Article Text

Abstract
Evidence increasingly confirms that synthetic chemicals disrupt the endocrine system and contribute to disease and disability across the lifespan. Despite a United Nations Environment Programme/WHO report affirmed by over 100 countries at the Fourth International Conference on Chemicals Management, ‘manufactured doubt’ continues to be cast as a cloud over rigorous, peer-reviewed and independently funded scientific data. This study describes the sources of doubt and their social costs, and suggested courses of action by policymakers to prevent disease and disability. The problem is largely based on the available data, which are all too limited. Rigorous testing programmes should not simply focus on oestrogen, androgen and thyroid. Tests should have proper statistical power. ‘Good laboratory practice’ (GLP) hardly represents a proper or even gold standard for laboratory studies of endocrine disruption. Studies should be evaluated with regard to the contamination of negative controls, responsiveness to positive controls and dissection techniques. Flaws in many GLP studies have been identified, yet regulatory agencies rely on these flawed studies. Peer-reviewed and unbiased research, rather than ‘sound science’, should be used to evaluate endocrine-disrupting chemicals.
- ENDOCRINOLOGY
- Environmental epidemiology
- ENVIRONMENTAL HEALTH
- TOXICOLOGY
Statistics from Altmetric.com
The state of the science on endocrine-disrupting chemicals
Endocrine-disrupting chemicals (EDCs) are compounds or mixtures of compounds that interfere with hormone action and thereby contribute to disease and disability.1 In 1996, when the studies of EDCs were in their infancy, the US EPA defined endocrine disruptors as ‘exogenous agent[s] that interfere with the synthesis, secretion, transport, binding, action, or elimination of natural hormones in the body which are responsible for the maintenance of homeostasis, reproduction, development and/or behavior’.2
The chemicals’ landscape has changed drastically in the past decades, with >85 000 chemicals on the market and thousands more that have been produced (figure 1). Simple compiling of programmes like those used in the US EPA's Endocrine Disruptor Knowledge Base3 and evaluations of the published, peer-reviewed scientific literature by the international non-profit organisation, the Endocrine Disruptor Exchange4 have identified >1000 chemicals with potential endocrine-disrupting properties. The US Environmental Protection Agency's (EPA) Endocrine Disruptor Knowledge Base identifies only those chemicals that bind to three hormone receptors: oestrogen, androgen and thyroid (n>1800).5 A more comprehensive examination of all hormones relevant to human physiology is likely to yield a much larger number than this limited EPA screening effort. In addition, EDCs can display actions beyond simple receptor binding, and so even a broad examination of hormone receptor binding would yield a vast underestimate of the total number of EDCs.
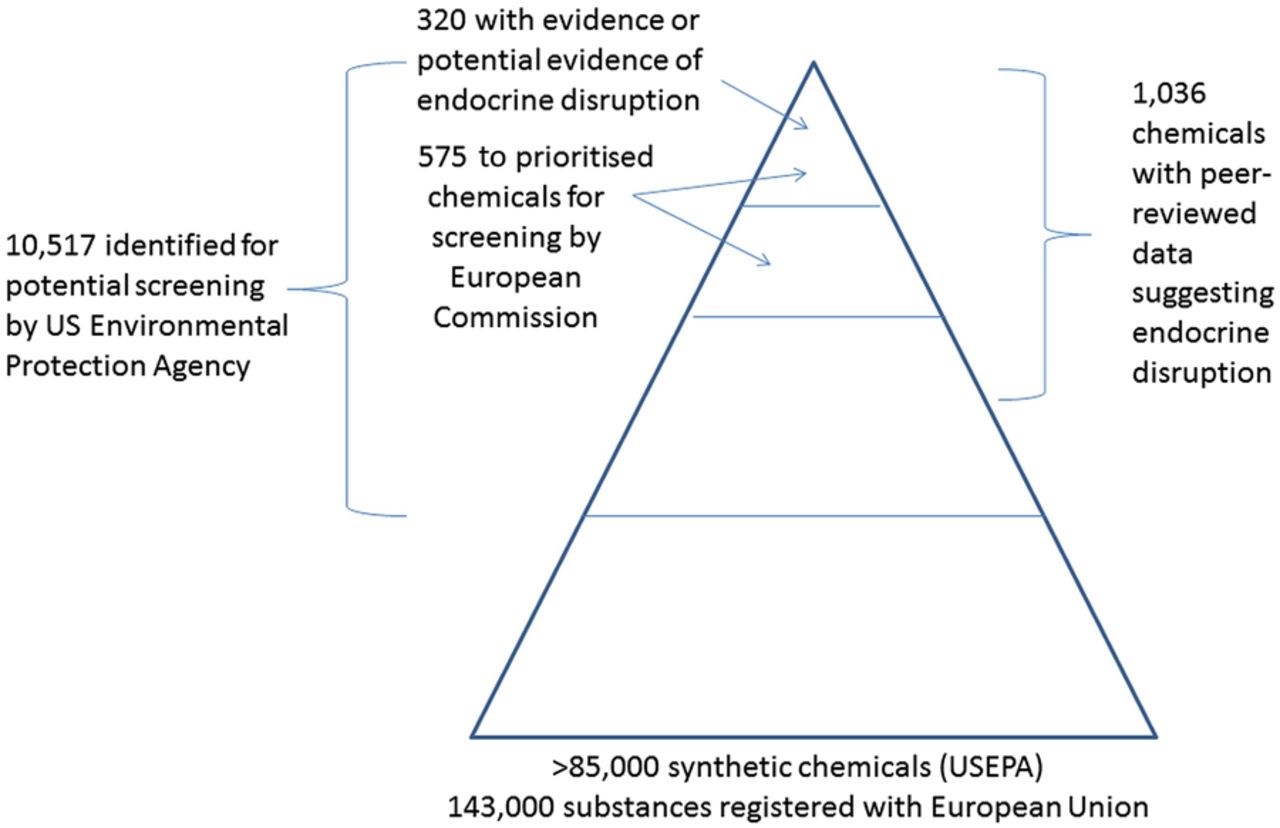
Identifying endocrine disruptor in the universe of synthetic chemicals.
In 2002, one of the first international reports on EDCs was written by experts and assembled by the International Programme on Chemical Safety and WHO.6 More recent reports and scientific statements from the Endocrine Society7 ,8 and the WHO and United Nations Environment Programme (UNEP) have reviewed studies demonstrating the relationship between EDC exposures and endocrine diseases in controlled animal studies and human populations.9 Other scientific organisations have followed these scientific statements with additional expressions of concern including the International Federation of Gynecologists and Obstetricians, which called for the reduction of prenatal EDC exposures to prevent a broad array of female reproductive and other problems across the life course.10
