Article Text

Abstract
Objective: To examine the relation of scores on tests of mental ability across childhood with established risk factors for premature mortality at the age of 30 years.
Methods: A prospective cohort study based on members of the British Cohort Study born in Great Britain in 1970 who had complete data on IQ scores at five (N = 8203) or 10 (N = 8171) years of age and risk factors at age 30 years.
Results: In sex-adjusted analyses, higher IQ score at age 10 years was associated with a reduced prevalence of current smoking (ORper 1 SD advantage in IQ 0.84; 95% CI 0.80, 0.88), overweight (0.88; 0.84, 0.92), obesity (0.84; 0.79, 0.92), and hypertension (0.90; 0.83, 0.98), and an increased likelihood of having given up smoking by the age of 30 years (1.25; 1.18, 1.24). These gradients were attenuated after adjustment for markers of socioeconomic circumstances across the life course, particularly education. There was no apparent relationship between IQ and diabetes. Essentially the same pattern of association was evident when the predictive value of IQ scores at five years of age was examined.
Conclusions: The mental ability–risk factor gradients reported in the present study may offer some insights into the apparent link between low pre-adult mental ability and premature mortality.
- mental ability
- risk factors
- mortality
Statistics from Altmetric.com
Although psychometric tests of mental ability (IQ tests) have been most commonly utilised in educational environments,1 in the past five years the association of mental test scores with all-cause mortality has been examined in the recently established field of cognitive epidemiology.2 A systematic review identifying nine population-based cohort studies with extended follow-up of child and young adult groups into middle and older age found that low scores on early tests of mental ability were associated with elevated all-cause mortality rates.3 The consistency of this observation across the identified studies has inevitably led to some conjecture regarding the mechanisms responsible.3–7 One such potential pathway is the influence of early life mental ability on established adult risk factors for premature mortality that may mediate the ability–mortality gradient, including smoking,8 obesity and overweight,8–10 diabetes,11 and raised blood pressure.8 12
There is a scarcity of data linking early life mental ability with such later risk factors for premature mortality.3 In separate Scottish cohorts, there was a suggestion that childhood mental ability was associated with smoking cessation whereas results for uptake were discordant.13 14 In those studies, and in a report from Scandinavia,15 higher mental ability scores in childhood also appeared to offer protection against raised blood pressure in later life. For the most examined risk factor, obesity/overweight, the link with ability is discrepant across a series of analyses.16–21 In the only study examining the link between pre-adult IQ and later diabetes risk of which we are aware, there was no suggestion of a gradient.14
Some of the studies are subject to limitations that hamper data interpretation. First, those examining the relation of early life mental ability with a single risk factor in isolation, rather than a range, restrict insights into the specificity of any relationships. Second, studies sometimes lack data on socioeconomic position. As a correlate of IQ,1 socioeconomic position may therefore be a confounder or mediator in the IQ–risk factor association, depending on the period of measurement relative to this psychological characteristic.2 Third, most studies are small in scale, leading to suboptimal statistical power.
Data from the 1970 British Cohort Study allow us to examine the link between mental ability at the age of 10 years and risk factors reported by study participants at the age of 30 years and, in so doing, address these issues of data paucity and methodological shortcomings. A priori, we chose to examine the predictive value of mental ability scores at 10 years of age because it is around this period that ability begins to stabilise.22 That data on mental ability were also collected when the study members were aged five years affords us the opportunity of exploring the link between these early life scores and adult risk factors.
