked by another review author (PPFMK). Data on the following were extracted from each article: author; country of study; study design (cohort, case–control or cross-sectional study); case definition of specific shoulder disorder; sources and number of participants; exposure definition; exposure assessment; exposure categories; risk estimate and adjustment for confounders.
Methodological quality assessment
Methodological quality was assessed for the studies that reported on risk factors; studies that reported on job title were analysed descriptively without quality assessment. The quality of the studies was independently assessed by two review authors (HFM, PPFMK or CF). For all study designs, the slightly adapted quality criteria (see online supplementary appendix 2) from the systematic review by van Rijn et al 7 were used. The quality criteria for exposure definition and assessment were reformulated into: (1) at least two aspects of duration, frequency and intensity of exposure; and (2) ≥3 exposure categories reported (in order to detect a dose–response).
In total, 16 items across five categories for quality assessment were assessed (see also online supplementary appendix 2): (1) study population, (2) assessment exposure,(3) assessment outcome, (4) study design and (5) data analysis. The criteria for each item were scored with ‘positive’, ‘negative’ or ‘not clear’. There was disagreement about 19 out of 240 items, all of which were resolved by discussion. High quality was defined as ≥11 items scored as ‘positive’ out of 16 quality criteria.
Association measures between work-related risk factors or job title and SAPS
Risk estimates and the corresponding 95% CIs of the association between work-related factors and SAPS were extracted or calculated and summarised. Risk estimates concerning the association between job title and shoulder disorders were described and summarised. Three review authors (HFM, CF, PFMK) discussed and decided on the risk estimates to be included in the meta-analysis.
Data synthesis
A descriptive analysis of all studies was performed, summarised, classified into categories of physical and psychosocial risk factors, and assessed for methodological quality.
Meta-analyses and quality of evidence
The selection of the work-related risk factors in the meta-analyses was based on: (1) sufficient contrast between reported exposure categories, that is, low versus high exposure; (2) clearly defined exposure criteria suitable for exposure assessment at worksites; and (3) effect estimates controlled for other non-work-related factors, as reported in the primary studies. Risk estimates for both men and women were selected when the study provided only sex-specific estimates.
The meta-analysis was performed in line with the procedure described in Watanabe et al.11: all risk estimates were transformed into a natural logarithm. The SE for a log-transformed OR was calculated based on the 95% CI for the risk estimate. A log-transformed OR and its SE were used for the meta-analysis in Review Manager (Cochrane Review Manager V.5.3). For the main analysis, the main ORs and the SEs from selected studies were subjected to a random-effects model meta-analysis to estimate a pooled OR and its 95% CI.
The quality of evidence was assessed using the GRADE (Grades of Recommendations, Assessment, Development and Evaluation) framework for prognostic studies developed by Huguet et al. 12 The starting point for the quality of the evidence was ‘high’ for longitudinal studies that sought to confirm independent associations between the prognostic factor and the outcome (‘Phase 2’ explanatory studies). The evidence could decrease on the basis of five factors: study limitations, inconsistency, indirectness, imprecision and publication bias. Moreover, two factors: (1) study findings with moderate or large effect sizes (ie, lower limit of 95% CI, OR>2.0) or (2) an exposure-response gradient, could lead to an upgrade of the quality of evidence. Four levels of quality were used: high, moderate, low and very low.
