Article Text

Abstract
Objectives: To examine whether, in former communist countries that have undergone profound social and economic transformation, health status is associated with income inequality and other societal characteristics, and whether this represents something more than the association of health status with individual socioeconomic circumstances.
Design: Multilevel analysis of cross-sectional data.
Setting: 13 Countries from Central and Eastern Europe and the former Soviet Union.
Participants: Population samples aged 18+ years (a total of 15 331 respondents).
Mean outcome measures: Poor self-rated health.
Results: There were marked differences among participating countries in rates of poor health (a greater than twofold difference between the countries with the highest and lowest rates of poor health), gross domestic product per capita adjusted for purchasing power parity (a greater than threefold difference), the Gini coefficient of income inequality (twofold difference), corruption index (twofold difference) and homicide rates (20-fold difference). Ecologically, the age- and sex-standardised prevalence of poor self-rated health correlated strongly with life expectancy at age 15 (r = −0.73). In multilevel analyses, societal (country-level) measures of income inequality were not associated with poor health. Corruption and gross domestic product per capita were associated with poor health after controlling for individuals’ socioeconomic circumstances (education, household income, marital status and ownership of household items); the odds ratios were 1.15 (95% confidence interval 1.03 to 1.29) per 1 unit (on a 10-point scale) increase in the corruption index and 0.79 (95% confidence interval 0.68 to 0.93) per $5000 increase in gross domestic product per capita. The effects of gross domestic product and corruption were virtually identical in people whose household income was below and above the median.
Conclusion: Societal measures of prosperity and corruption, but not income inequalities, were associated with health independently of individual-level socioeconomic characteristics. The finding that these effects were similar in persons with lower and higher income suggests that these factors do not operate exclusively through poverty.
- Eastern Europe
- socioeconomic factors
- income inequality
- societal factors
- multilevel analysis
Statistics from Altmetric.com
There is extensive literature documenting the influence of social and psychosocial factors on health.1 The effects of individual-level factors, such as education and perceived level of control, have been well documented in a large number of studies. More recently, it has been shown that, in developed countries, societal characteristics, such as income inequality, are also associated with various measures of health status.1–4 It has been proposed that high income inequality is an indicator of low levels of social capital or social cohesion;5 6 these are inherently ecological concepts that cannot be measured at the level of individuals.5 Societies that are more egalitarian and have higher levels of social capital and social cohesion tend to be more healthy,7–10 but there is a vigorous debate as to whether the effects of societal characteristics are independent of other aggregate or individual socioeconomic measures.7 11 12
The issue of the effects of societal characteristics on health is particularly pertinent to the countries of Central and Eastern Europe (CEE) and the former Soviet Union (FSU). Since the 1960s, both health status and economic indicators in CEE/FSU have been lagging behind those in Western Europe and North America.13 Moreover, superimposed on these long-term trends were dramatic political, social and economic changes following the fall of the communist regimes that occurred in the region in 1989/1990. Over a short period of time, economic production, real wages and gross domestic product (GDP) fell substantially, while unemployment, crime and income inequalities rose steeply.14–16 For example, between 1989 and 1996 income inequalities in Russia increased from very low levels to levels seen in Latin America.15 At the same time, there were dramatic fluctuations in mortality, particularly in the countries of the FSU. For example, between 1989 and 1994, mortality from all causes in Russia increased by 45% in men and by 27% in women, and Russian mortality rates were still rising in 2004 (WHO Health for All database).
At the national level, changes in life expectancy in CEE/FSU during the societal transformation were associated with macroeconomic changes: the fall in life expectancy was most pronounced in countries with the largest fall in GDP and the largest rise in income inequality.17 These international data are consistent with ecological studies in several CEE/FSU countries, which found that markers of “social stress”, low social cohesion or low social capital were associated with increased mortality.18–21 None of these studies, however, took into account individual socioeconomic status (SES). It is possible that the apparent effect of societal factors reflects no more than the well-established effect on health of individuals’ socioeconomic characteristics. To our knowledge, only one study that combined societal and individual-level data has been conducted in CEE/FSU to date. In that study, income inequality was associated with increased rates of poor self-reported health, but the association was removed by adjustment for individual SES and, separately, by adjustment for low perceived control.22
Our study had two objectives: first, to determine whether there is a relation between health status and societal characteristics, including income inequality; and, second, if such a relation were found, to investigate whether it is independent of individuals’ socioeconomic status and markers of societal wealth.