METHODS
The 1970 British Cohort Study is an ongoing longitudinal study that takes as its subjects 17 198 live births occurring to parents residing in Great Britain between 5 and 11 April 1970.23 Following the initial 1970 survey, there have been five major follow-up studies of the cohort members to monitor their physical, educational and social development, their transitions to adult life24 and, in the latest study, their adult identity. The present analyses uses data from 1980–1981 when study participants completed cognitive ability tests at the age of 10 years,25 and from 1999–2000 when, aged 30 years, they responded to enquiries about their health, including risk factors for premature mortality.26
Mental ability score at the five-year follow-up
Written informed consent was given by parents of study participants before the start of data collection. Testing of the children’s mental ability took place in the children’s homes. Four tests were used: the Human Figure Drawing Test, a Copying Designs Test, the English Picture Vocabulary Test and the Profile Test. The Human Figure Drawing Test was a modified version of the Draw-a-Man Test, originally devised in the 1920s by Goodenough27 and developed by Harris28 as a measure of intellectual maturity. Scores on the test correlate with conventional IQ tests (approximately r = 0.5).29 Children were asked to “make a picture of a man or lady”, and to draw a whole person. When they had finished, they were asked what the drawing was, what various parts of the drawing were and to label them. They were then requested to draw another picture of the opposite sex depicted in the first drawing, and the same process was repeated. The drawings produced by the children were scored using an adapted version of the Harris–Goodenough scale, based on 30 developmental items.30 The Copying Designs Test is measure of visual–motor coordination.31 Children were asked to make two copies of eight designs. The English Picture Vocabulary Test is an adaptation of the American Peabody Picture Vocabulary Test.32 It consists of a series of 56 sets of four different pictures with a particular word associated with each set of four pictures. The children were asked to point out the one picture that corresponds to the given word. In the Profile Test, children were shown an incomplete profile of a head, asked what it was, and then requested to complete the drawing and to identify and label the various parts. Scores from these tests were recorded by trained coders. The reliability of coding was checked on a random sample of 273 tests and showed that the percentage of tests in which the original code was not confirmed on recoding was only 1% or less for each test.
We carried out a principal components analysis of these four tests in order to establish the presence of a general cognitive ability factor (denoted as g). Examination of the scree slope suggested the presence of a single component. The first unrotated principal components accounted for 45% of the total variance among the four tests. The factor loading of each of the tests on the first unrotated principal component was 0.71 for the Human Figure Drawing Test, 0.75 for the Copying Designs, 0.63 for the English Picture Vocabulary Test and 0.55 for the Profile Test. Scores were saved for each subject on the first unrotated principal component, which is an indicator of each person’s general cognitive ability.33
Data collected at the 10-year follow-up
Testing of the children’s mental ability took place in schools. Mental ability at the age of 10 years was assessed using a modified version of the British Ability Scales,34 the administration of which was adapted so that it could be carried out by teachers. There were four subscales: word definitions, word similarities, recall of digits, and matrices. The word definitions subscale consisted of a list of 37 words. The teacher articulated each word in turn and asked the child about its meaning. The word similarities subscale consisted of 42 items each made up of three words (for example, orange, banana, strawberry or sad, worried, happy). For each item, the teacher enunciated the three words and asked the child to name another word consistent with the theme. The recall of digits subscale consisted of 34 items. For each item, the teacher read out digits at half-second intervals and asked the child to repeat them. The matrices subscale consisted of 28 incomplete patterns arrayed as a grid. For each item, the child was requested to draw in the missing part of the pattern. Test results were scored by trained coders. The reliability of coding was monitored throughout the survey and results were fed back to the coders. Regular checks carried out on a 5% random sample of tests showed that the percentage of tests in which the original code was not confirmed on recoding was low: 0.8% for recall of digits, 4.7% for word definitions, 1.9% for word similarities and 2.3% for matrices.35
Following principal component analyses of these four tests, examination of the scree slope suggested the presence of a single component. The first unrotated principal component accounted for 57% of the total variance among the four tests. The factor loading of each of the tests on the first unrotated principal component was 0.83 for word definitions, 0.84 for word similarities, 0.58 for digit recall, and 0.74 for matrices. Again, scores were saved for each subject on the first unrotated principal component.33 For ease of interpretation, we transformed the g score from the tests at five and 10 years of age to an IQ-type score (mean 100, SD 15). Finally, in order to explore whether any aspects of performance on the cognitive tests had an influence on the risk factor outcomes once the effect of general cognitive ability was subtracted, we saved the residuals from linear regression analyses of each test on the IQ score.