Results
Selected studies
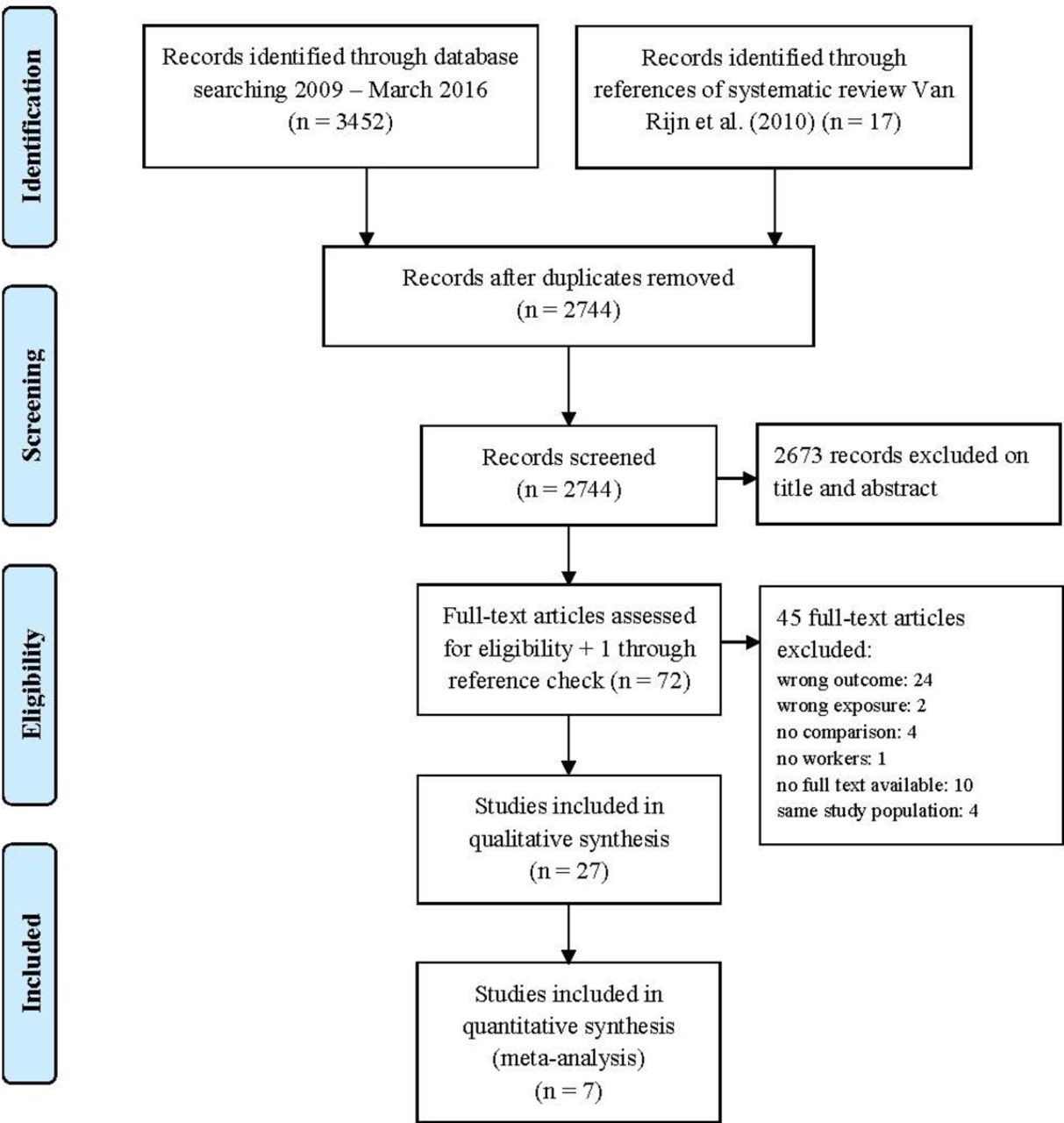
A PRISMA flow diagram of the study selection process is shown in figure 1. After excluding duplicates, 2744 references were retrieved from the databases and the systematic review by van Rijn et al,7 and assessed based on title and abstract. The full texts of 72 potentially eligible articles were then examined, of which 31 articles met the inclusion criteria, 4 of which contained the same study population and outcome of interest, resulting in 27 articles included in this review. Of the 27 articles, 12 described job title and sectors of industry, 13 described risk factors and 2 described both. Six diagnoses were studied: RCS or rotator cuff tendinitis, infraspinatus tendinitis, supraspinatus tendinitis, SIS, BT, SP with clinical test, all part of the SAPS case definition.