Evidence reviewed in these scientific statements increasingly confirms that synthetic chemicals disrupt the endocrine system and contribute to disease and disability across the lifespan. Sufficient evidence demonstrates that EDCs can induce diseases and dysfunctions including neurodevelopmental and cognitive deficits, infertility and other reproductive disorders, obesity and diabetes, immune dysfunction, asthma and cancers.8 Epidemiological studies similarly suggest associations between EDC exposures and these conditions in environmentally exposed populations. For some compounds, the coherence between epidemiological studies at the doses encountered in current populations and in vivo experiments (and also sometimes in vitro studies) adds to the strength of arguments for causality. Examples include phthalates and their disruption of metabolic processes, as well as organophosphates and brominated flame retardants and disruption of prenatal thyroid with neurocognitive consequences.11 ,12
EDCs: how controversial are they?
After the publication of the 2012 UNEP/WHO report on EDCs, a number of critical statements were published in the scientific literature.13 ,14 These rebuttals of the UNEP/WHO report raised a number of issues including concerns that the report did not use systematic review criteria in the evaluation of evidence.15 Yet, these rebuttals included many scientifically inaccurate comments, specifically misrepresenting criteria for interpreting causation as originally elaborated by Sir Austin Bradford Hill some 50 years ago,16 incorrectly suggesting that standardised ‘weight of evidence’ approaches can be readily applied to evaluate endocrine disruption, and dismissing low-dose effects as well as non-linear and non-monotonic exposure–response relationships that are extremely well documented. Concerns raised about the UNEP/WHO report were rebutted in a number of recent articles by the UNEP/WHO authors and others.17–19 A recent manuscript noted parallels between the rebuttals of the UNEP/WHO report and tactics once used by the tobacco industry to prevent public health actions and scientific progress.17 These approaches also include the failure of many authors to report conflicts of interest including paid consultancies for industries that manufacture EDCs.20
The UNEP/WHO report was welcomed at the Fourth International Conference on Chemicals Management (ICCM4). More than 100 countries present at this conference agreed by consensus on four key points:21 (1) EDC exposures can result in adverse effects in humans and wildlife; (2) the most vulnerable period for EDC exposure is during embryogenesis, fetal development and perinatal life, when organ systems are developing; (3) EDC exposures during development can result in adult-onset diseases and (4) focus should be on reducing EDC exposures. Interestingly, there was one major exception to the acceptance of the UNEP/WHO report by the participants at ICCM4: industry associations representing global chemicals and pesticide producers and a US business association registered their disagreement with the state of science. A footnote in the ICCM4 report thus identifies the limited stakeholders who dispute the UNEP/WHO report, stating ‘The International Council of Chemical Associations, CropLife International and the United States Council for International Business wish to note that the methodology and conclusions of the report remain contentious amongst certain scientific groups’.