Information on the current occupation of both parents was collected during the interview with the child’s parents in 1980. The social class of each parent was derived from their current occupation using four categories (professional/managerial; skilled non-manual; skilled manual; semiskilled or unskilled) according to the 1980 Registrar General’s Classification of Occupations.36 The children underwent a medical examination during which evidence of illness or handicap was recorded, and blood pressure, height and weight were measured. We calculated body mass index (BMI; kg/m2) from the height and weight data, converting to metric units as necessary. Data on birth weight were ascertained from medical records.
Data collected at the 30-year follow-up
Information was collected by interview in the participant’s home, with participants giving written consent. As part of a series of questions on health, study members were asked about their current smoking status and smoking history, their height (without shoes), their weight (without clothes, and before pregnancy when relevant), and whether they had ever had high blood pressure or diabetes. There is evidence that self-reports of each of these indices show moderate to high levels of agreement with data extracted from medical records or biochemical indicators, making them acceptable for use in large-scale population-based studies.37–40 Furthermore, as we demonstrate later (see Results section), individuals who reported high blood pressure at the age of 30 years were more likely to have higher directly measured values at ages 10 and 16 years. We calculated BMI from the height and weight data, converting to metric units as necessary. We defined overweight (⩾25 kg/m2) and obesity (⩾30.0 kg/m2) according to World Health Organisation criteria.41 Participants were asked about their highest academic or vocational qualification and these were subsequently coded into six categories (no qualifications; certificate of secondary education grades 2–5/national vocational qualification (NVQ) level 1 and equivalent qualifications; ordinary levels/NVQ level 2 and equivalent qualifications; advanced levels/NVQ level 3 and equivalent