Article Text

Abstract
Objective This study aims to systematically review all published quantitative studies examining the direct association between social capital and common mental disorders (CMD). Social capital has potential value for the promotion and prevention of CMD. The association between different types of social capital (individual cognitive and structural, and ecological cognitive and structural) and CMD must be explored to obtain conclusive evidence regarding the association, and to ascertain a direction of causality.
Design 10 electronic databases were searched to find studies examining the association between social capital and CMD published before July 2014. The effect estimates and sample sizes for each type of social capital were separately analysed for cross-sectional and cohort studies. From 1857 studies retrieved, 39 were selected for inclusion: 31 cross-sectional and 8 cohort studies. 39 effect estimates were found for individual level cognitive, 31 for individual level structural, 9 for ecological level cognitive and 11 for ecological level structural social capital.
Main results This review provides evidence that individual cognitive social capital is protective against developing CMD. Ecological cognitive social capital is also associated with reduced risk of CMD, though the included studies were cross-sectional. For structural social capital there was overall no association at either the individual or ecological levels. Two cross-sectional studies found that in low-income settings, a mother's participation in civic activities is associated with an increased risk of CMD.
Conclusions There is now sufficient evidence to design and evaluate individual and ecological cognitive social capital interventions to promote mental well-being and prevent CMD.
- MENTAL HEALTH
- SOCIAL CAPITAL
- SYSTEMATIC REVIEWS
- PSYCHIATRY
Statistics from Altmetric.com
Background
Common mental disorders (CMDs) comprising depressive and anxiety disorders cause significant disability globally and can be extremely costly to the individual, their families and the countries in which they live.1 Poor mental health is associated with poverty,2 and can lead to a loss of productivity and decreased human capital, impeding sustainable development.3–5 Social capital, which measures the quality and quantity of social relationships in a community, may be a protective factor6 which could both prevent CMD developing and promote wider economic development.
Definition of social capital
The nature of social environments has been hypothesised to explain why some populations have worse mental health outcomes than others.7 Social capital is a way of conceptualising and measuring the social environment. The definition of social capital is controversial,8 but the sixth edition of the Dictionary of Epidemiology describes social capital as: “The resources—for example, trust, norms, and the exercise of sanctions—available to members of social groups…social capital is conceptualized as a group attribute” and (2) “The resources—for example, social support, information channels, social credentials—that are embedded within an individuals’ social networks…social capital is conceptualized as an individual attribute as well as a property of the collective.”8
The features of social capital can be grouped into the quantity of social interactions, termed as structural social capital, and the quality of social interactions, termed cognitive social capital.9 Structural (participatory) social capital refers to relationships, networks, membership, organisations, associations and institutions that may link groups or individuals together. Cognitive (perceived) social capital refers to values, norms, attitudes, beliefs, civic responsibility, altruism and reciprocity within a community.9 ,10 These concepts are distinct from social networks and networking, social hierarchies, relationships between family and friends, and other social determinants such as neighbourhood deprivation, which fall outside the definition of social capital and are, therefore, not included in this review.
Social capital states that individuals and groups may benefit from participation and mutual cooperation within an array of social networks at both the individual and ecological level.9 ,11 ,12 Individual social capital (ISC) is measured by asking an individual series of questions about their participation in community groups and activities, and their perception of the quality of these relationships, such as whether they are reciprocal or based on trust. Ecological social capital (ESC) is most commonly measured by asking a representative sample of the community the ISC questions and then aggregating these to the community level to produce, for example, average levels of civic engagement or trust in a community.9 ESC can also be measured contextually, such as by voting rates. Table 1 outlines the different ways in which social capital is measured.
Measures of social capital
Causal pathway between social capital and CMD
The aetiology of mental illness is important to consider when looking at how social capital may affect CMD. The association between social determinants, such as low socioeconomic status, lack of education, unemployment and exposure to negative life events is well established.13 The concept of social capital extends these social determinants to also include the quantity and quality of social relationships.