Although mortality or another objective health outcome would be preferable, it would require either linkages of mortality registers with good routinely collected data on socioeconomic characteristics or longitudinal follow-up of large population samples in many countries. Neither is currently possible or feasible. Self-rated health, on the other hand, is easy to measure in population surveys, is a good predictor of future mortality in individuals,23 and correlates well with mortality at the aggregate level.22 24 We therefore used self-rated health as the primary outcome in this study.
The selection of societal characteristics as potential predictors of health was based on the availability of data and previous research. Since there is a large body literature on income inequality, we used the Gini coefficient and two measures of income inequality derived from the survey data.
We also used national homicide rates, since they indicate levels of crime, considered by some as an indicator of social capital.20 25–27 Corruption is a societal indicator of adherence to legal norms in public offices and institutions, and has been linked to governance28 and social capital.29 30 Finally, we included several markers of economic prosperity, since this is seen as the most likely potential confounder of the relationship between income inequality and health.
METHODS
Study populations
The data come from the 2004 round of the New Europe Barometer surveys, a series of population surveys in the former communist countries with primary focus on political and social attitudes (www.abdn.ac.uk/cspp). The characteristics of 13 countries surveyed in 2004 and of the study samples are shown in tables 1 and 2. In each country, a random sample of the population aged 18 years and over was selected by a multistage sampling method. The response rates ranged between 59% and 67%; refusal rates were between 16% and 25%; the remaining non-responders comprised those who were not at home on three separate occasions. Sampling and interviews were conducted by local agencies. Since the studies focused on political and social attitudes, ethics approval was not required.
Data were collected by structured questionnaires completed during interviews in subjects’ homes. In all centres, the questionnaires contained identical questions on the variables of interest, and correct wording was checked by translating questions back into English.
Self-rated health
In all countries, subjects were asked an identical question: “How do you rate your physical health in the last 12 months?” The possible responses were very good, good, average, bad and very bad. The variable was dichotomised by combining the responses into “poor health” (bad and very bad responses) and “good health” (very good, good and average responses).
Individual socioeconomic factors
Several socioeconomic characteristics were available in all countries. First, participants reported their education on a locally appropriate scale; these responses were then reclassified into three categories: less than secondary, secondary and higher than secondary education. Second, participants also reported monthly household income in local currency, either as an exact value or in bands; we used country-specific quartiles in these analyses. Third, participants reported whether their household owned a colour television, video recorder or car, and if they had access to the Internet. We used the number of the items owned as a categorical variable. Fourth, the subjects reported their marital status (married/cohabiting, single, separated/divorced or widowed).
Societal characteristics
Because of our a priori interest in income inequalities and other societal variables, and on the basis of the ecological correlations, the following societal (i.e. country-level) characteristics were included in the multilevel models: income inequality, corruption index and homicide rate. We also analysed the effects of GDP, the maximum economic contraction between 1990 and 2004 and the annual economic growth between 1990 and 2004.
Most societal indicators were taken from external sources. Recent estimates of GDP adjusted for purchasing power parity (PPP) in 2004, annual economic growth and the maximal contraction of the economy (i.e. the number of percentage points by which GDP fell) between 1990 and 2004, and the Gini coefficient of income inequality in 2004 were obtained from the TransMONEE database.31 The Corruption Perception Index, based on expert rating and published by Transparency International, ranks countries in terms of the degree to which corruption is perceived to exist among public officials and politicians (www.transparency.org). For each country, the index estimates levels of corruption on a scale from 0 to 10; for the analyses, we recoded the original values so that 0 indicates the lowest level of corruption and 10 indicates the highest level. National rates of homicide and life expectancy at birth and at age 15 (to compare rates of self-rated health with objective outcomes) were taken from the WHO Health for All database (www.who.dk/hfadb).
