Article Text

Abstract
Background To investigate whether school performance is a risk factor for suicide death later in life and, if so, to what extent this is explained by intergenerational effects of parental education.
Methods This population-based cohort study comprises national birth cohorts between 1972 and 1981 in Sweden. We followed 898 342 students, graduating between 1988 and 1997 from the 9 years of compulsory school, equivalent to junior high school, until 31 December 2006, generating 11 148 758 person-years and 1490 suicides. Final school grades, in six categories, and risk of suicide were analysed with Poisson regression.
Results The incidence rate ratio (RR) for suicide death for students with the lowest grades was 4.57 (95% CI 2.82 to 7.40) for men and 2.67 (1.42 to 5.01) for women compared to those with highest grades after adjustment for a number of sociodemographic and parental morbidity variables, such as year of graduation, parental education, lone parenthood, household receiving social welfare or disability pension, place of schooling, adoption, maternal age and parent's mental illness. Students with grades in the middle categories had RRs in between. These relationships were not modified by parental education.
Conclusions The strong association between low school grades and suicide in youth and young adulthood emphasises the importance of both primary and secondary prevention in schools.
- Suicide
- school performance
- adolescence
- register
- Sweden
Statistics from Altmetric.com
Introduction
The suicide rate in many western countries has decreased during the last couple of decades. However, for young people aged 15–24 years the decline is not as clear. The suicide rates (6.6 and 11.9 per 100 000 inhabitants for female and male adolescents, respectively) in Sweden are moderately high compared to other western European countries.1 Therefore, it is of great importance to investigate and establish possible risk factors for young adults.
School is an important arena in young persons' everyday life and success as well as failure may influence psychological stress and self-esteem—factors that are associated with suicide risk.2 3
School performance is easily measured, at least in terms of school grades, and may potentially be used in secondary prevention to identify those at-risk for suicide. However, studies elucidating the relation between school grades and psychiatric health and suicide are scarce. A few previously published studies show that poor school performance is more common among suicidal youths.4–8 Alaraisanen et al found in their study of 11 017 individuals that good school performance was associated with decreased suicide risk. However, a majority of earlier studies used small sample sizes and might be unrepresentative for the general population. Most also suffer from lack of adjustment for major confounders. It is difficult to disentangle the mental health effects of school grades per se because school success is associated with several conditions that themselves are important determinants of suicide in youths and young adults. Socioeconomic living conditions of the childhood household, such as parental educational level, place of residence, financial stress, lone parenting, intergenerational effects of parental psychiatric illness and addiction, determine mental health as well as school performance.9 10 To a certain extent these influences, in interaction with genetic traits, are probably mediated by cognitive competence, as measured by IQ, where lower IQ has been demonstrated to be a risk factor for suicide.11 12
The aim of this study was to assess whether low grades after 9 years of compulsory school, equivalent to junior high school, increased the suicide risk. Furthermore, we assessed whether childhood socioeconomic status measured as parental education modified this relation. It is possible that having low grades may, for instance, have more detrimental effects on self-esteem and psychological stress among youths in highly educated families due to presumably higher expectations of school success. However, children brought up in a less supportive environment under more negative socioeconomic conditions may suffer from a general susceptibility to psychological stress.
Swedish national registers makes it possible to create large study populations with information about school grades as well as a broad range of background variables. In this study we used these resources and studied 898 342 students born between 1972 and 1981 and followed them from 15 to 25–35 years of age.
Materials and methods
Study population
We used the unique personal identity number assigned to each Swedish resident (about 9 million in total) to link together information from six population-based registers.13
We selected all Swedish residents born between 1972 and 1981 (N=1 073 684) from the Total Population Register held by Statistics Sweden. At least one parent had to be born in Sweden (904 300 individuals). We excluded students who had been treated as an inpatient for substance abuse and psychiatric inpatient care before graduation (n=4234; 0.4%). After excluding also those who died before the age of 15 years (n=1724; 0.2%), our final cohort consisted of 898 342 individuals. The follow-up period lasted from 1 July, the year of graduation, to 31 December 2006, generating 11 148 758 person-years in total. Thus, the incidence of suicide was measured from the age at graduation (usually 15 y) until age 25 years for those graduating in 1997 and until age 34 years for those graduating in 1988.