Social capital can affect CMD on the individual and ecological level. For individuals, living in a trusting neighbourhood that alleviates daily stressors and promotes good health behaviours can be protective against CMD.14 ,15Those with high social capital have more opportunity for social support, influence, engagement and access to resources that impact health.16 Low social capital in the individual as well as the community could cause hostile environments and reduce buffers against CMD.15 ,17
ESC affects community productivity,15 social efficacy, political marginalisation and government performance.9 These factors influence social services, infrastructure and investment in human capital, which in turn influence the social environment, resources available to individuals and community buffers. These factors can contribute to the incidence and prevalence of CMD.9 ,15 Communities with low tolerance of mental illness may also exclude affected members, leading to worse health outcomes.9
The association between social capital and CMD
A recent systematic review of 56 studies on social capital and socioeconomic inequalities in health found that social capital has a positive effect on health.18 A previous systematic review published in this journal on social capital and all mental illnesses, conducted in 2005 by De Silva et al,6 found that individual level cognitive social capital (ICSC) was associated with better mental health, no evidence of an association with individual structural social capital, and inconclusive evidence of an association between any measure of ESC and mental illness as the included studies were so diverse. However, all 21 included studies were cross-sectional, and it is plausible that the findings are due to reverse causality whereby people with mental health problems report lower levels of trust and reciprocity, rather than the low cognitive social capital causing mental health problems.6 The De Silva et al review included all mental illness, although most studies looked at CMD. Since 2005, many new studies on the association between social capital and CMD, including longitudinal studies capable of establishing the causal relationship between social capital and CMD, have been published, justifying this updated and more focused review.
This review aims to systematically review all published quantitative cross-sectional and longitudinal studies exploring the association between individual and ecological cognitive and structural social capital, and CMD.
Methods
Search strategy
This review was written in accordance with the PRISMA guidelines.19 The search strategy was designed to retrieve quantitative studies looking at the association between social capital and CMD. With the help of an information technologist, a search strategy was developed to search journals focused on epidemiology, public health, psychiatry and sociology in 10 databases up to July 2014. As different terms are sometimes used to describe social capital, we chose a wide range of terms such as ‘social cohesion’, ‘community participation’ and ‘social organisation’ to ensure that all relevant articles would be included. Owing to the large amount of studies retrieved, only peer-reviewed studies were included, and references of articles were not searched. Only English publications were included for logistic reasons. Online supplementary appendix A specifies the search terms and databases that were used to retrieve articles.
Study selection
The titles and abstracts of all retrieved articles were assessed by the first author against predetermined inclusion criteria. The second author was consulted when there was uncertainty. The criteria were predetermined based on the objectives of the review, and then iteratively revised by piloting these on a subset of the search results. Observational quantitative studies (cross-sectional and cohort) were included, excluding study designs without the ability to determine the relationship between social capital and CMD in an individual (such as ecological or qualitative studies). The separate disorders that comprise CMD were included (depression, anxiety, PTSD, etc), as were general scales that measure CMD holistically. Studies that did not use a validated tool to measure CMD were excluded, as were studies on other mental disorders such as psychosis, drug and alcohol use, and suicide. There were few studies on these mental disorders, and limiting the scope to CMD provided for a more homogenous synthesis of the studies. All studies that had appropriate definitions of social capital matching the definition in the Dictionary of Epidemiology8 and reflected in the measures listed in table 1 were included, whether or not they self-defined as measuring social capital. Studies defining their population as adults of both sexes from any setting were included. Studies on children were excluded, as the social capital definitions for children are often based on relations with family and peers. The quality of all studies meeting the inclusion criteria was evaluated using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies,20 and only studies of strong or moderate quality were included.
Data extraction
Data from included studies were manually extracted and summarised into tables. This included descriptive data about the setting, population and sample size, which aspect(s) of social capital were measured and the tools used to measure it, the validated mental health tool used to measure CMD, the type of analysis and the effect estimate for the association between each type of social capital and CMD.
The effect estimates were divided into ICSC, individual level structural (ISSC), ecological level cognitive (ECSC) and ecological level structural (ESSC) social capital. In order to create homogenous groups for synthesis, these divisions were made based on what the authors measured, and reflect the definitions from table 1 rather than the type of social capital defined by the authors. Multiple effect estimates were extracted from studies that measured more than one type of social capital (eg, ICSC and ISSC).
Data management and synthesis
The studies were too heterogeneous to enable a meta-analysis. Instead, a subgroup analysis based on the strategy developed by Ramirez et al21 was used. This comprised of adding up sample sizes of each study for each of the social capital subgroups (ICSC, ISSC, ECSC and ESSC) based on the effect that these had on CMD. The results were divided into whether higher social capital was significantly (p<0.05) associated with lower CMD (a negative association labelled−), whether there was no association (labelled/), or whether higher social capital was significantly associated with higher CMD (a positive association labelled+), and presented separately for cross-sectional and cohort studies. When multiple models presenting different confounders were included, the model controlling for the most amount of confounders was selected. Emphasis is put on the results of the cohort studies, as only these are capable of determining the direction of causality between social capital and CMD.