In addition, since income inequality was one of our primary interests, we also used the survey data to obtain alternative estimates of income inequalities that are independent of the official data. To do so, we plotted for each country separately the cumulative distribution of participants’ household income, from which we estimated the 10th, 20th, 80th and 90th percentiles. From these figures, we calculated the country-specific ratios of the 80th vs. 20th and 90th vs. 10th percentile. The larger the ratio, the more unequal the income distribution.
Statistical analyses
Two types of statistical analyses were conducted. First, we examined the ecological associations in the 13 countries between societal characteristics and life expectancy at age 15 and rates of poor self-rated health. For this purpose, we calculated national rates of poor health, directly standardised for age and sex from the survey data, using the total combined population in the 13 samples as standard population. Simple correlation coefficients were used.
Second, we combined the societal (ecological) variables with the individual-level data. We used logistic regression to estimate the effects of the societal factors on poor health after controlling for the individual characteristics. To take into account the clustering of individuals in countries (in effect, we had only 13 points of analysis of the societal factors), we used the robust estimates of the effects of societal characteristics (subcommand “cluster” in Stata 9). This approach is generally equivalent to a multilevel analysis with two levels (countries and individuals), with fixed individual-level effects. (We also fitted random effect models but they neither changed the results nor added to explanation of the effects of societal variables on health, and are therefore not reported.) For each societal characteristic, we built three statistical models: (1) adjusted for age and sex; (2) additionally adjusted for education, income quartile, number of household items owned and marital status; and (3) as in (2) plus GDP. Throughout the analyses, we checked for differences between men and women. As the results in men and women were similar (there was no statistically significant interaction between sex and societal characteristics), results are reported for both genders combined.
RESULTS
Participating countries
Characteristics of the 13 participating countries and study samples are shown in table 1. There was a greater than threefold difference in GDP between the poorest and richest countries and a twofold difference in the Gini coefficient between the most and least equal countries. The extent of the scale of the economic changes during the transformation is illustrated by economic contraction; in Ukraine, for example, the official economy at the time of the maximum contraction was only 40% of that in 1990. Differences in life expectancy at age 15 are also considerable; the difference between the country with the lowest and highest figures (Russia and Slovenia) is 10.4 years. The age- and sex-adjusted prevalence of poor self-rated health varied between 10.4% in Slovenia and 24.3% in Ukraine.
Population samples
Individual data were available on 15 331 persons, 55% of whom were women (table 2). About one-fifth of participants had higher than secondary education, and about three-fifths were married. On average, the participants’ household owned 2.1 out of the four possible items. The differences in the number of items between countries was in the expected direction; the ecological correlation between GDP and the number of items was 0.95 (p<0.001, not shown in tables).
Ecological associations
Self-rated health was the principal outcome variable for the main analyses. It was therefore of interest whether self-rated health correlates with life expectancy. There was a strong inverse association (figure 1): the higher the rate of poor health, the lower the life expectancy (r = −0.73, p = 0.005).

