Article Text

Abstract
Background The impact of early initiation of diabetes care soon after the identification of hyperglycaemia rather than leaving diabetes untreated on changes in glycaemic control has not been fully clarified. We aimed to quantify the effect of initiating and continuing diabetes care compared with not starting management of diabetes on short-term changes in glycaemic control among the Japanese with newly screening-detected diabetes.
Methods We retrospectively reviewed data from a nationwide claims database to assess histories of physician-diagnosed diabetes or hyperglycaemia, as well as the use of antidiabetic agents, blood testing for hyperglycaemia or dietary advice among individuals without a history of diabetes care. Changes in glycated haemoglobin (HbA1c) concentrations were evaluated using baseline data and data from a health examination during the following year.
Results Among 1393 individuals with newly screening-detected diabetes, 62% (n=864) did not initiate diabetes management during the follow-up period; 49.2% (n=425) of the untreated group had poor glycaemic control (HbA1c ≥7%) at the baseline examination. Only 38% (n=529) began diabetes management in medical settings. Individuals who remained untreated had a 1.87 (95% CI 1.38 to 2.52) or 1.63 (1.10 to 2.41) times higher risk of absolute increases in HbA1c ≥0.5% or ≥1%, respectively, compared with the treated patients, a difference that was significant. Making more frequent clinic visits especially after the first visit was dose-dependently associated with improved HbA1c levels compared with no diabetes management.
Conclusions In comparison with a lack of management of diabetes, immediately initiating and continuing diabetes care after identification of hyperglycaemia in a screening setting would contribute to clinically meaningful, improved glycaemic control in the Japanese.
- DIABETES
- SCREENING
- Clinical epidemiology
Statistics from Altmetric.com
Introduction
Evidence has shown the importance of glycaemic control in reducing the risk of the development of vascular complications in patients with diabetes1 ,2 and that intensive strategies to control blood glucose levels as early as possible would provide long-term effects on vascular complications, the so-called ‘legacy effect’ or ‘metabolic memory’.3 ,4
On the other hand, recent data showed that many patients with a previous diagnosis of diabetes did not receive diabetes care.5 ,6 Since data are not usually available on individuals who do not start management of diabetes soon after the identification of hyperglycaemia, evidence is scarce about how initiating early management of diabetes, rather than leaving the condition untreated, would benefit glycaemic control. A substantial lead time has been suggested between identification of diabetic hyperglycaemia and the initiation of diabetes control.7 ,8 Patients who do not start management of diabetes may experience a further deterioration of glycaemic control, although the detrimental effect of not receiving medical care for diabetes has not been clarified. In addition, the high dropout rate during medical treatment involving clinic visits is also an important issue.9–11 Clarifying the effect of keeping clinic appointments, particularly for a period after the first visits, would motivate patients to start and continue diabetes care in clinical settings that would contribute to more favourable glycaemic control that, in turn, might result in reducing the risk of the development of vascular complications. In Japan, taking a health examination is common in the general population and universal health coverage has been established nationwide.12 ,13 Therefore, under these conditions, we could review data on health examinations and in the nationwide claims database to quantify the effect of starting diabetes control on short-term changes in glycated haemoglobin (HbA1c) concentrations among individuals with screening-detected diabetes. Our aims in this study included (1) elucidating the impact of initiating early clinical management of diabetes versus leaving diabetes untreated on short-term changes in HbA1c concentrations and (2) quantifying the possible benefits of maintaining diabetes care on glycaemic control in comparison with not receiving treatment of diabetes in Japanese individuals.