Results
Description of included studies
Figure 1 presents a flow chart of the selection process. In total, 1847 titles and abstracts were retrieved by the database search, of which 39 studies were included in the review: 31 cross-sectional and 8 cohort studies. These 39 studies yielded a total of 90 effect estimates—39 for ICSC, 31 for ISSC, 9 for ECSC and 11 for ECSC. The included studies were heavily biased towards high-income countries with 8 from North America, 7 from Scandinavia, 6 from Australia, 6 from Europe, 4 from East Asia, 5 from South America, 3 from Africa and 1 from South East Asia. Only 2 were from lower to middle income countries, 7 were from upper to middle income countries, and the remaining were from higher income countries.
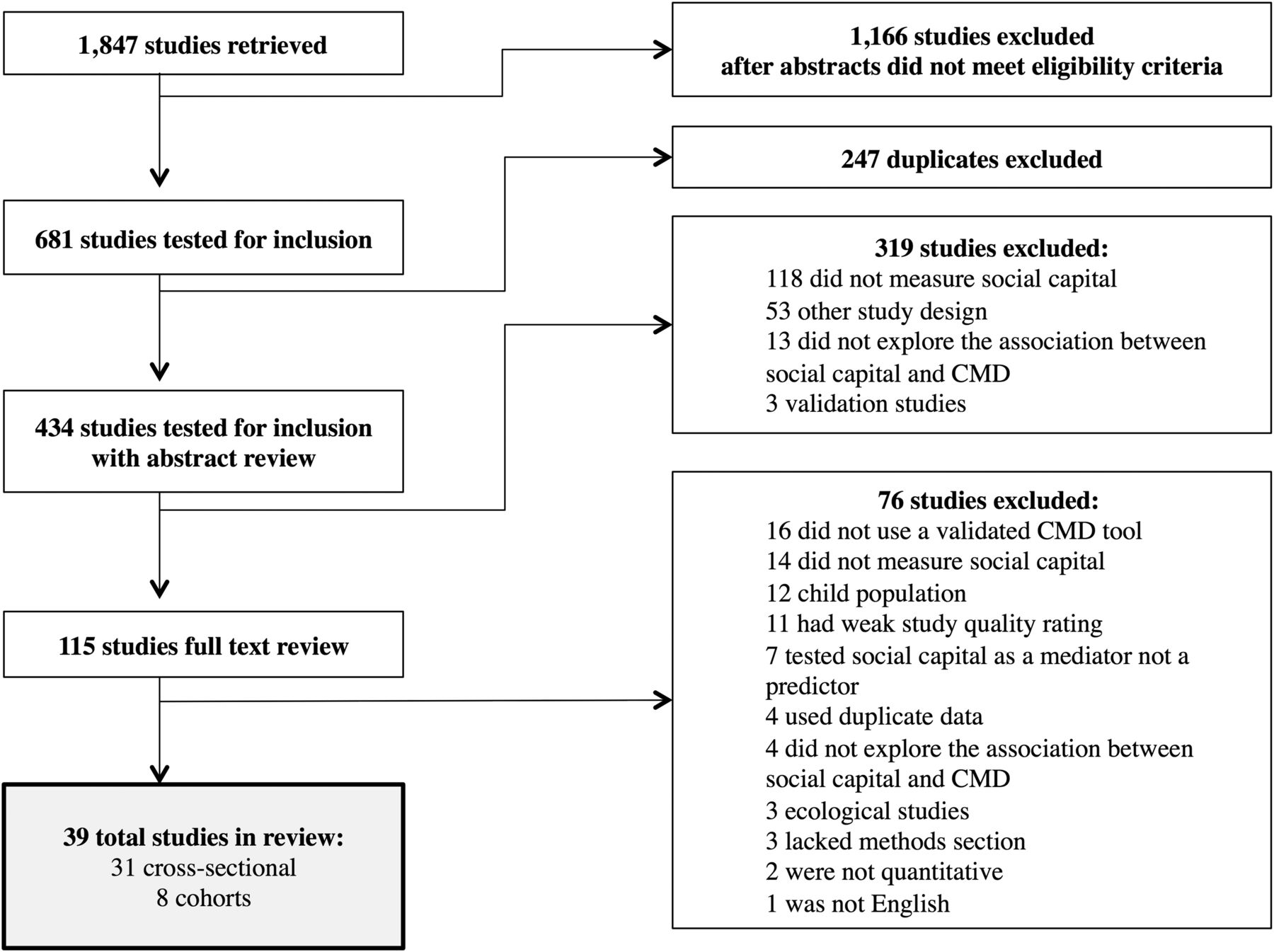
{kind=link}
Flow chart of study selection (CMD, common mental disorder).