School grade
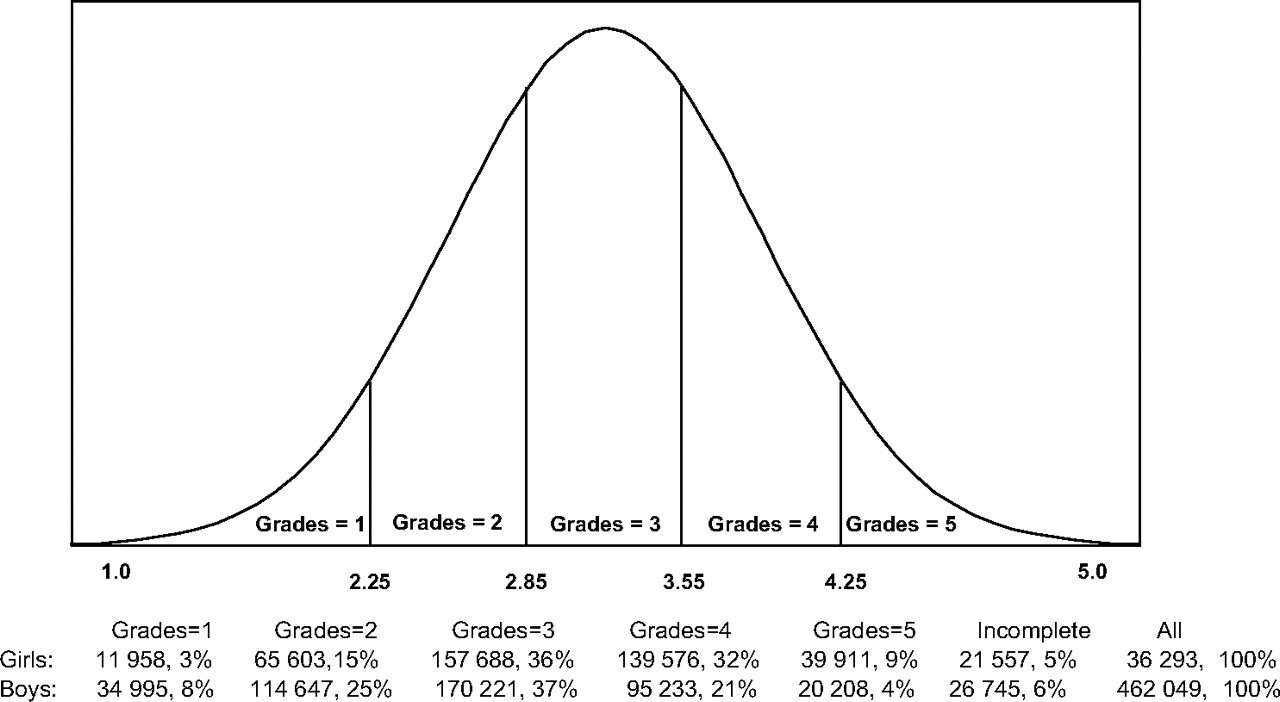
School grades from the National School Register, which is administered jointly by the Swedish National School Administration and Statistics Sweden, were used to calculate grade point average, referred to as grades, for all students. This register encompasses information on each individual's educational achievement—that is grades by subject as well as grade point average for all students graduating from the 9th year since 1988. During the period 1988–1997 the school system used a normally distributed scale of five grades 1–5 (where 5 is highest) with the presumption that school achievements are dispersed according to a normal distribution with mean 3.0 and SD 1.0. The National School Administration supervises the grading system through national examinations. Grade in gymnastics was, according to national rules, excluded if it lowered the average grades. The grades for the cohort studied ranged from a minimum of 1.0 to a maximum of 5.0. Mean for the whole country was supposed to be 3.0. However, during the whole time period our cohort had a mean of 3.2 with SD 0.7. We classified school grades into six groups where ‘incomplete’ contains all students who finished school without complete grades regardless of whether they attended regular or special school (figure 1).
{kind=link}
Distribution of the six different grade groups, numbers and per cent by sex.
Suicide
Suicide was defined as having an underlying cause of death in the Causes of Death Register coded according to the International Classification of Diseases (ICD) as (ICD–9: E950–E959; ICD–10: X60–X84) or as death with uncertain intent (ICD–9: E980–E989; ICD–10: Y10–Y34). With our definition of suicide, including deaths with uncertain intent, our aim was to minimise spatial and secular trends in detecting and classifying cases of suicide.14
Effect modifiers and confounders
We obtained parental highest attained educational level, from the Swedish Population and Housing Census 1990, which was a mandatory nationwide census conducted every 5 years between 1960 and 1990. Parental educational level was classified into four categories as seen in table 1. For households with two adults, we chose the highest educational level to characterise the household.