qualifications; degree or diploma/NVQ level 4 and equivalent qualifications; or higher degree/NVQ level 5). The subject’s social class was derived from their own current occupation using the same four categories described above. Enquiries were made regarding participants’ current gross and net (take-home) pay from employment and what period this amount covered. Annual equivalent last gross pay was derived from these data. When gross pay was missing but net pay variables were available, gross pay was imputed from net using known parameters of the tax system in the relevant year.26
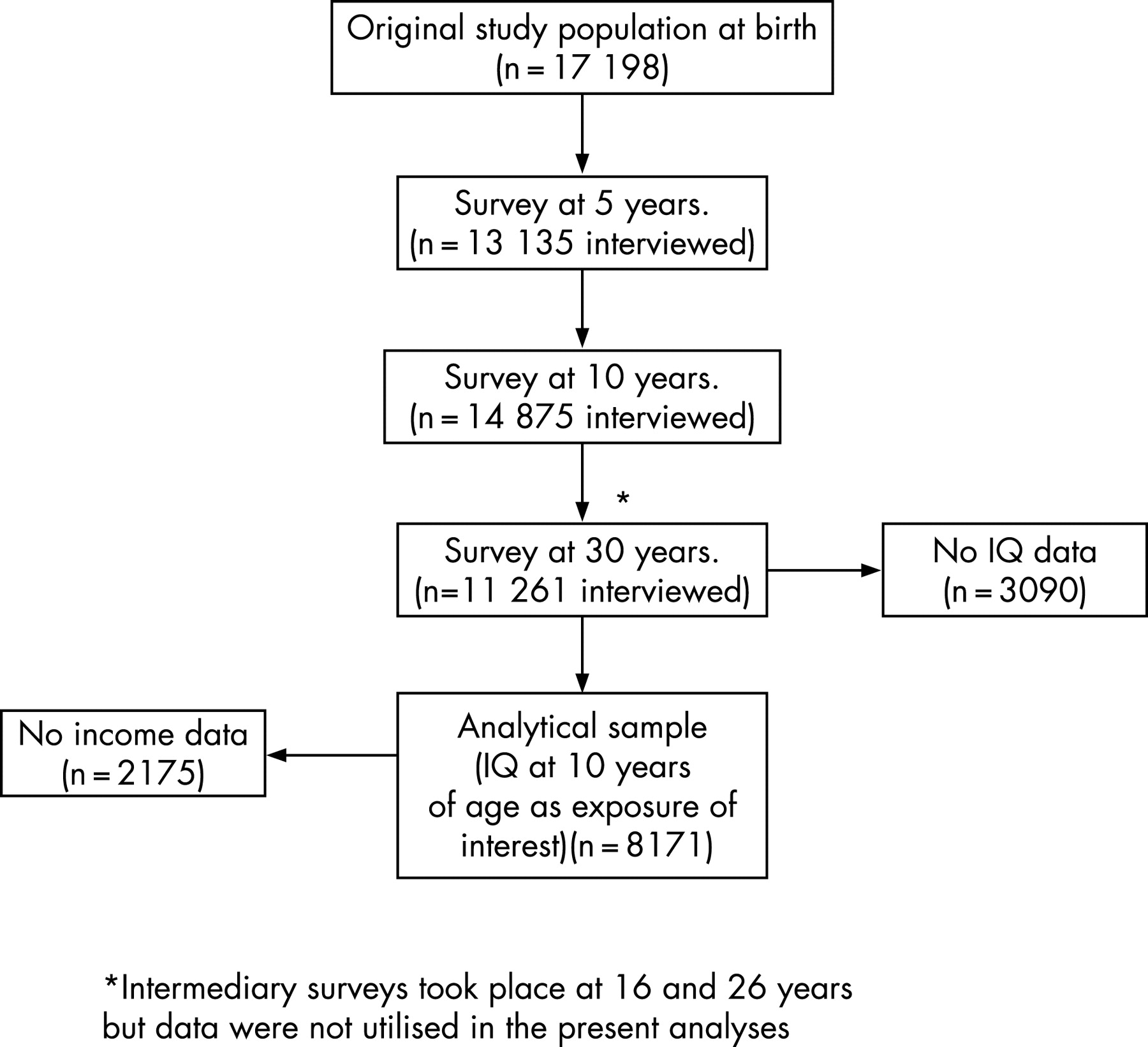
The number of participants in 1970 British Cohort Study at each phase of data collection is illustrated in fig 1. In total, 8171 study members (72.5%) had data on cognitive function at the age of 10 years and 8203 (72.8%) had cognitive function data at the age of five years. As discussed, the analyses that follow are based primarily on the former group.
{kind=link}
Compared with these 8171 men and women, cohort members who did not participate in the 30-year follow-up had a slightly lower general ability or g score at the age of 10 years (mean (SD) IQ score was 97.1 (15.3) compared with 101.1 (14.7); p value for difference <0.001). Similar results were apparent for IQ at five years of age. Those who did not participate at the 30-year follow-up were also slightly more likely to have come from a manual social class background at the age of 10 years than those who did participate (56.3% compared with 52.5%). Some cohort members were missing data on father’s social class at the age of 10 years or current social class at the age of 30 years. Comparison of cohort members with and without complete data for these potential confounding or mediating variables showed that the relations between IQ score and the adult self-reported risk factor outcomes were similar in the two groups. To avoid selection bias, we retained cohort members with incomplete data in the analysis by using mother’s social class in place of father’s social class if no father was present and by creating an extra category for missing data within childhood and current social class.