All of the cohort studies measured social capital in adults without mental illness at baseline, and followed them up to see whether they developed CMD over time. The shortest follow-up was 6 months, and the longest was 7 years. Six cohort studies measured ISC, and two ESC. The results of the cohort studies are presented in tables 2 and 3, and the cross-sectional studies in online supplementary appendices B and C. Tables 4 and 5 present the synthesised results for each type of social capital by study design.
Description of individual level cohort studies
Description of ecological level cohort studies
Summary of effect estimates on the association between ISC and CMD
Summary of effect estimates on the association between ESC and CMD
Individual social capital
Thirty-three studies measured ISC, 27 of which were cross-sectional studies and 5 cohorts. There is strong evidence that high ICSC is associated with reduced risk of CMD. Results from the cohort studies provide good evidence that people with high ICSC have a lower risk of developing CMD. No study found that high ICSC was associated with worse CMD outcomes (table 4). Two of three cross-sectional studies found that high ICSC was associated with low CMD for visible minorities residing in high-income countries;29–31 2/2 found high ISSC associated with low CMD.30 ,32
The results for ISSC were more varied. The results from cross-sectional studies showed that the largest pooled sample sizes was from studies that showed no association between ISSC and CMD, at a ratio of nearly 5 to 1. Interestingly, there were three effect estimates from two studies that showed ISSC to be associated with a higher risk of CMD. The studies were from lower and middle income countries, namely Vietnam,15 ,32 Ethiopia and Peru.15 The six effect estimates from four cohort studies were inconclusive, with a roughly equal distribution of a positive association with CMD and no association.
Ecological social capital
A total of nine studies measured ESC, seven of which were cross-sectional and two cohorts. The cross-sectional studies provided strong evidence that higher ECSC is associated with lower risk of CMD (table 5). No cohort studies tested this relationship.
For ESSC, a similar pattern as for ISSC was observed, with the vast majority of the sample size showing no association, a smaller proportion a positive effect, and a minority a negative association. The negative association was found in Ethiopia, and showed that more support from individuals at the community level was associated with increased odds of CMD.15 The two included cohort studies used a one-dimensional measure of ESSC—voting rates. After controlling for confounders such as neighbourhood deprivation, neither study showed a significant effect on CMD.
Discussion
Discussion of results
This review provides strong evidence that ICSC is associated with CMD in cross-sectional studies, backed up by clear evidence from cohort studies that this relationship is not due to reverse causality and high cognitive social capital is protective against developing CMD. This pattern is repeated for ECSC, though all the included studies were cross-sectional.
The picture for ISSC is more mixed, with overall no association at either the individual or ecological level, but an indication from cross-sectional studies that in some low resource settings an individual's participation in civic activities is associated with an increased risk of CMD. This was only true in lower income countries. The study by Thuy and Berry explored the association between social capital and CMD in mothers of children with disabilities,32 while De Silva et al15 looked at social capital and maternal CMD in poor mothers with infants. In both cases, the mothers had large family responsibilities, and the authors hypothesise that participating in a high number of structural social capital activities, such as community groups, may have placed an additional burden on already over-stretched mothers.15
Most studies in this review focused on ISC, reflecting the more standard conceptualisation of social capital as an individual rather than ecological phenomenon, and also the relative ease with which ISC is measured compared to ESC. Scholars have suggested that both ISC and ESC be measured,15 ,33 as the two are not mutually exclusive.12 ,34–36 In this review, only three studies simultaneously controlled for both individual and ecological levels of social capital.15 ,29 ,37 Controlling for both ISC and ESC in the same model is important, as high levels of ESC might be more likely to benefit those who are trusting and socially active (those who have higher cognitive social capital) than those who are not.33
Risk of bias within and across studies
Within each study, there were different study designs, participants, eligibility criteria, methods, follow-up periods and analysis techniques. Some studies had special populations, and there were diverse cultural differences between groups. Social capital is made up of multiple components, and can be measured differently to be appropriate for different settings. All of these could lead to clinical, methodological and statistical heterogeneity in the findings of the review.
In addition, differences in the way social capital was measured in the included studies may affect the results of the review. First, the measurement of ESC was extremely varied across studies, ranging from one-dimensional ecological measures, such as voting rates,27 ,28 to ISC scores aggregated to the community level severely restricting the comparability of findings across the ESC studies.15 Despite these measurement differences, there were no clear differences in results between the studies that used aggregate measures versus single ecological measures in this review.