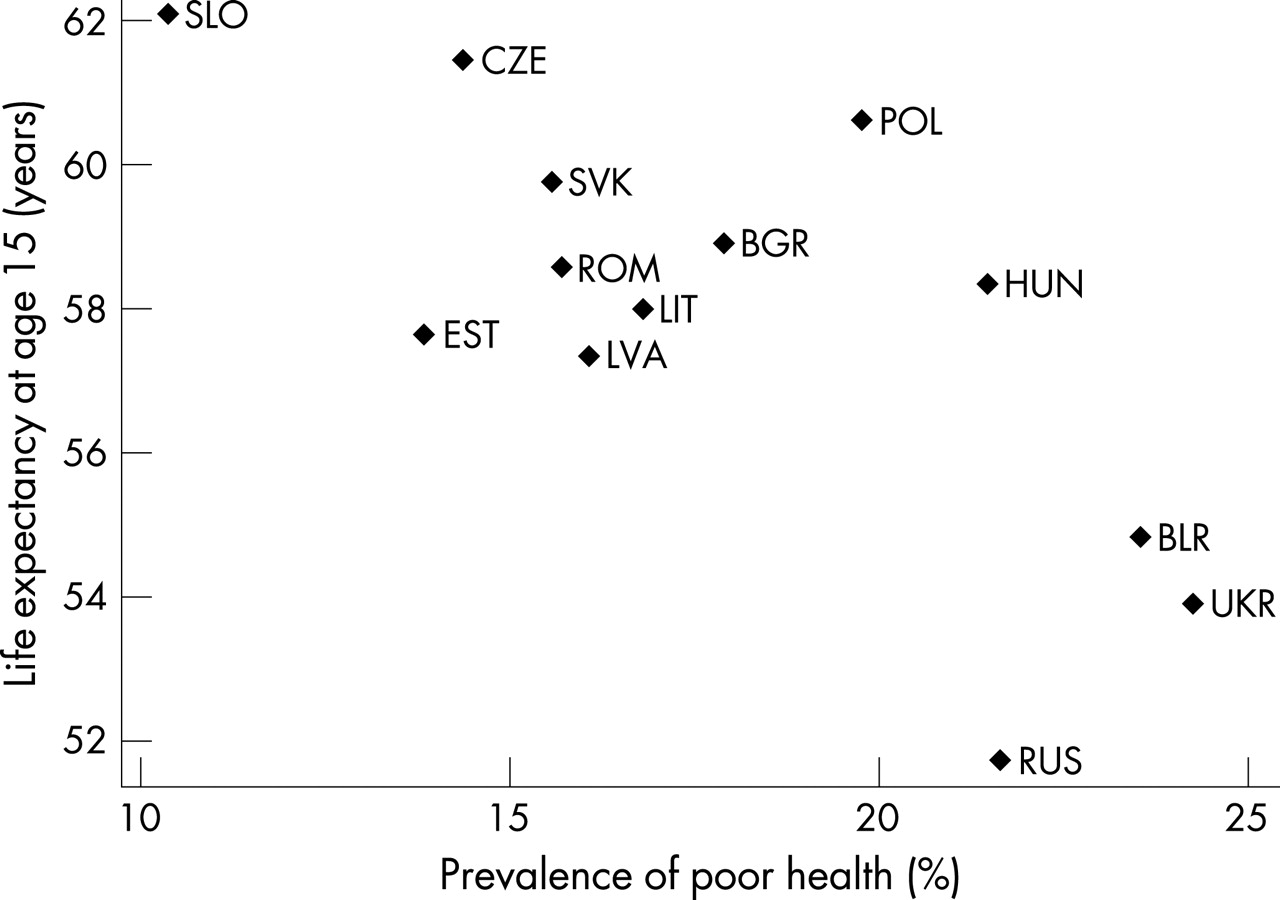{kind=link}
The correlation matrix for the societal characteristics, self-rated health and life expectancy is shown in table 3. Self-rated health was significantly correlated with GDP and corruption, and life expectancy at age 15 was related to all societal characteristics. The correlation between the national measure of income inequality, the Gini coefficient and the two data-derived measures was 0.71 for the ratio of 80th/20th percentile and 0.55 for the ratio of 90th/10th percentile.
Multilevel analyses
The results of analyses that combined societal and individual-level factors are shown in table 4. Our objective was to examine the association of society-level socioeconomic factors with health status and mortality, when additional variables are introduced. Neither the Gini coefficient nor the ratios of the 80th to the 20th or the 90th to the 10th income percentiles were significantly associated at the 0.05 level with poor self-rated health in age- and sex-adjusted models. Moreover, the estimated effects were further attenuated after additional adjustment for individual-level socioeconomic factors (table 4, model 2). Only corruption index and GDP among the eight societal characteristics were significantly associated with poor self-rated health in models that controlled for individual-level factors. Among these variables, GDP had the largest effect on health status, and further adjustment for GDP generally reduced the effect estimates in most cases (i.e. the coefficients moved nearer to 1.0) and none of the odds ratios was statistically significant (table 4, model 3). GDP was inversely associated with health status, and its effect remained significant in the five of the seven models that included GDP, individual factors and the other societal factor; the estimated odds ratio for a $5000 increase in GDP in these seven models ranged from 0.75 to 0.86 (results not shown, but available on request). Interactions between societal and individual-level variables were not statistically significant, and none improved the overall fit of the statistical models. We therefore concluded that, once individual-level variables were included, the additional explanatory power of these variables was reduced and, when the single macrolevel variable of GDP was introduced, none of the remaining societal variables retained significant explanatory power.