Statistical analysis
We used analysis of variance to examine the relations between the mean IQ score and the characteristics of the participants. Correlation coefficients were used to examine the relation between IQ score and educational qualifications. We used logistic regression to test whether IQ score at the age of 10 years was associated with the following binary outcomes (yes/no): smoking either currently or in the past, giving up smoking (among those who had ever smoked), and the presence of obesity, overweight, self-reported high blood pressure and self-reported diabetes. Odds ratios with accompanying 95% confidence intervals were expressed per 1 SD increase in the IQ score. In preliminary analyses, there was no suggestion that sex modified the IQ score–risk factor relationship, so all effects estimates are individually adjusted for sex, in addition to childhood social class at the age of 10 years, own occupational social class, highest academic or vocational qualification, and annual earnings at the age of 30 years.
RESULTS
Table 1 shows the characteristics of the study participants in relation to IQ score at the age of 10 years. As expected, IQ score was strongly associated with socioeconomic circumstances across the life course. Those individuals who were from, or were currently themselves in, a non-manual occupation thus had markedly higher childhood IQ scores than their counterparts in manual employment. There was also a strong relationship between ability and academic or vocational qualifications achieved by the age of 30 years, with markedly greater IQ scores at 10 years of age apparent in individuals with higher attainment. Data on current annual earnings were available for 5996 of the participants (74%). Annual earnings at the age of 30 years was also positively related to IQ score at the age of 10 years. Males had a slightly higher average IQ score than females.
Most of the risk factors for premature mortality were strongly associated with socioeconomic circumstances (data not shown). Smoking, overweight, obesity, and self-reported high blood pressure were thus less common among participants from higher social classes (early life and current), among those who had higher educational qualifications and among those with greater annual earnings. Diabetes was the only risk factor that showed no associations with any indicator of socioeconomic circumstances, but the number of cases was low (n = 82). Women were less likely than men to smoke, or to be overweight, but they were more likely to report a history of high blood pressure, and were more likely to have given up smoking by the time of the 30-year follow-up (data not shown).
Table 2 shows the prevalence of each of the risk factors at the 30-year follow-up and their relation to the childhood IQ score at the age of 10 years, adjusting for sex and socioeconomic circumstances across the life course. In sex-controlled analyses a 1 SD rise in the childhood IQ score was associated with reductions of 16% in the likelihood of being a current smoker (odds ratioper 1 SD advantage in IQ (OR) 0.84; 95% CI 0.80, 0.88), 16% in the likelihood of being obese (OR 0.84; 95% CI 0.79, 0.91), and 10% in the likelihood of having high blood pressure (OR 0.90; 95% CI 0.83, 0.98). The childhood IQ score was positively associated with an increase of 25% in the “risk” of having given up smoking (OR 1.25; 95% CI 1.18, 1.24) by the age of 30 years. There was no apparent IQ–diabetes association in these analyses. Controlling for early life socioeconomic position led to some attenuation of these IQ–risk factor relationships, although they remained statistically significant at conventional levels. Whereas attenuation was also apparent when we adjusted separately for current occupational social class, all relations with IQ, except for ever smoking, were retained. Adjusting for educational qualifications had the strongest impact of any covariate in the present analyses, with the association between IQ and ever smoking actually reversed. Control for current earnings had only a modest effect on the relations between the childhood IQ score and adult risk factors. In multivariate models in which we adjusted for all indicators of socioeconomic circumstances (childhood and currently), higher IQ score at the age of 10 years ceased to be a predictor of giving up smoking by the age of 30 years, but it continued to be associated with a reduced likelihood of being overweight. A very similar pattern of association to that reported above was also seen in the analyses in which IQ at five years of age was the principal exposure of interest (table 3).