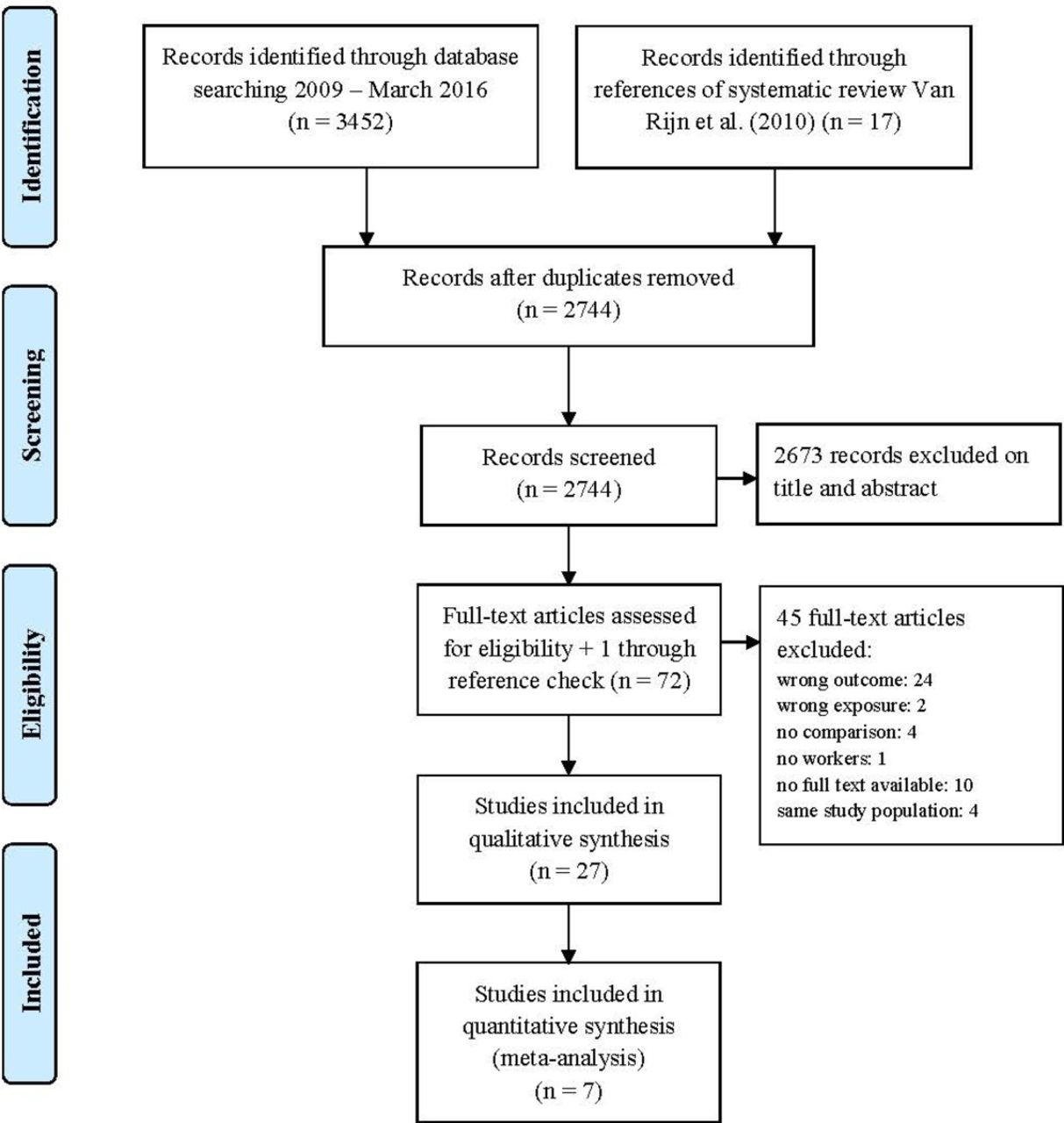
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Job title and SAPS
Fourteen studies13–26 described the association between performing a specific job or working in a sector of industry and the occurrence of clinically assessed SAPS (including the diagnoses M75.1–75.5) (see online supplementary appendix 3). The following jobs and sectors had an increased risk of SAPS: assembly workers,14 fish processing workers,15 slaughterhouse workers,16 sewing machine operators,17 manual workers,19 fishermen,20 construction and interior workers,21 metal workers,21 nurses,24 and workers in the army, air force and marines.25
Risk factors and SAPS
In total, seven longitudinal studies2 21 27–31 and eight cross-sectional studies6 22 32–37 described the association between exposure to physical and psychosocial risk factors and the occurrence of clinically assessed SAPS (see online supplementary appendix 4). The characteristics of the outcome definition (SAPS) and exposure definition (in intensity, frequency and duration) are presented in table 1.