An alternative way of illustrating the role of deprivation compared with non-material influences is to stratify the samples by their household income. One would expect that the effects of societal characteristics that operate though deprivation would be stronger among poorer subjects. However, the odds ratios for GDP, corruption and homicide rate were almost identical in subjects with household income below and above the median, the three adjusted estimates being within 2% of each other (table 5), which confirms the previous points about the lack of interactions in these models.
DISCUSSION
In this multilevel analysis of population data from 13 former communist countries, measures of income inequality were not associated with rates of poor self-rated health. Corruption index and homicide rates were associated with poor health when individual socioeconomic factors were taken into account, but the associations were not statistically significant after additionally controlling for GDP. GDP was also positively associated with good health status, although this association also lost significance when controlled statistically for level of corruption.
We draw attention to a number of potential limitations that are not unique to this study. First, a more objective health outcome would be desirable, mainly because of the potential for reporting bias (less healthy persons may be more likely to spuriously over-report unfavourable social circumstances). However, such reporting bias is unlikely to be associated with societal characteristics that were taken from external sources, such as GDP, the Gini coefficient, the corruption index or homicide rate.
Second, measurement of macroeconomic indicators may be problematic in countries in transition, where a part of the economy is “shadow” economy. In this context, it is important that the officially estimated Gini coefficients correlated well with the inequality measures derived from the survey data (r = 0.71 and 0.55 for the ratios of 80th vs. 20th and 90th vs. 10th percentiles respectively). It is equally encouraging that official estimates of GDP agreed well with the number of items owned by the household (r = 0.95).
Third, more detailed data on individuals’ socioeconomic circumstances, were they available, may explain more of the effect of societal characteristics. This is particularly so with income; internationally comparable figures would be preferable to income in local currencies. However, calculating household income adjusted for purchasing power parity is not straightforward, especially since in seven countries household income was reported in bands. On the other hand, household item ownership correlated well with the absolute difference between countries and would probably capture at least some of the absolute differences in material conditions. One additional limitation is related to household income, namely that it was not adjusted for household size since data on household size were available in only six countries. However, it is unlikely that this problem affected the results of our study for three reasons. First, the differences in average household size between these six countries were negligible. Second, the results from analyses restricted to these six countries were virtually identical whether or not household size was included in the analysis. Third, official data show that the differences in household size among the 13 participating countries are small;32 thus, any influence on our results would also be small.
Finally, the analysis of societal effects is based on 13 countries only. Due to the collinearity between societal measures, it is difficult to reliably separate their effects. A larger number of countries would be needed to separate the effects of different societal characteristics.
Despite these limitations, our study also has a number of strengths. It is one of the largest multinational studies including data on both societal and individual characteristics. The variations in health and societal characteristics were much larger than among Western countries. This increases the chances of finding an effect, if it exists. Importantly, the national rates of poor health correlated remarkably well with life expectancy at age 15; this provides further support for self-rated health as a valid indicator of population health. Overall, the good correlation between official figures and estimates derived from the survey data also suggests that the samples were sufficiently representative for results to be generalisable to whole populations.
Despite the large variation in both health and income inequalities, neither measure of income inequality was associated with health status. The lack of an effect of income inequality is consistent with an earlier study in seven post-communist countries.22 One reason for the absence of an effect may be the type of study population. In the literature, a link between income inequality and health status seems to be restricted to wealthy countries, among which overall income (GDP) is no longer a predictor of mortality.2 While the former communist countries are not developing countries, most of them fall into the category of “middle-income” countries, rather than high-income countries, where most previous studies of income distribution have been conducted. It is possible that the effect of income inequality is not apparent in the presence of pronounced economic hardship, although, given the large variation in income inequality in these data, in countries which used to be egalitarian only 15 years ago, one would think that an effect of income inequality would be detected, if it existed. It is also possible, of course, that such an effect could have been missed due to the relatively low statistical power of the study.