Additional meetings and reports22–24 have demonstrated that much of the debate on the concerns over EDC exposures represents ‘manufactured doubt’.25 What does this mean about the controversial nature of EDCs? Clearly, there are still many aspects of endocrine disruptor science that are unsettled, but these are generally related to the mechanisms responsible for the action of EDCs, rather than the principal induction of health outcomes themselves. Further research is needed to understand the extent of adverse effects that can be induced by each possible EDC, the precise shapes of dose–response functions for all exposure–disease pairs and the exact public health impact.
Similar ‘manufactured doubt’ existed about lead and its effects on the developing brain, despite substantial and accelerating evidence documenting adverse effects on young children that were permanent and lifelong. Policy action to remove lead from gasoline occurred even with incomplete information available. Scientific experts, then as now, provided data that policymakers interpreted and decided how to protect society while balancing other interests. While scientists are humans and are also affected by personal values, we aim for objectivity, recognising a responsibility to communicate real and serious threats when they are present. The current scientific evidence for endocrine disruption parallels that which existed for climate change just a few years ago. As citizens, our responsibility is to communicate the reality that the scientific case for policy action is now strong, and the health of future generations is clearly at stake.
Sound science: who could be against it?
Recent calls for ‘sound science’ in the evaluation of EDC data have been made by groups like the American Chemistry Council.26 In Doubt is their Product, David Michaels notes that the origin of the term ‘sound science’ can be traced back to the tobacco industry. Michaels wrote,27 ‘The vilification of any research that might threaten corporate interests as “junk science” and the sanctification of its own bought-and-paid-for research as “sound science” is indeed Orwellian—and nothing less than standard operating procedure today. But to give credit where credit is due, the sound science/junk science dichotomy has worked wonders as a public relations gimmick and has gained widespread acceptance in the current debate over the use of scientific evidence as policy’.