Definition and assessment of exposure and outcomes for studies included concerning risk factors (n=15)
Methodological quality
The methodological quality of the studies of risk factors varied from scoring 7 out of 16 items to 16 out of 16 items (see table 2). The most frequently missing quality items were the lack of blinding for outcome status (ie, specific shoulder disorder) and the reverse, the lack of blinding for exposure status, as well as a lack of information about completers versus withdrawals from the study. All six cohort and one case–control studies met the quality level of ≥11 out of 16 quality criteria; among the eight cross-sectional studies five met ≥11 quality criteria.
Methodological quality scores of 16 items for studies regarding risk factors*
Meta-analyses and assessment of evidence
In total, 16 300 patients with specific shoulder disorders from a population of 2 413 722 workers from Denmark, Finland, France, Germany and Poland were used in the meta-analysis. Two study populations were overlapping to some extent,2 31 therefore the risk estimates in the cohort study of Svendsen et al 31 were censored by the original authors for the period from 1996 through 2002. Figure 2 and additional figures in online supplementary material summarise the results of the meta-analyses, while table 3 summarises the assessment of evidence concerning risk factors for specific shoulder disorders.

{kind=link}
{kind=link}
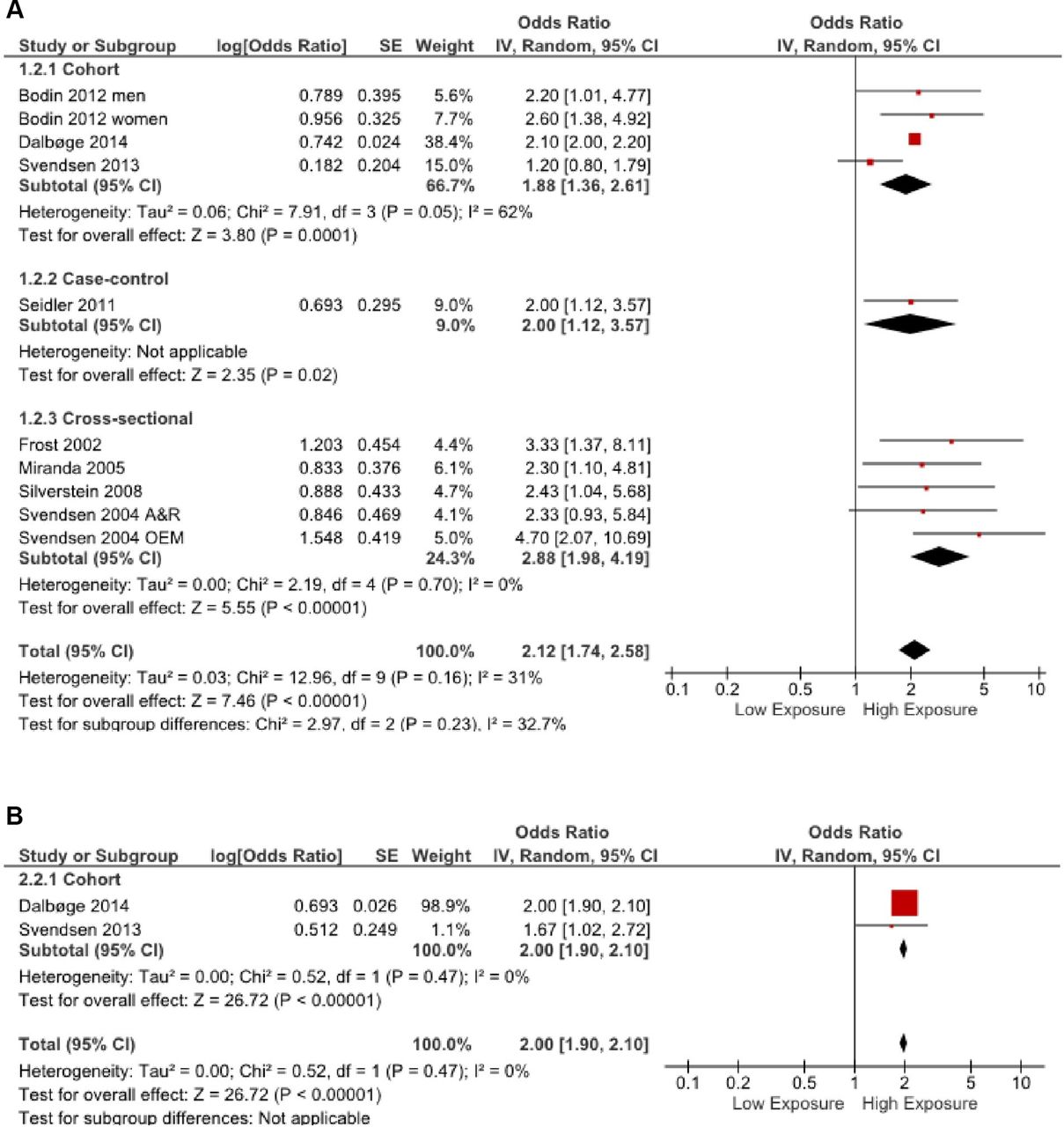
Forest plots. (A) Forest plot of studies regarding arm elevation and SAPS. (B) Forest plot of studies regarding shoulder load and SAPS. df, degrees of freedom; SAPS, subacromial pain syndrome.