Cultural differences between settings affect the aetiology of CMD, and also the importance of different aspects of both individual and ESC afforded by different societies. For example, the effect of social capital on CMD might change in individualist and collectivist societies, as collectivist societies emphasise the interdependence between humans. Different types of social capital may also have varying importance in different cultures. Unfortunately the implications of diverse social and cultural settings could not be assessed due to a lack of information in the published papers, and also the difficulty of summarising complex cultural differences in a systematic review.
Strengths and Limitations of this review
This review is subject to limitations. First, these results are not generalisable to lower income countries as 30 of the 39 included studies were situated in high-income settings and within these, only 6 were in disadvantaged populations. Seven were from upper -middle income countries, and just two were situated in low-income countries. Second, the heterogeneity of the included studies meant that a meta-analysis to determine the pooled effect size of the cohorts was not possible. Although studies were pooled according to the direction of effect and weighted by sample size, the size of the protective effect of ICSC on CMD remains unknown. Lastly, there were potential sources of bias in the methodology of this review, including the possibility of publication bias as no grey literature was searched, and non-English language publications were excluded. In addition, authors were not contacted for information not contained in the published paper. Only one author reviewed the studies for inclusion, although the second author was consulted when the first was in doubt.
Despite these limitations, this review included a large number of studies, all of which were assessed as being of high quality by the EPHPP tool, which displayed a clear pattern of association between ICSC, ECSC and CMD. This review found that ICSC is protective against CMD, enabling others to investigate the use of ICSC for the prevention and promotion of CMD. Another important finding is that structural social capital may be more culturally specific as it is more dependent on cultural norms of behaviour, while harnessing cognitive social capital may be universally beneficial for preventing CMD as it relies more on the perhaps universal human emotions of reciprocity, trust and sense of belonging.
Recommendations for research
Further research is needed on the association between all types of social capital and CMD in low and middle income countries. More cohort studies should be conducted to explore how all forms of social capital affect the risk of developing CMD. Much more research is needed on ESC and CMD. Researchers should also look at current ICSC and ECSC interventions taking place for economic development or health, and consider how these could be used to prevent CMD.
Future studies should aim to use standardised and validated tools to measure social capital. This will allow better comparability between studies, and will increase the reliability and validity of social capital measures. One tool that could be used is the Adapted Social Capital Tool, more commonly known as the A-SCAT.38 A shortened version of this tool, the Short Adapted Social Capital Assessment Tool (SASCAT),39 was used by two different papers in this review to measure social capital in Ethiopia, India, Vietnam and Peru,15 ,40 and appears to be a comprehensive tool that could be used across low and middle income settings. A systematic review on measurement tools for social capital in low and middle income countries41 recommends the A-SCAT, Elgar et al's42 World Value Survey Social Capital Scale, and Hurtado et al's43 six-item tool.
Recommendations for practice and policy
Interventions to improve cognitive ISC and ESC with the aim of preventing CMD should be developed and tested, and existing social capital initiatives should measure the impact they may be having on mental illness. Many initiatives for social capital are already in place in higher income as well as low and middle income countries. Current antipoverty and development initiatives could be influencing mental health, but the effect is not measured. Adding a mental health component to existing programmes would not detract from these initiatives, but would dramatically increase the evidence base for the effect of social capital on mental health.
Many studies on social capital have found that trust is positively associated with economic growth, and that social divisiveness can result in reduced growth.3 ,4 ,40 Interventions aimed at improving social capital may be a cost-effective way of preventing CMD. Prevention and promotion initiatives focused on increasing ICSC can be protective against CMD in the long run.
What is already known on this subject
This is a comprehensive review and assessment of the evidence of the association between social capital and common mental disorder. This was needed, as no previous reviews have found conclusive evidence on the direction of the association between different types of social capital and common mental disorder.
What this study adds
This review shows that individual level cognitive social capital is protective against common mental disorder, and that ecological level cognitive social capital is associated with less risk of common mental disorder. This information is useful for future interventions aimed at preventing common mental disorder.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Mary De silva at @GMentalHealth
Contributors MJDS had the idea for the review. AME came up with the protocol, conducted the searches, extracted and compiled the data, completed the analyses, and wrote the discussion and conclusions. While AME wrote the bulk of the paper, MJDS offered her intellectual input and guidance through all stages, and had ideas on how to analyse the data, and also helped edit the final paper.
Funding MJDS was funded by an LSHTM/Wellcome Trust Fellowship. All data was available freely through King's College London, the London School of Hygiene & Tropical Medicine, and McGill University journal subscriptions.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.