Methods
Study participants
We retrospectively reviewed data on Japanese men and women who underwent a health examination and who had data on health insurance claims provided by a database vendor, Japan Medical Data Center Co., Ltd. (JMDC)14 (figure 1). Among 457 601 individuals who had at least one claim during the period from April 2009 to March 2010, 168 997 underwent a health examination. Of the 168 997 individuals, 35 710 had HbA1c ≥5.7% (National Glycohemoglobin Standardization Program, NGSP) and 4788 had HbA1c ≥6.5%. Those 4788 participants with elevated HbA1c values had received results of blood testing after the health examination. We used the HbA1c ≥6.5% criterion15 ,16 for screening-detected diabetes in this study since the HbA1c test could be used concomitantly for diagnosing diabetes and initiating diabetes monitoring.17 Among the 4788 individuals, we excluded 421 who did not have claims data because of lack of health insurance during the observation period. Then, according to the claims data, we excluded 2769 individuals who had a history of physician-diagnosed diabetes (International Classification of Diseases (ICD) codes, E10–E14) or hyperglycaemia (ICD code, R73), pharmacological treatment for diabetes (Anatomical Therapeutic Code, A10) or undergoing glucose tolerance tests, blood glucose measurements or HbA1c measurements in the previous 1 year before the baseline examination in hospitals. Among the remaining 1598 individuals who had no history of management of diabetes or hyperglycaemia, 205 did not undergo a health examination in the next year. As to the 205 individuals, we could not determine the exact reasons for their not taking the health examination; however, based on the claims database, we observed that 118 (57.6%) of those individuals did not start diabetes management and that 87 (42.4%) did start treatment of diabetes. Subsequently, a total of 1393 individuals were included in the current analysis.
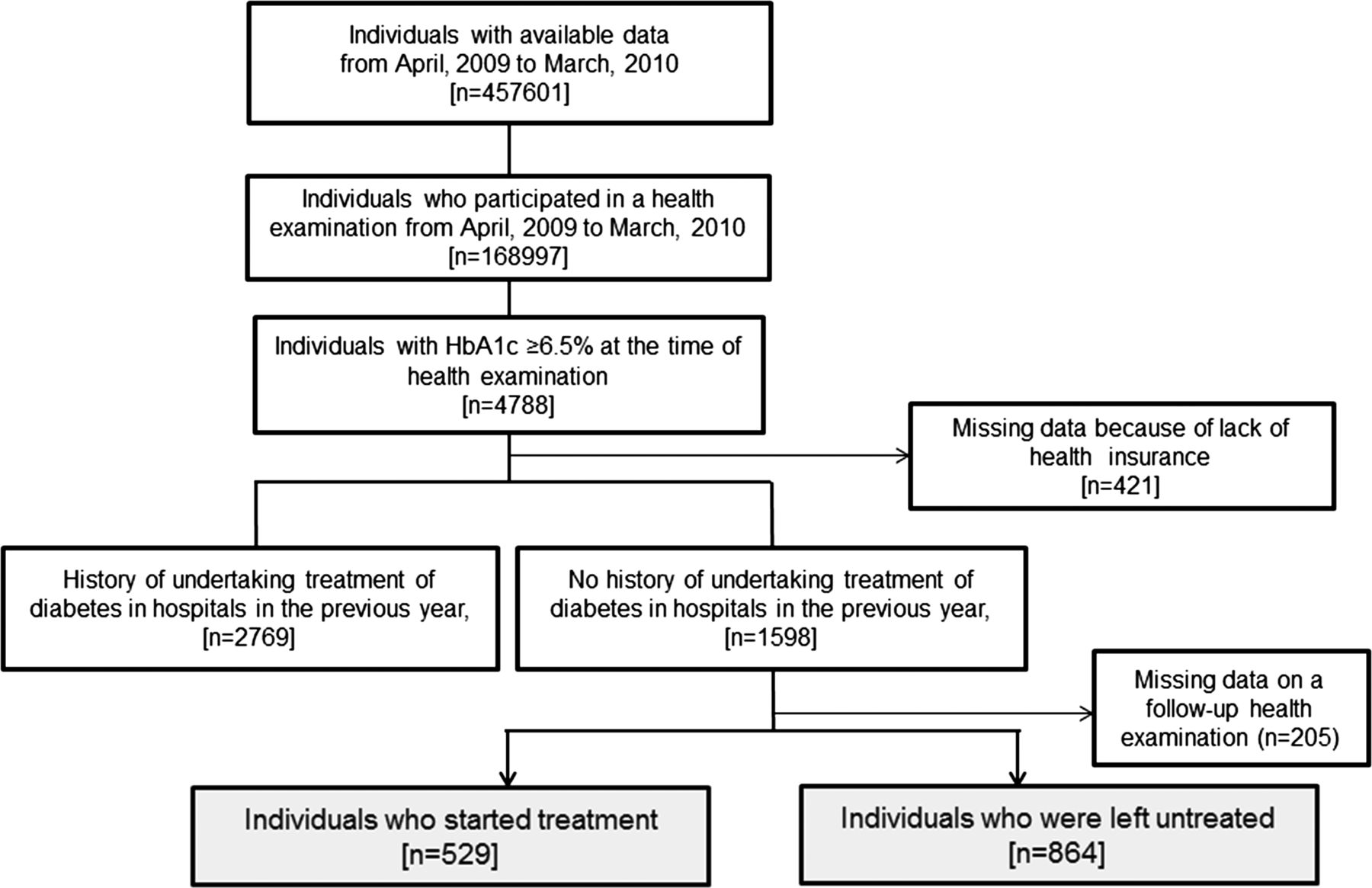
Flow chart of enrolment of participants in the study (HbA1c, glycated haemoglobin).