Study participants who were overweight at the age of 30 years tended to have greater adiposity at the age of 10 years than the rest of the participants; mean BMI at the age of 10 years was 17.6 compared with 16.3 kg/m2 (p<0.001). They were also more likely to have had evidence of illness or handicap on medical examination aged 10 years (OR 1.25; 95% CI 1.01, 1.25). Although overweight individuals were also marginally heavier at birth (3.35 kg compared with 3.29 kg), this differential was small, only attaining statistical significance (p<0.001) as a result of the large sample size. We examined whether the relation between lower childhood IQ score and an increased risk of being overweight as an adult was affected by adjusting for each of these indices. These adjustments strengthened the association; in multivariate analysis in which we controlled for the aforementioned factors plus all indicators of socioeconomic circumstances already listed, a 1 SD increase in the childhood IQ score was associated with a reduction of 11% in the risk of being overweight as an adult (OR 0.89; 95% CI 0.84, 0.95).
Individuals who reported having high blood pressure at the age of 30 years had higher directly measured blood pressure at the age of 10 years (mean for systolic 101.7 versus 97.8 mm Hg) and at the age of 16 years (115.7 versus 110.8 mm Hg). They also had a very slightly lower birth weight (3.28 versus 3.31 kg, p = 0.06), although the difference was not statistically significant. The inclusion of systolic blood pressure at the age of 10 years and birth weight in the sex-adjusted model had little effect on the relation between childhood IQ score and the risk of high blood pressure as an adult (OR 0.91; 95% CI 0.83, 0.99), although the relation was attenuated when adjusted for childhood and adult socioeconomic circumstances (OR 0.98; 95% CI 0.86, 1.11).
In the analyses described above (table 2), we assessed the relation between adult risk factors for premature mortality and childhood general mental ability, which we extracted from a principal components analysis of scores on four tests of ability at the age of 10 years (matrices, digit recall, word definitions and word similarities). In order to explore whether any aspects of childhood performance on the cognitive function tests were associated with these adult risk factors when the effect of general ability was subtracted, as indicated, we saved the residuals from linear regression analyses of each test on IQ score and examined the relation of each of them separately with the risk factors. Participants who scored higher on the matrices test than would be expected from their IQ score were less likely to be a current smoker (OR 0.93; 95% CI 0.89, 0.99 in sex-adjusted analyses), but this relation was attenuated after multivariate adjustment. We found no other significant associations, suggesting that it is childhood general ability rather than any other specific aspect of cognitive function that predicts these outcomes in adult life. That is, the associations between the ability scores and the risk factors were essentially due to general cognitive ability alone.
DISCUSSION
The aim of the present analyses was to explore the relation between childhood IQ at 10 years of age and established adult risk factors for premature mortality as potential mechanisms linking IQ with mortality. In univariate analyses, higher childhood IQ scores were related to a lower risk at the age of 30 years of ever having smoked (and an increased likelihood of having given up once started), being overweight or obese, and having raised blood pressure. Although our primary motivation for examining the link between IQ and established risk factors for mortality was to explore potential pathways linking IQ with death, it is also the case that some of the risk factors studied—hypertension, obesity—are important health endpoints in their own right.
What this paper adds
In this, the largest study to date to examine the relationship between IQ across childhood and a range of behavioural and physiological risk factors for premature mortality, higher test scores were associated with more favourable levels of some indices in middle age.
This is the first study to demonstrate that IQ scores as early as five years of age predict these adult health outcomes.
Most of the IQ–risk factor associations were somewhat weakened after statistical control for indicators of socioeconomic position, particularly in adulthood. Education had the most consistent and strongest attenuating effect. It is plausible that educational attainment may represent at least a partial proxy for IQ42 43 and in cognitive domains not examined in the mental ability tests taken by our participants. As such, including it in our statistical models may be seen as over-adjustment; in the present study, and elsewhere,44 education and mental ability were correlated (rs = 0.43, p<0.001). Educational attainment, like IQ, is related to several of the health outcomes featured in the present analyses.45
In a related point, in the main analyses of the present study, childhood mental ability was measured at 10 years of age, after five years of exposure to the education system. It is therefore possible that the quality of early educational experience, via any effect it has on IQ scores, contributes to disease risk. Mental ability assessed as early as five years of age was, however, related to cognitive performance at the age of 10 years (r = 0.50; p value <0.001). Furthermore, it is striking that when we examined the predictive value of IQ score at the age of five years for the various risk factor outcomes, the relations revealed were essentially the same as those when IQ five years later was the main exposure. To our knowledge, this is the earliest in life that IQ scores have been shown to be related to adult health endpoints.