Quality of the evidence for the relationship between risk factors and specific soft tissue shoulder disorders according to the GRADE framework
Arm elevation
Three cohort studies2 28 31 and one case–control study21 demonstrate that there is moderate quality evidence that arm elevation increases the incidence of SAPS, with a pooled OR of 1.91 (95% CI 1.47 to 2.47) (table 3), comparable to the pooled OR of 2.12 (95% CI 1.74 to 2.58) (figure 2A) when also including the cross-sectional studies (n=5) of sufficient quality.
Shoulder load
Two cohort studies2 31 demonstrate that there is moderate quality evidence that shoulder load increases the incidence of SAPS, with a pooled OR of 2.00 (95% CI 1.90 to 2.10) (table 3 and figure 2B).
Hand-arm force exertion
Four cohort studies2 28 29 31 and one case–control study21 demonstrate that there is low-quality evidence that hand-arm force exertion increases the incidence of SAPS, with a pooled OR of 1.53 (95% CI 1.25 to 1.87) (table 3), comparable to the pooled OR of 1.56 (95% CI 1.26 to 1.93) (online supplementary figure 2.3) when also including the cross-sectional studies (n=3) of sufficient quality.
Supplementary file 2
Arm-hand repetition
Three cohort studies2 29 31 demonstrate that there is low-quality evidence for no increased incidence of SAPS due to arm-hand repetition with a pooled OR of 1.42 (95% CI 0.91 to 2.22) (table 3), which is significantly lower compared with the pooled OR of 1.70 (95% CI 1.18 to 2.46) (online supplementary figure 2.4) when also including the cross-sectional studies (n=2) of sufficient quality.