There was, however, a relation between health and three societal characteristics: corruption index, homicide rate and GDP. The associations lost statistical significance after controlling for GDP but the interpretation of the last model is difficult – a multivariable analysis of just 13 points (countries) with mutually correlated variables is not statistically reliable. However, the associations of both corruption index and homicide rate with health status were in the expected direction, and they may reflect the effects on health of social institutions, governance and possibly social cohesion and social capital.25 26 28–30 This would be consistent with a number of ecological studies within countries both in CEE/FSU18–21 and elsewhere6 33
Throughout the analyses, GDP was consistently inversely associated with health status. This is not surprising given the grave economic problems of some of the participating countries. It is possible that, at least among the countries with low income, material deprivation is the most important social influence on health. On the other hand, adjustment for individual socioeconomic status led to only a modest reduction in the effect of GDP on health. This suggests that the role of GDP is not exclusively mediated by individual deprivation. In the ecological analyses, GDP correlated strongly with both corruption index and homicide rate. It is likely that, in addition to measuring societal wealth, GDP also reflects the quality of social organisation, which in turn also includes social cohesion.
As mentioned above, it is probably not possible to separate the effects of societal wealth from other societal characteristics in a study involving only 13 countries. However, one would expect that societal influences operating via material deprivation would be stronger in persons with low income. The fact that the effects on health of GDP, corruption and homicide rate were similar in persons below and above median household suggests that these effects do not operate exclusively through material deprivation.
It is plausible that the influence of GDP, corruption and crime reflect the presence and functioning of democratic institutions. A number of studies have suggested that democracy is positively associated with health status;34–36 the proposed mechanisms include representation (social and health policies are more a priority for groups who dominate in democracies), accountability (greater attention to social and health issues in democracies) and selection of political leaders (policies are formulated and supported by competent and less corrupt leaders).36 It also appears that the policy response to the social, economic and health crisis in CEE/FSU was more effective in countries with the better established democratic institutions (GA Cornia, 2006, unpublished).
In conclusion, these data confirm the close associations between health and GDP and other societal characteristics. The fact that the association between corruption and homicide rate and health is reduced after controlling statistically for GDP and, conversely, that of GDP to health is reduced when controlling for corruption does not make it straightforward to distinguish causal pathways, especially given the problem of collinearity. It is plausible, however, that the causal connection is from low GDP to lack of social cohesion and poorly functioning democratic institutions. Support for this theory is provided by the fact that the association between low GDP and poor health is as strong in people with higher than median income as in those with lower than median income. This study lends support to the view that social development in these countries, as in others where there have been market failures,37 will require the building of social institutions and well-functioning communities.
What is already known on this subject
At population level, health is associated with societal characteristics, such as income inequality, social capital and national prosperity. It is not clear, however, if this represents something more than the association of health with individual socioeconomic circumstances.
What this study adds
This is one of the largest multinational studies including data on both societal and individual characteristics. Societal measures of prosperity, crime and corruption, but not income inequality, seem to influence health independently of individual‐level socioeconomic characteristics. The finding that these effects were similar in people with lower and higher income suggests that these factors do not operate exclusively through poverty.
Policy implications
Reducing income inequality alone may not improve population health. However, the results support the view that social development in post-communist countries, as in others where there have been market failures, will require the building of social institutions and well-functioning communities.
Acknowledgments
All authors jointly designed the study. M Bobak analysed the data and drafted the paper. M Murphy advised on the statistical analyses and commented on the draft. R Rose and M Marmot commented on the draft.
REFERENCES
Footnotes
Funding: The study was funded by a grant from the Economic and Social Research Council and by the MacArthur Foundation Initiative on Social Upheaval and Health. The funding bodies had no influence over the design of the study and the analyses and interpretation of the data.
Competing interests: None
Linked Articles
- In this issue