Comparison with other studies
As described, to date there is a dearth of studies examining the association between childhood mental ability and adult risk factors for premature mortality. Hypertension is not only a risk factor for mortality but also a health outcome its own right. Childhood mental ability scores have been found to be lower in middle and older-age adults with hypertension (classified from direct measurement) in comparison with their disease-free counterparts.15 46 In a Scottish group, there was a weak correlation between the full range of individual blood pressure and IQ scores.46 In the present study raised blood pressure was self-reported at the age of 30 years, rather than in older age, and, although there was a reduced prevalence in people with higher childhood IQ, this relation was lost at conventional levels of statistical significance when educational qualifications entered the multivariable model. In a separate middle-aged population, childhood mental ability and self-reported high blood pressure were not associated.14
Policy implications
The skills captured by IQ tests, such as verbal comprehension and reasoning, may be important in the successful management of an individual’s health behaviours and associated outcomes.
Several previous studies, largely sampling men, have reported on the association between early life mental ability and obesity/overweight.16–21 Findings are mixed, with null and inverse relations seen. We are aware of only two20 21 reports of the link between childhood IQ and adult obesity/overweight, but only one of these21 adjusted for potential mediating or confounding factors as we did. In the 1958 British Birth Cohort,21 the null association reported after adjustment for a wide range of covariates contrasts with the inverse effect we found. Several of the studies reporting a lower risk of obesity/overweight in the higher mental ability groups are cross-sectional17 47 or case–control studies.17–19 This raises concerns about reverse causality. That is, rather than low cognition scores predicting obesity/overweight, it may be that the development of these conditions, with their accompanying social stigma, leads to a failure to thrive cognitively.16 18 Longitudinal studies are well placed to explore this issue by either excluding individuals with existing obesity/overweight at study induction so that the occurrence of obesity/overweight can be studied, or by controlling for early life obesity status. In the present analyses, the apparent protection conferred by high early life mental tests scores against later obesity/overweight actually increased when we adjusted for childhood BMI.
Smoking initiation was unrelated to IQ in one study,1 whereas three others14 48 49 found an inverse association, as we did; however, one of these reports did not provide effect estimates.49 That another utilised a survey sample drawn from a group of individuals classified as “unwanted” at birth who were then followed into later life48 suggests that the findings have somewhat questionable generalisability. In the present cohort we have also shown that IQ at the age of 10 years is related to other behaviours in later life, in particular physical activity, food intake and vegetarianism.50 51
Strengths and limitations
The present study has some advantages over existing work. First, the analytical sample is an order of magnitude larger in size than most other studies examining the link between IQ and risk factors for mortality in later life, so providing high statistical power. Second, by reporting on the relation of ability with a range of risk factors we have been able to examine the specificity of association. Third, the present cohort is particularly well characterised for life course socioeconomic position, and also includes data on birth weight, childhood obesity and illness, so allowing us to examine the independent effect of childhood IQ. Fourth, whereas most studies use single mental tests or sums of test scores, we employed a validated psychometric approach that examined the effect of the general cognitive factor and non-g residual components. Finally, with the data drawn from participants who reside throughout Great Britain, our findings should have a high degree of generalisability.