Assessment of initiation of medical treatment of diabetes using a claims database
To clarify the impact of starting diabetes management on short-term changes in HbA1c concentrations after the identification of diabetes, we examined data on the health check-up at the time of the baseline examination and at the follow-up in the next fiscal year. Initiation of diabetes care soon after the baseline examination was assessed using the nationwide claims database between the baseline examination and follow-up health examination in the next fiscal year. We assessed claims for physician-diagnosed diabetes or hyperglycaemia, antidiabetic agents, glucose tolerance tests, blood glucose measurements or HbA1c measurements by a month before the follow-up health examination after the baseline examination. Nutritional advice by a registered dietitian in outpatient visits during the observation period was also considered as the initiation of outpatient treatment. Then participants were classified into two groups according to whether they did or did not start diabetes management based on the claims database. Among the individuals who started treatment, we assessed who had a history of at least one hospital admission during the observation period.
Continuing outpatient treatment and the number of clinic visits
Among individuals who had outpatient treatment (without a history of hospital admission), we investigated the effect of the frequency of visits on HbA1c concentrations. We counted the number of outpatient visits during the overall observational time, specifically from the first visit to 3 months later or specifically from the first visit to 6 months later. We assessed the first diagnosis of either diabetes or hyperglycaemia and continuation of blood measurements of HbA1c or glucose concentrations, glucose tolerance tests, pharmacological therapy or dietary therapy on a monthly basis. If any one of these factors was observed, we considered that there was an outpatient visit during that month.
Changes in HbA1c concentrations between the baseline and follow-up examinations
Poor glycaemic control was indicated by HbA1c ≥7%. Elevations in HbA1c were indicated by absolute increases of ≥0.5% or ≥1% over baseline values or a relative increase of ≥20% for baseline HbA1c concentrations. Examples of such relative increases from baseline HbA1c concentrations would be 6.5% at the baseline examination and ≥7.8% at the follow-up examination, and 7% at the baseline examination and ≥8.4% at the follow-up examination. An absolute reduction in HbA1c was indicated by 1% or more. The value for HbA1c was estimated as the NGSP value (%) calculated by the formula HbA1c (%)=HbA1c (Japan Diabetes Society) (%)×1.02+0.25%.18
Statistical analysis
Logistic regression analysis was performed to calculate ORs and 95% CIs for changes in HbA1c concentrations. ORs were adjusted by age, sex and body mass index (BMI). We also examined whether results were independent of the HbA1c levels at the baseline examination or being treated with antidiabetic agents. Analysis was performed with IBM SPSS Statistics V.19, and statistical significance was considered as p<0.05.
Results
Among the 1393 individuals with screening-detected diabetes, 62% (n=864) had no history of initiating treatment or management of diabetes and only 38% (n=529) started treatment in clinical settings (figure 1). The mean (SD) HbA1c value was 7.75% (1.57%) in individuals who started treatment and 7.70% (1.66%) in those who did not receive treatment (table 1). In the treatment group, we observed that 56.7% (n=300/529) had poor glycaemic control of HbA1c ≥7% and 11.5% (n=61/529) had HbA1c ≥10% at the baseline examination. The prevalence rate of HbA1c ≥7% was also high (49.2%) among individuals who did not start management of diabetes.