‘Sound science’ seems like something that all scientists should support. Who could be against good, transparent science? In the case of EDCs, the chemicals industry has suggested that ‘sound science’ requires the use of good laboratory practices (GLPs), a series of record-keeping procedures and data-reporting protocols. GLP was actually instituted in response to serious cases of fraud after industry and contract laboratories were found to have falsified chemical toxicity data.28 Because of the regulatory and financial burden associated with GLP, studies that comply with these regulations are typically conducted by the industry or contract laboratories hired by the industry; academic laboratories are rarely equipped, staffed or funded at the levels needed to conduct studies according to GLP and instead rely on independent replication to assess reliability and validity, which are not guaranteed using GLP. Regulatory agencies like the US EPA are bound by requirements that studies used in chemical risk assessments must be performed according to the GLP. This guidance was written to prevent the use of fraudulent studies conducted by contract laboratories and is now being used to exclude peer-reviewed, often government-funded studies conducted in academic laboratories from being used in risk assessment decision-making. This is especially concerning given the influence that funding source has been shown to have on study outcomes.17 ,29–31
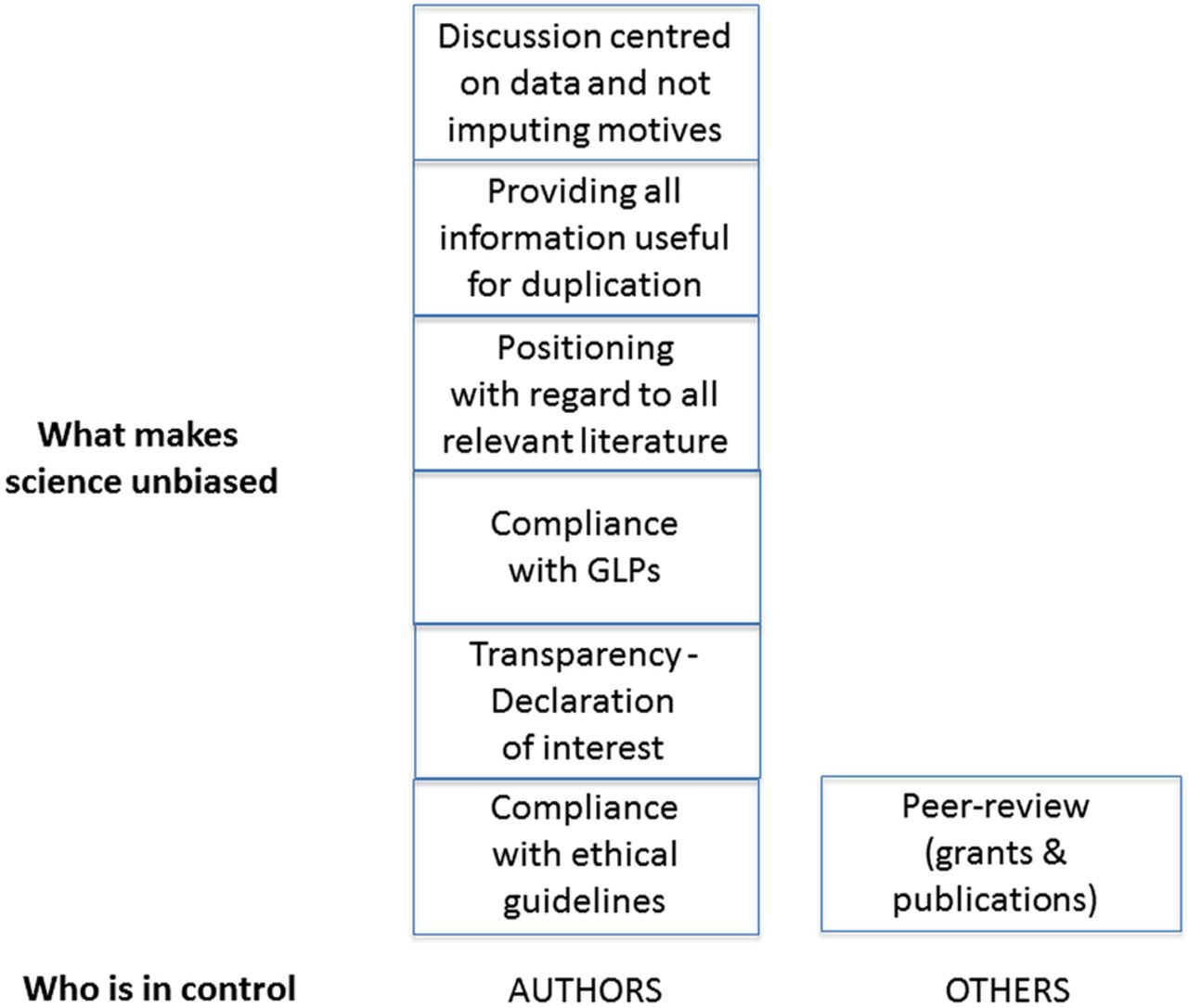
Further concerns are raised by the evaluations that have shown serious flaws in GLP-compliant studies including contamination of negative controls, lack of responsiveness to positive controls and technical problems including inadequate dissection techniques.31–33 Last, the rigorous reviews that are involved in obtaining grants from National Institutes of Health and other funding institutions before conducting research and the peer-review process that precedes publication of results are far more effective in identifying qualified, accurate science than is adhering to GLP.27 As illustrated in figure 2, all components of what would make science ‘sound’ but one is under the author's control. Credit to and credibility of science rest on a single and crucial component: peer review.

{kind=link}
{kind=link}
Components of peer-reviewed and unbiased science and stakeholders.
A focus on scientific principles
Scientific experts have argued that specific principles should be used in the evaluation of environmental chemicals with endocrine-disrupting properties.34 In particular, endocrinologists have noted that scientists studying EDCs must understand five principles of endocrinology: (1) the endocrine system coordinates the functions of the body from conception until death; (2) the effects of hormones are mediated via specific interactions with receptors; (3) hormones have different effects depending on life stage, with developmental exposures typically associated with permanent ‘organisational’ responses; (4) hormones act at low doses and (5) hormones can induce non-linear and non-monotonic dose responses.