Inevitably, there are also some study limitations. First, although we were able to examine the relation of mental ability with important risk factors for premature mortality, all outcomes were self-reported and no data were available on blood cholesterol and emerging or novel risk indices such as markers of blood clotting, inflammation, and thrombosis.52 Second, the longitudinal nature of the present study has inevitably led to some attrition; only 46% of the participants at the 30-year follow-up had taken part in all earlier surveys of the cohort, although 80% of the participants in the 30-year follow-up had missed none or only one of these earlier sweeps, and 74% of them had taken the British Ability Scale tests as part of the 10-year follow-up.53 The participants at the 30-year follow-up did gain significantly higher scores at the age of 10 years for mental ability than those who did not take part, an observation made elsewhere,54 but the size of the differences was very modest (0.3 SD). Unless the relations of childhood mental ability with risk factors for premature mortality are in the opposite direction in non-responders or those who have died to those found in the present analyses—a highly unlikely scenario—little bias will have been introduced.
Third, by relating childhood IQ to adult risk factors for premature mortality we have attempted to assess their potential mediating role in the apparent association between pre-morbid IQ and premature mortality. To test such pathways fully, however, a data set with information on childhood IQ, adult risk factors and mortality would be required. We are aware of one study that holds such data. In the 1946 British birth cohort, an inverse IQ–mortality relationship was evident in men but not women55 although the number of deaths was low. Adjusting for adult smoking patterns at the age of 26 years had little impact on this association among men. One explanation might be that smoking habits at 26 years of age are not indicative of later behaviour that influences disease risk; another is that smoking does not lie on the mechanistic pathway linking early life IQ with adult mortality risk. Further studies are clearly needed.
Public health implications
At least two potential interventions could be utilised to address the apparent cognitive variation in health outcomes identified in the present study. First, in a far-reaching approach, early life educational programmes could be utilised to enhance childhood mental ability. Two recent reviews of early learning and school readiness interventions,56 57 one of which focused on randomised trials only,56 found that these programmes resulted in marked improvements on tests of reading, arithmetic ability and general intelligence that appeared to extend to secondary school ages. Critically, however, the extent to which these improvements are actually maintained across the life span has yet to be examined. Second, the skills measured using mental ability tests, which include reasoning and verbal comprehension, may be of relevance in the successful management of related health behaviours. Behavioural modification advice, intended, for example, to modify levels of smoking, physical activity and diet—for the latter it can be particularly complex—could therefore be redesigned to make it more suitable for individuals with lower cognitive ability. In principal, this would be a rapidly implemented, adult-targeted intervention to address cognitive variation in these behaviours.
In conclusion, in the present study, childhood IQ was associated with risk factors for premature mortality, such that a raised prevalence of some risk indicators was evident in lower IQ-scoring individuals. By establishing associations between general cognitive ability and risk factors for mortality, these relationships begin to offer some insights into the mechanisms underlying the gradient between low pre-adult mental ability and premature mortality.
CONTRIBUTIONS
G D B generated the idea for the present analyses, which was developed by C R G and I J D. C R G conducted all data analyses. I J D advised on the psychometric analyses of the mental ability tests. C R G and G D B wrote the first draft of the manuscript. All co-authors made substantial contributions to subsequent drafts.
Acknowledgments
The 10-year follow-up was carried out by the Department of Child Health, Bristol University. The 30-year follow-up was carried out under the auspices of the Joint Centre for Longitudinal Research (comprising the Centre for Longitudinal Studies, Institute of Education, University of London, the International Centre for Health and Society, University College Medical School, London, and the National Centre for Social Research). The authors would like to thank the UK Data Archive, University of Essex, for providing the data. D B is a Wellcome Fellow. The original data creators, depositors or copyright holders, the funding agencies, and the UK Data Archive bear no responsibility for the analyses and interpretation presented here.
We thank Doug Carroll and two other anonymous referees for their constructive comments.
REFERENCES
Footnotes
Funding: I S is funded by UK ESRC grants L326253061, RES-225-25-2001, and RES-000-22-1748. I J D is the recipient of a Royal Society–Wolfson Research Merit Award. GB is a Wellcome Trust Fellow.
Competing interests: None declared.
- Abbreviations:
- NVQ
- national vocational qualification
Linked Articles
- In this issue