Characteristics of the 168 997 individuals who underwent a health examination and the 1393 individuals with elevated HbA1c ≥6.5%
Figure 2A shows the association between baseline HbA1c and changes in HbA1c concentrations among the individuals who did not receive treatment and those who initiated treatment. Most of the untreated patients with high HbA1c at the baseline examination did not experience a large reduction in HbA1c concentrations at the follow-up examination. However, individuals who started diabetes management showed a trend towards a large reduction in HbA1c concentrations, particularly among those with poor HbA1c values. A large reduction in HbA1c was observed in individuals who had only outpatient treatment (n=398) and those who had a history of inpatient treatment (n=131; figure 2B). Among the 398 individuals who started outpatient treatment, 304 had HbA1c measurement(s), 334 had glucose measurement(s) and 32 had glucose tolerance test(s) at least once in clinical settings. Also, 75 had received dietary advice by a dietitian and 97 had started treatment with antidiabetic agents. We also examined the association between baseline HbA1c and HbA1c changes among the 398 outpatients according to the presence or absence of the use of antidiabetic agents (figure 2C). Antidiabetic agents were more likely to be used in participants with substantially high HbA1c values at the baseline examination and large changes in HbA1c concentrations were based on the prescription of antidiabetic agents.

{kind=link}
{kind=link}
Changes in glycated haemoglobin (HbA1c) concentrations at the health examination in the year after detection of diabetes according to HbA1c concentrations at the time of the baseline health examination. (A) Open circles, participants who were left untreated; closed circles, participants who started treatment. (B) Participants who started treatment. Open circles, patients with a history of inpatient treatment; closed circles, outpatient treatment. (C) Participants who started outpatient treatment. Open circles, initiation of pharmacological treatment; closed circles, without initiation of pharmacological treatment.
The mean (SD) change in HbA1c concentration between the baseline and follow-up health examination was −0.6% (1.5%) in patients who started treatment and 0% (1%) in those who did not receive treatment (table 2). The probability of elevation in HbA1c ≥0.5% (table 2, A) or HbA1c ≥1% (table 2, B) was 1.91 (95% CI 1.42 to 2.57) times or 1.72 (1.17 to 2.53) times higher, respectively, in the untreated group compared with the treated group. Adjustment for age, sex, BMI and HbA1c values at the baseline examination did not alter the association. Individuals in the untreated group had an adjusted OR of 1.87 (1.38 to 2.52) for a ≥0.5% increase or an adjusted OR of 1.63 (1.10 to 2.41) for a ≥1% increase compared to the outpatient treatment group. From the results of our assessment of a relative increase of ≥20% for baseline HbA1c concentrations (table 2, C), ORs for increasing HbA1c concentrations were 1.72 (1.005 to 2.94) in the unadjusted model and 1.65 (0.96 to 2.85) in the adjusted model. When we performed an analysis using the group of patients who started outpatient treatment as a reference and calculated ORs, individuals who were left untreated experienced an approximately two times elevated risk of deteriorating HbA1c concentrations in each definition of A, B or C (see online supplementary table S1).
Changes in HbA1c concentrations between baseline and follow-up health examinations and OR for increases in HbA1c concentrations among the untreated diabetic group in comparison with the outpatient treatment group
A dose-dependent association was observed between frequency of visits and reduction in HbA1c concentrations among patients who started outpatient treatment and those who were left untreated (n=1262; table 3). Although only one clinic visit was associated with an adjusted OR of 1.99 (1.10 to 3.60) for a reduction in HbA1c concentrations (≥1% or more) compared with no visits (untreated group), two or more visits were associated with a high probability of reducing HbA1c concentrations with an adjusted OR of 4.40 (2.53 to 7.65), independently of age, sex, BMI, HbA1c at the baseline examination and treatment with antidiabetic agents. Results were fundamentally the same if we excluded individuals with a history of prescription of antidiabetic agents. Further, frequent follow-up clinic visits especially during the period of up to 3 months or up to 6 months after the first visit were also dose-dependently associated with a reduction in HbA1c concentrations independently of age, sex, BMI and HbA1c at the baseline health examination. Results regarding the OR for a reduction in HbA1c ≥1% remained significant if we adjusted for the prescription of antidiabetic agents. We made a similar observation in results of our additional analysis using a different definition of HbA1c reduction (a relative reduction of ≥20% in the baseline HbA1c concentration; data not shown).