Hand-arm vibration
Three cohort studies2 27 29 and one case–control study21 demonstrate that there is low-quality evidence that hand-arm vibration increases the incidence of SAPS, with a pooled OR of 1.34 (95% CI 1.01 to 1.77) (table 3), comparable to the pooled OR of 1.34 (95% CI 1.02 to 1.76) (online supplementary figure 2.5) when also including the cross-sectional study (n=1) of sufficient quality.
Psychosocial demands
Three cohort studies29–31 demonstrate that there is low-quality evidence that psychosocial demands increase the incidence of SAPS, with a pooled OR of 1.12 (95% CI 1.01 to 1.25) (table 3), comparable to the pooled OR of 1.14 (95% CI 1.04 to 1.24) (online supplementary figure 2.6) when also including the cross-sectional studies (n=3) of sufficient quality.
Social support
Three cohort studies28 30 31 demonstrate that there is low-quality evidence for no increased incidence of SAPS due to low social support from colleagues and/or manager, with a pooled OR of 1.05 (95% CI 0.83 to 1.33) (table 3), comparable to the pooled OR of 1.02 (95% CI 0.84 to 1.24) (online supplementary figure 2.7) when also including the cross-sectional study (n=1) of sufficient quality.
Decision latitude
Two cohort studies29 30 demonstrate that there is low-quality evidence for no increased incidence of SAPS due to low decision latitude, with a pooled OR of 1.08 (95% CI 0.89 to 1.31) (table 3), which is comparable to the pooled OR of 1.01 (95% CI 0.81 to 1.25) (online supplementary figure 2.8) when also including the cross-sectional study (n=1) of sufficient quality.
Job control, job security and working with temporary workers
One cohort study31 demonstrates that there is low-quality evidence for no increased incidence of SAPS due to low job control, with an OR of 1.22 (95% CI 1.00 to 1.50). One cohort study30 demonstrated that there is low-quality evidence for no increased incidence of SAPS due to low job security, with an OR of 1.12 (95% CI 0.93 to 1.36). One cohort study28 demonstrated very-low-quality evidence that for female workers there is an increased incidence of SAPS when working together with temporary workers, with an OR of 2.2 (95% CI 1.2 to 4.2) (table 3).
Discussion
Main findings
This systematic review, including a meta-analysis, revealed moderate evidence that arm elevation and shoulder load increase the incidence of specific shoulder disorders, with estimated pooled ORs around 2.0. Low to very-low-quality evidence was found for an association between hand force exertion, hand-arm vibration, psychosocial job demands and working together with temporary workers and the incidence of specific shoulder disorders. Low-quality evidence suggesting no associations was found for repetitive arm movements, social support, decision latitude, job control and job security.
Most longitudinal studies were controlled for the personal factors of age and sex, for non-work-related factors such as specific leisure time or sport activities, and for other work-related factors. This could be a reason why the psychosocial factors were found to contribute little to the incidence of these specific shoulder disorders. The biological pathway for specific shoulder disorders seems to be biomechanical in nature (eg, ref 38), while psychosocial factors might act as more intermediating factors5 influencing these biomechanical factors.
This review confirmed and strengthened the evidence on risk factors as reported in the systematic review by van Rijn et al.7 Based on the more recent published prospective cohort and case–control studies used in our review, the most important risk factors for clinically assessed soft tissue-specific shoulder disorders defined as SAPS are arm elevation and shoulder load in terms of combined physical exposures. Psychosocial factors seem to contribute to a much lesser extent in the onset of specific shoulder disorders.
Risk factors and SAPS
The exposure categories for the risk factors and the case definitions of the specific shoulder disorders varied in the included studies. Therefore, we have explicitly described all definitions and assessments (see table 1) and reported outcomes (see online supplementary appendix 4). The variability in exposure categories of the retrieved risk factors, however, did not allow to combine comparable exposure levels across studies into more detail.