Number of students' grade point average, suicides and suicide rates per 100 000 person-years for the studied covariates
Admission to hospital for psychiatric diagnoses in the National Patient Register before graduation defined the parents as having been treated as psychiatric inpatients.
Information about lone parenthood was obtained from the Census 1990. For those who graduated in 1988 and 1989 the Census from 1985 was used. We collected information on whether the household received social welfare or if any parent received disability pension, during the year of graduation or the previous year, from the Total Enumeration Income Survey, which contains data on the income and subsidies of all Swedish residents.
We categorised place of schooling into three groups according to the degree of urbanisation (table 1).
Information on adoption was retrieved from the Multi Generation register, which contains all known relations between children and parents (born 1932 or later) since 1961.
Statistical analysis
We used the incidence rate ratio to estimate the relative risk (RR), through performing multivariate analyses by Poisson regression with suicide as the dependent variable. We assessed person-years at risk by adding up the years the individuals were alive and living in Sweden during the follow-up period (1 July of the year of graduation, because graduation is in June, to 31 December 2006). SAS Genmod procedure was used to calculate RRs and 95% CIs for suicide with the highest grade (5) as the reference group. SAS version 9.1 was used.
We studied women and men separately and considered all adjustment variables as possible confounders since they all occurred before the graduation. None of the variables were regarded as operating contemporaneously between graduation and the outcome of interest (mediators).
In the first model, adjustment was made only for the year of graduation, which was regarded as crude rates. In the second model we added variables that, to different degrees, reflect the social and psychological childhood environment: parental education, lone parenthood, household receiving social welfare or disability pension, place of schooling, adoption and maternal age. Model III was adjusted for year of graduation, parent's mental illness and parent's substance abuse, while all covariates were included in the final model (IV).
To analyse effect modification from parental education we dichotomised this variable with 12 years of education or more in the highest category.
Results
In table 1 the number of suicides and suicide rates for the studied covariates for all 436 293 women and 462 049 men in the study are presented.
During the follow-up period from July 1988 until December 2006 there were a total of 1490 suicides: 414 women and 1076 men of which 20% were deaths with uncertain intent. Mean age at suicide was 23.8 for both genders. The overall suicide rate was more than twice as high among men compared to women (crude rates 18.7 and 7.7 per 100 000 person-years, respectively). Students from households with higher education had higher school grades and tended to have slightly lower rates of suicide. Adopted children had more than twice the suicide rate compared to children not adopted.
The crude RRs (adjusted only for year of graduation) displayed a gradual increase of suicide risk with decreasing levels of grades in both women and men (model I, tables 2 and 3). In model II, adjustments for family living conditions—that is, parental education, lone parent status, receipt of social welfare or disability pension, place of schooling, adoption and maternal age—resulted in only modest attenuations of the increased risks.
Grade point average and the risk of suicide, women
Grade point average and the risk of suicide, men
Adjustment for parental hospital admissions because of psychiatric disorders (model III) generated very similar results as model I. In the fully adjusted model IV, the school grade gradient remained for both women and men. In all models, students with incomplete grades had the highest suicide risks. We also performed the same analysis with only certain suicide as outcome and obtained similar risks and gradients (data not shown). In a restricted analysis we only followed our cohort until age 20 years. This resulted in similar RRs for men but slightly lower for women.
In the stratified analysis (table 4) we found that the effect of having low grades was not modified by parental educational level.
Grade point average and the RR of suicide, by parental education
Discussion
Our findings in 898 342 students from junior high school showed that school failure in terms of low school grades implies a substantial increase in the risk of suicide. The increased risk remains, with a clear gradient, for lower compared to higher grades even after adjustments for a range of possible confounders, such as family psychiatric illness, low family educational level, receipt of social welfare, being adopted or living in a lone parent household. The effect of having low average grades seems to be independent of parental educational level.
The strengths of the study include the nationwide cohort design, the complete coverage of school grades and suicides, together with linkage of numerous potential confounders made possible by the unique personal identifier assigned to each Swedish resident.