Effect of number of physician visits (monthly basis) on probability of reduction in HbA1c concentrations (1% or more) at the next health examination among individuals who started outpatient treatment in comparison with those who were untreated
Discussion
In this study of Japanese individuals with newly screening-detected diabetes, individuals who did not start management of diabetes experienced an almost 1.5–2 times higher risk of deterioration of glycaemic levels than those who promptly started diabetes care. Those individuals who initiated diabetes care experienced clinically meaningful short-term reductions in HbA1c concentrations compared with those who were not treated for diabetes. This association was independent of treatment using antidiabetic agents or baseline HbA1c concentrations. Additionally, our results indicated that more frequent follow-up visits, particularly after the first outpatient visit, were dose-dependently associated with improved HbA1c levels in comparison with no visits.
Considering that many patients with known diabetes do not receive treatment,5 ,6 our results underscore the importance for both healthcare professionals and patients of starting diabetes management soon after the identification of hyperglycaemia by screening. Also, our data would contribute to constructing preventive or screening strategies for diabetes using HbA1c concentrations and the subsequent initiation of diabetes care. According to data from the Epidemiology of Diabetes Interventions and Complications follow-up study to the Diabetes Control and Complications Trial, early intensive diabetes therapy would have long-term beneficial effects on the risk of cardiovascular disease in patients with type 1 diabetes.4 The legacy effect of early glycaemic control has also been shown in patients with type 2 diabetes.3 The UK Prospective Diabetes Study showed that each 1% reduction in HbA1c concentration was associated with a 37% decreased risk of microvascular complications, a 14% decreased risk of myocardial infarction and a 21% decreased risk of any end point or death related to diabetes among newly diagnosed patients with type 2 diabetes.2 Although our data could only show the short-term benefit of glycaemic control after the initiation of diabetes care, our results could motivate people to start early treatment of diabetes. Results of the multicentre Anglo-Danish-Dutch Study of Intensive Treatment In People with Screen Detected Diabetes in Primary Care showed that intensive management of patients with type 2 diabetes detected by screening was associated with improvements in cardiovascular risk factors, but was not significantly associated with reductions in the incidence of cardiovascular events or death over 5 years.19 Further investigations are needed to clarify the impact on microvascular and macrovascular complications among those who received early diabetes care in comparison with those left untreated.
Among patients with diabetes, it was reported that only 25.8% received treatment for diabetes and that only 39.7% of those treated had adequate glycaemic control (HbA1c <7%) in a Chinese population.5 We observed that about 50% of individuals with screening-detected diabetes had poor glycaemic control and that a large number of study participants with elevated HbA1c did not receive diabetes treatment. Also, our data suggested that patients with very poor glycaemic values could not be expected to have improved HbA1c concentrations without treatment by healthcare professionals. Although we could not determine the reasons for not starting diabetes care from our data, according to data from the National Health and Nutrition Examination Survey in Japan, the most frequently cited reasons for not initiating diabetes care was the absence of any particular pain or symptoms.6 The development and progression of diabetes takes place over a long asymptomatic period with a gradual increase in HbA1c over the years before the diagnosis of diabetes.20 Studies of individuals with newly diagnosed diabetes or screening-detected diabetes found that these individuals had early diabetes-related tissue damage during the preclinical stage.21 ,22 Healthcare professionals should provide information to patients with screening-detected diabetes on the importance of initiating diabetes care in clinical settings as early as possible, rather than awaiting test results of a subsequent health check-up without appropriate treatment by a physician.