The variability in case definitions of specific shoulder disorders was partly due to the different clinical settings, which varied from a primary care setting to a clinical specialist. Although case definitions for the specific shoulder disorders varied, all studies in the formal and secondary meta-analyses clinically assessed these disorders using a combination of symptoms and signs in terms of diagnostic physical testing and/or imaging as recommended in the multidisciplinary guideline for diagnosis of SAPS.8 9 This guideline also proposes using a combination of clinical tests to increase post-test probability of a diagnosis of SAPS. Consequently, further research in the area of clinical assessment of specific shoulder disorders (eg,39 40combined with more detailed exposure assessment in using intensity, duration and frequency of risk factors (eg, ref 2) will contribute to a better insight into the pathogenic pathways and attributional fractions of worksite exposure.
Methodological considerations
Meta-analyses were performed to estimate pooled associations, although there was heterogeneity in the clinically assessed shoulder disorders and the assessment of exposure to risk factors in the longitudinal studies included in this review. For each risk factor we have chosen to contrast between the lowest and highest exposure category for answering our research questions whether or not an increased risk is present and to what extent. To prevent data-driven approaches, we did not select other exposures between low and high. Furthermore, a reported dose–response relation in the original studies was used in the GRADE assessment. For specific shoulder disorders we used the case definition of SAPS, although in two studies2 31 it was not possible to differentiate the results between SAPS diagnoses and a supposed small proportion of osteoarthritis cases.
Heterogeneity, however, was explicitly addressed through the grading of the quality of evidence. Publication bias was difficult to assess because of the small number of studies included in each risk factor. Taking cross-sectional studies into account—also including smaller study groups with and without statistically significant associations—made little difference to the estimates of the pooled ORs, with exception of repetitive arm movements. However, we treated the assessment of publication bias conservatively by downgrading the evidence in the case of lack of clarity.
In this systematic review based on a validated search in two databases, all three criteria for the establishment of work-related disorders41 were encountered, namely clinical diagnosis, exposure and evidence for causal relationships. Evidence for causal relationships was based on the meta-analyses and grading of the evidence. The choice of risk factors for the meta-analyses was transparent, and based on maximal contrast between exposure categories and feasibility of assessment for diagnosis and exposure assessment in general practice. Exploration of the formal meta-analyses (prospective cohort and case–control studies) by including cross-sectional studies yielded associations in the same direction.
Prevention
Knowledge of evidence-based work-related risk factors can stimulate primary and secondary prevention. Preventive actions to reduce arm elevation and shoulder load as combined physical exposures, for example, hand force exertion and arm elevation, are recommended to prevent specific work-related shoulder disorders. Psychosocial demands and working together with colleagues in temporary employment were the only psychosocial factors that revealed significant associations with specific shoulder disorders in this review. It is possible that psychosocial factors play an intermediate role,5 38 and therefore should also be targeted in occupational preventive actions. In addition, as psychosocial factors play a more prominent role in the onset and prevalence of non-specific SP—through other biological pathways such as muscle strain from the neck and shoulder muscles—targeted interventions counteracting these factors might also be considered. There are indications that specific strength training42–44 or just general exercise training,45 adjustment to furniture and equipment46 and improving work techniques like taking more breaks and reducing work demands can reduce specific and non-specific shoulder disorders.47
Conclusions
Arm-hand elevation and shoulder load double the risk of specific soft tissue shoulder disorders. Low to very-low-quality evidence was found for an association between hand force exertion, hand-arm vibration, psychosocial job demands and working together with temporary workers and the incidence of specific shoulder disorders.
Acknowledgments
We are very grateful to the authors of the paper by Svendsen et al 31 for the reanalyses of their data so we could incorporate their outcomes in our meta-analyses.
References
Footnotes
Contributors HFM initiated the study, performed the statistical analyses and drafted the manuscript. JGD contributed to the literature search. HFM, CF and PFMK performed the study selection, data extraction and interpretation of the data. MHWFD was the principle investigator in this study. All authors made substantial contributions to the conception of the study and manuscript.
Funding The work was sponsored by the Ministry of Social Affairs and Employment, the Netherlands (Grant No. 5100-22709).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.