Since having an immigrant background and/or a non-Swedish ethnicity has been demonstrated to influence school performance15 as well as suicide risk,16 we restricted our analyses to those having at least one Swedish-born parent. Our study did not include the detailed data about psychiatric morbidity that would have made it possible for us to fully study the importance of psychiatric disorders for the association between school grades and suicide. Although the most severe hospitalised psychiatric cases in the study population with an onset during childhood and school years were excluded from the study, milder psychiatric conditions have been found to be quite prevalent in school children. Depression has been found to be associated with heritable traits and adversity in early childhood, but also with deteriorated school performance during the school years and self-harm in youth and young adulthood.17 Poor school performance may increase the risk of suicidal actions in a student with depressive traits.18 Other psychiatric conditions, such as anxiety disorder19–21 and attention-deficit hyperactivity disorder combined type,22 which have been found to be associated with educational problems as well as suicidal behaviour, can be expected to have similar complex interaction patterns with self-harm and school performance. If we could capture and adjust for all mental ill health in childhood, the relationship between school grades and suicide might weaken. Besides our lack of data on mental health issues, another limitation is our lack of indicators of alcohol and drug abuse during the school years. To be able to establish the causality of the association between school grades and suicide risk, longitudinal studies of mental health during the school years and school performance is needed.
Antisocial behaviour and conduct disorder are risk factors for poor school performance as well as suicide, which we could not control for in this study. These markers may have partly explained the highly increased risks in the groups with very low or incomplete grades, although it is probably not suffice to explain the clear gradient in suicide risk from highest to lowest grades.
There was no indication that parental education to any greater extent affected the association between school grades and suicide.
It seems probable that the main mechanisms responsible for this strong gradient are complex interactions of school performance with a number of other determinants of mental health. In a life course perspective, school performance and mental health in youth share hereditary, prenatal and early childhood determinants with an onset prior to school entry. During the years in school, socioeconomic living conditions as well as peer, teacher and family relations have an impact on school performance as well as on mental health.
Having low school grades means that many future career doors are closed, since school performance is important for the individual's access to higher education and, thereby, also for future career opportunities, future income and future socioeconomic position. Therefore, school failure could lead to more financial struggles and stress, which may increase the suicide risk.
Low school grades may lead to low self-esteem and feelings of stigmatisation. Young student's feelings of anger, hopelessness and sadness can negatively colour their beliefs about themselves and their future, including their self-image and beliefs of being able to be academically successful or not.23 Bursztein also emphasises the strong relationship between adolescent's aggression and impulsivity and suicide risk.24 Individuals with poorer school grades might run a higher risk for increased psychological stress and lower self-esteem, which alone is a well-known risk factor for suicide.2 3
Low school grades may also imply lower IQ and, thereby, a proxy for an individual's ability to cope, which could influence one's ability to embrace health education. IQ has been demonstrated to be an important predictor for suicide and suicide attempts.18 25–28 The magnitude of the gradient of school grades to suicide in our study was considerably greater than the gradient found in a previous Swedish study of IQ tests at military conscription as a predictor of suicides in men.26 It has also been shown that male international adoptees generally perform better in school than expected by their cognitive competence measured as IQ test at conscription.29 This demonstrates that grades are not merely proxy indicators of IQ, although the two concepts may capture similar mechanisms. Further, Lekholm et al analysed influences on school grades and found that non-cognitive student characteristics, such as motivation and parental engagement, to a large extent influence school grades.30
This study is also in line with previously reported increased risk of suicide in international adoptees in Sweden.31 Pre-adoption circumstances of abuse and institutional neglect have been presumed to be the main causes behind this increased risk.
Based upon the present findings of 898 342 individuals, we conclude that poor school performance seems to be a risk factor for suicide among both women and men and regardless of parental education. Thus, we would like to emphasise the importance of both primary and secondary suicide prevention. In primary prevention, different educational methods/strategies need to be considered regarding both students' self-esteem and capability and thereafter evaluated in a public health perspective that includes suicidal behaviour. One may speculate that methods to instruct students with major and minor learning problems would be a crucial point in such an evaluation, but also the opportunities available for secondary schooling to prepare students with learning problems for entrance on the labour market. In secondary prevention it seems important to identify and treat students with psychiatric disorders in school before they cause detrimental effects on school performance.
Finally, we would like to emphasise the need of further research on this topic and also the importance of qualitative research that hopefully can explain more of the mechanisms behind this result.
What is already known on this subject
Former studies have indicated that adolescences with poor school grades run a higher risk of committing suicide than their peers. However, most studies lack adjustment for major confounders, are small and may be unrepresentative for the general population.
What this study adds
In this nationwide study we found that poor school grades increase the suicide risk and, in analyses of six different grade levels, we found a gradient showing that students with second highest grades run a higher risk of suicide than students with the very highest grades and so forth.
Acknowledgments
We thank Professor Bo Vinnerljung for excellent advice.
References
Footnotes
Funding The Swedish Council for Working Life and Social Research financially contributed to part of the correspondent author's salary.
Competing interests None.
Ethics approval This study is approved by the ethical committee dnr: 60-5075/2007 at Karolinska Institute, Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.