Considering these basic principles of hormones, a number of issues have been raised with the types of end points that are favoured in the evaluation of potential EDCs. The test guidelines developed in the 1930s are still in use (eg, OECD Test Guideline 440, the uterotrophic assay) for the evaluation of EDCs. The end points included in test guidelines use insensitive toxicity outcomes such as organ weight that do not reflect human disease processes.35 ,36 They also use a limited range of doses17 and rely on extrapolations to lower doses that are rarely tested for adverse effects. Furthermore, test guidelines assume the antiquated Paracelsian notion that the ‘dose makes the poison’, rejecting or ignoring examples of non-monotonicity, even when they are present.37 Typical regulatory toxicology studies rarely justify the number of animals by power calculations, nor do they follow the rule to increase the number of animals as the tested dose decreases, as would be required to maintain power constant when the difference between exposed animals and controls is expected to decrease. The statistical tests used to identify ‘thresholds’ are often rudimentary, if not statistically wrong. Finally, many test guidelines ignore critical periods in development, allowing some effects to be missed, producing misleading results and contributing to incorrect policy decisions. For example, an OECD guideline study suggests testing the effects of chemicals on female rodents at 22–42 days of life to evaluate the effects on puberty.38 Yet, it is well known that earlier periods including fetal and perinatal development are critical for maturing the signalling pathways that regulate the secretion of hormones at puberty as well as pubertal development of hormone-sensitive organs, as evidenced by the tragic history of the pharmaceutical diethylstilbestrol (DES). Young girls exposed to DES in utero developed cancers of the reproductive tract, and to date effects in so-called DES sons and daughters are being elaborated, including obesity and additional cancers.39–44
A number of additional issues have been debated in the context of regulatory decision-making for EDCs. One debate surrounds the use of potency for the prioritisation, evaluation or even the identification of EDCs. Some arguments suggest that binding affinity can be used as a surrogate or predictor of the potency of a compound,45 ,46 so that chemicals with a low-binding affinity for a hormone receptor relative to the native hormone can be dismissed or ignored as ‘weak’ agonists (or antagonists).47 This notion is easily dismissed considering significant evidence that potency is end point-specific and, thus, cannot be predicted by the knowledge of binding affinity alone. For example, bisphenol A has been shown to be 10 000 or 100 000 times weaker than 17β-oestradiol when considering its effects on uterine weight, but equipotent when considering its effects on insulin release from pancreatic islets, and doses that have no effect on organ weight can alter the development of oestrogen-sensitive organs such as the brain.48–51
Other issues related to the discussion of potency suggest that there are ‘adaptive’ responses after exposures to synthetic chemicals with low potency, and that these ‘weak’ EDCs do not cause obvious harm because the body is able to compensate for their effects.52 Yet evidence from pregnancy cohorts in humans demonstrates that so-called compensated or subclinical hypothyroidism contributes to adverse neurodevelopmental outcomes in children.53–55 Those groups that support the use of potency in the prioritisation of EDCs suggest that only those chemicals that cause overt and measurable toxic effects in animals such as tumour incidence should be restricted.46 This is an unscientific and dangerous distinction, analogous to the argument that has been made with regard to low-level lead exposures; industry consultants have repeatedly argued that effects on outcomes like IQ are not adverse.56 ,57 The social costs of IQ include lost lifetime economic productivity, intellectual disability and increased risk of criminality. Improved cognition and health from the phase-out of lead from gasoline, dismissed by some as irrelevant, produce $2.4 trillion in economic benefits globally each year, representing 4% of global gross domestic product.58
Similar to the arguments about potency, debate has surrounded issues related to ‘low-dose effects’ and the presence of thresholds (eg, doses below which no effects can be seen) for EDCs.15 ,59 ,60 Again, conversations regarding these issues often address whether effects seen at low doses are representative of ‘adverse’ outcomes, and this discussion is further complicated by the inability or unwillingness of many regulatory agencies to describe which end points are adverse.19 ,34 ,61 ,62
The cost of inaction
Decisions about whether actions should be taken to protect public health often consider the financial implications of such actions, even when economic costs are not supposed to be considered in such evaluations. This has recently been raised in the European Union, where the European Commission was found to have broken the law in their delay to propose scientific criteria for the evaluation and identification of EDCs.24 Although draft criteria were proposed in 2013, the European Commission has instead conducted an economic assessment of the various proposed draft criteria rather than use scientific principles, judgement and justification for the selection of final criteria. Economic assessments are also widely used in other countries (eg, by the Office of Information and Regulatory Affairs in the Office of Management and Budget in the USA).