As to the issue of how frequently patients should be followed, a retrospective study that included patients with diabetes who were treated by primary care physicians showed that encounters every 2 weeks might be associated with the most rapid achievement of goals for HbA1c and other metabolic factors.23 Our previous analysis of patients with diabetes under specialist care showed that they experienced substantial improvement, especially in glycaemic control, as early as a few months after the first visit.11 However, the effect of the frequency of visits was only investigated among patients who were treated in clinic, and therefore no comparisons could be made with individuals who made no visits.11 ,23 In this study, we showed that keeping follow-up clinic visits after the first visit would contribute to more favourable glycaemic control compared with not initiating treatment. Whether this pattern of diabetes care would contribute to reducing the risk of the development of vascular complications should be investigated further.
Inpatient diabetes education has been noted to play an important role in diabetes care,24 ,25 although it might be common to offer intensive education programmes for diabetes care during outpatient visits. Results of a recent study of a Western population suggested that inpatient diabetes education was associated with less frequent hospital readmissions of patients with poor glycaemic control.26 It was also reported that compared with hospitalised patients with diabetes who received usual care, those who received intensive care by a diabetes team tended to have a shorter hospital stay and achieved better glycaemic control.27 As to the inpatient treatment group in our study, not all of these participants were hospitalised throughout the entire follow-up time. As our study was not an intervention study, treatment approaches differed according to the individual patient and physician. It would be necessary to investigate the effectiveness of inpatient diabetes education in comparison with usual care in outpatient visits considering the cost-effectiveness of each treatment programme.
The strengths of our study include the objective assessment of the history of diabetes care based on a nationwide claims database as well as quantifying glycaemic changes over a 1-year period in a large number of individuals with screening-detected diabetes according to their pattern of follow-up care. The limitations are that we cannot completely deny the possibility of misclassification of participants based on the definitions used in our study. Our study was limited to the assessment of changes in HbA1c concentrations; thus, a further extensive study to explore the impact of prompt diabetes management on cardiovascular risk factors or vascular complications is warranted. Since our study was conducted specifically in Japanese individuals, further investigations would be needed among other ethnic populations in different healthcare systems to confirm our findings.
In conclusion, early management of diabetes resulted in clinically meaningful short-term reductions in HbA1c concentrations compared to leaving the condition untreated. Individuals who did not start diabetes management in medical settings did not experience reductions in HbA1c concentrations. Compared to not receiving diabetes treatment, initiating diabetes treatment after identification of hyperglycaemia and further continuing diabetes management were shown to benefit short-term glycaemic control.
What is already known on this subject
-
Recent data showed that many patients with a previous diagnosis of diabetes did not receive diabetes care.
-
Evidence is scarce about the benefits of initiating early management of diabetes on short-term glycaemic control among newly screening-detected patients with hyperglycaemia compared with leaving the condition untreated.
What this study adds
-
Compared to no diabetes treatment in medical settings, initiating diabetes treatment soon after identification of diabetic hyperglycaemia by a health examination and further continuing diabetes management were shown to benefit short-term glycaemic control.
-
Healthcare professionals should provide information to patients with screening-detected diabetes on the importance of initiating diabetes care in clinical settings as early as possible, rather than awaiting test results of a subsequent health check-up without appropriate treatment by a physician.
Acknowledgments
All authors thank Mr Shinya Kimura, Ms Rie Nishikino and the staff members at the Japan Medical Data Center Co., Ltd, for their assistance in data preparation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors YH and HS contributed to the study concept and design, critical revision of the manuscript and study supervision. HS contributed to the acquisition of data, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis All authors contributed to the analysis and interpretation of the data, statistical analysis, drafting and writing of the manuscript and approved the final version of this article.
-
Funding This work is financially supported in part by the Ministry of Health, Labour and Welfare, Japan. HS and YH are recipients of a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.
-
Competing interests None.
-
Ethics approval The study protocol followed the Japanese Government's Ethical Guidelines Regarding Epidemiological Studies in accordance with the Declaration of Helsinki and was reviewed by the Institutional Review Board at the School of Medicine, Faculty of Medicine, Niigata University.
-
Provenance and peer review Not commissioned; externally peer reviewed.