The problem with using economic assessments in environmental health decision-making is that typically only one side of the economic equation (eg, the cost to industry) is evaluated, leaving the costs of inaction (eg, environmental and health costs as well as reduced quality of life) unexamined. A historical example of this phenomenon comes from studies examining the association between air particulate and disease outcomes;63 estimates of the economic burden on industries including the fossil fuel industry suggested that the cost of reducing particulate matter would cripple the economy. Yet, additional evaluations showing the benefits to public health of reducing particulate matter led to different conclusions: the economic benefits of improved health would outweigh the costs to industry.64 Recently, similar analyses were conducted which evaluated a limited number of EDC exposures for which there was the greatest evidence linking exposures to diseases and dysfunction. Six peer-reviewed articles were published in the Journal of Clinical Endocrinology and Metabolism attributing EDC exposures in Europe to healthcare costs of over €160 billion annually.11 ,12 ,65–68 These evaluations represent conservative estimates because they examined only 15 exposure–outcome relationships for which there is substantial probability for causation. In addition, because they did not include many indirect costs of chronic diseases due to EDCs and evaluated fewer than 5% of all EDCs, the cost estimates are likely to represent only a small subset of the true costs of EDCs in Europe. On the basis of the data from the US Centers for Disease Control and Prevention, a similarly large burden of disease may be attributable to EDCs in the USA; exposures to EDCs in the USA are in many cases equal to if not higher than those in the European Union. These findings speak to the substantial health and economic benefits that can be obtained by applying the best science, and not simply ‘sound science’, to inform regulatory policymaking. An additional issue is that the economic costs of regulation are often carried out in a simplistic way, assuming that the cost to the industry of banning a compound would correspond to the current market share of the compound. This amounts to assuming that if, for example, a pesticide is banned, the money formerly used to buy this pesticide will not be used to buy any other pesticide, nor anything else, and stored in a safe.
Conclusions
In the USA, the original 1976 Toxic Substances Control Act did not require that chemicals are tested prior to their use in many consumer products and industrial applications.69 Although the REACH (Registration, Evaluation, Authorization and Restriction of Chemicals) legislation and other regulations on pesticides and biocides in the European Union give the EU the authority to regulate these chemicals, additional debates about how EDCs should be defined and identified have prevented many anticipated chemical regulations and restrictions.70
To date, the US Environmental Protection Agency has identified 10 517 chemicals for potential endocrine disruptor screening and testing, yet has only screened 52 chemicals with the tests in the Endocrine Disruptor Screening Programme (figure 1).71 ,72 In testing completed at the behest of the European Commission, 320 of 575 chemicals prioritised for screening showed evidence or potential evidence for endocrine disruption.73 These numbers illustrate the size of the problem, and the need for regulatory action. Moving forward, evaluations of EDCs should rely on scientific principles, well-designed and transparently reported studies and consideration of the economic costs of inaction.
What is already known on this subject
Despite agreement by scientists and governments that chemicals contribute to disease by disrupting endocrine systems, ‘manufactured doubt’ continues to be cast as a cloud over rigorous, peer-reviewed and independently funded scientific data.
What this study adds
Moving forward, evaluations of endocrine disrupting chemicals should rely on scientific principles, well-designed and transparently reported studies and consideration of the economic costs of inaction.
References
Footnotes
Twitter Follow Leonardo Trasande at @leotrasande
Contributors LT wrote the first draft with LNV. All other authors provided thoughtful insights and revisions, and contributed to final review.
Funding LNV was supported by Award Number K22ES025811, and LT was supported by R01ES022972 and R01DK100307 from the National Institute of Environmental Health Sciences (NIEHS) of the National Institutes of Health. J-PM was supported by the Broad Reach Fund, the Fund for the Carolinas, the Marisla Foundation and the Wallace Genetic Foundation for work on endocrine-disrupting chemicals. FvS was supported by NIEHS grants (ES020952 and ES021394).
Disclaimer The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests LNV has been received travel reimbursement from Universities, Governments, NGOs and Industry, to speak about endocrine-disrupting chemicals. J-PB, RS, LT and RTZ acknowledge the support of the Endocrine Society for travel and participation in meetings about incorporation of endocrine science data in regulatory management of EDCs. FvS received an honorarium from Nipro Medical Corporation to present a lecture.
Provenance and peer review Commissioned; externally peer reviewed.