Article Text

Statistics from Altmetric.com
Introduction
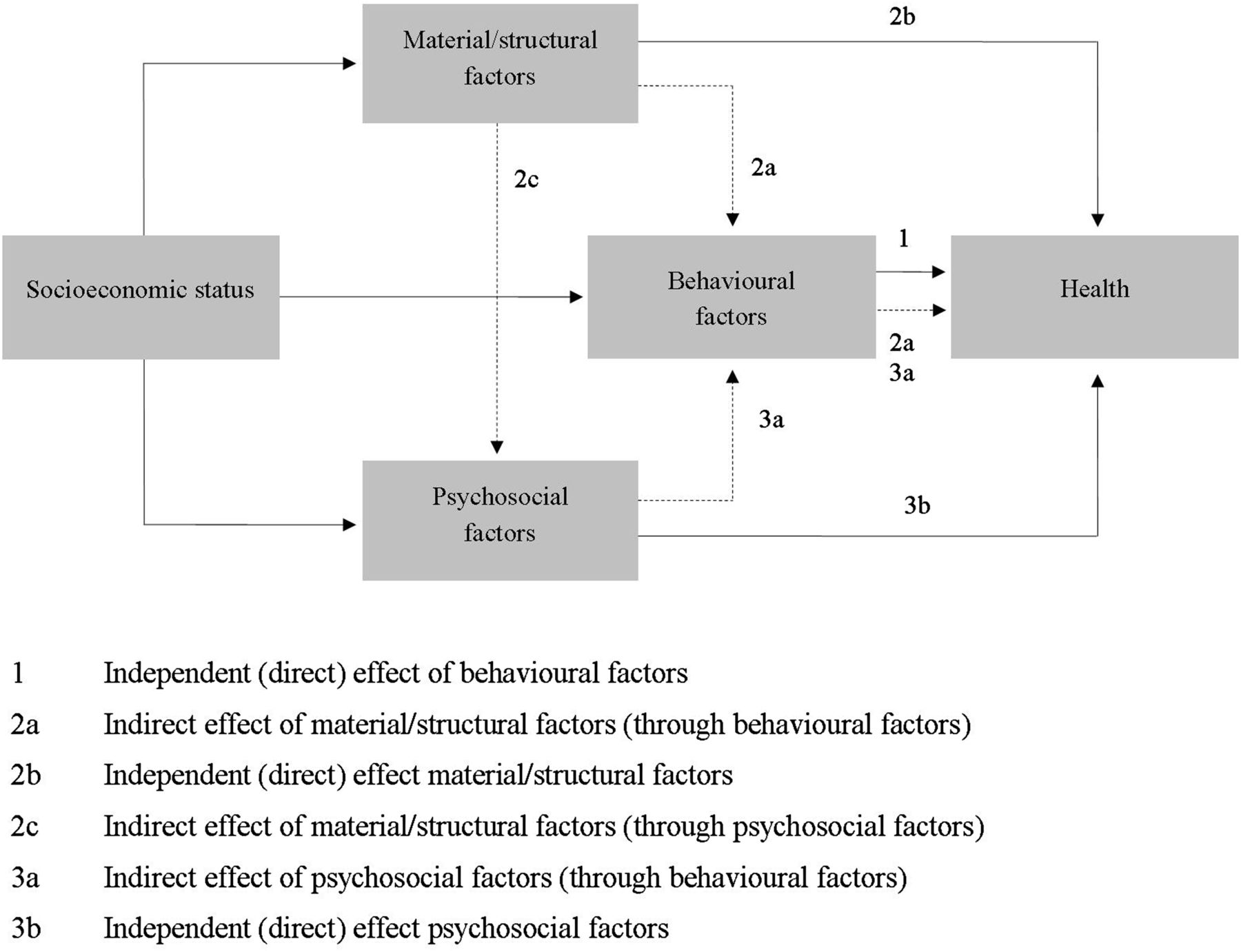
It is well established that individuals of a lower socioeconomic background have an increased risk of morbidity and premature mortality.1–4 Behavioural, psychosocial and material factors have been identified as key pathways in the explanation of socioeconomic inequalities in health.5–8 The materialist explanation postulates that health inequalities are the result of worse material and structural conditions, such as crowding, poor housing conditions and insecure or low employment status, hard physical working conditions or financial difficulties, all of which are found more often among socioeconomically deprived people.8 ,9 The psychosocial hypothesis emphasises that, for example, not only negative life events and chronic strain but also low mastery, coping or social support are unequally distributed to the disadvantage of people of lower socioeconomic status (SES) and thus contribute to social inequalities in health.10 The behavioural explanation takes into account that substance use, low physical activity and poor dietary habits are more prevalent among people of lower SES.11 So far, most studies on the explanation of health inequalities focused only on single explanatory approaches. For example, a Finnish study has shown that behavioural factors explained about half of the educational differences in cardiovascular disease mortality between the lowest and highest educational level.12 However, only the simultaneous analyses of different explanatory approaches allow a reflection of the contribution of each approach in relation to the other pathways (relative contribution). For instance, health behaviour is embedded in a social context and is, thus, influenced by a person's material and structural living conditions and psychosocial resources. Psychosocial resources also partly operate although behavioural factors, such as coping with psychosocial hazards in social relationships, may lead to harmful health behaviour, such as smoking or excessive alcohol consumption (figure 1).13 Therefore, taking into account only one explanatory approach would lead to an overestimation of single pathways instead of understanding their contribution in relation to others.
Studies, including several pathways, to quantify the relative contribution are scarce and heterogeneous. Stronks et al14 were probably the first to analyse different explanatory pathways at the same time. They showed not only that structural and behavioural factors separately contribute to the explanation of socioeconomic inequalities in health (direct effect) but also that they share a substantial contribution which can be defined as the (indirect) effect of structural determinants working through behavioural factors. Several studies from Finland,15 ,16 Germany,17 ,18 Israel,19 ,20 Korea21 ,22 or the Netherlands23–25 followed this work and expanded the explanatory model to the three main pathways. However, these analyses often used varying explanatory approaches and indicators of health and SES. They also differed in the complexity and the extent of explanatory variables.
We found only systematic reviews that focused on the relationship between material (eg, work characteristics and socioeconomic position)26 or psychosocial (eg, social capital and socioeconomic inequalities)27 or behavioural factors (eg, sedentary behaviour for youth)28 and SES. However, to the best of our knowledge, no systematic review has gathered all empirical studies, comparing the relative contribution of all three pathways (material, psychosocial and behavioural pathway) for explaining social inequalities in self-rated health (SRH). Evidence on the relative contribution of different explanatory approaches is of key importance for public health as it can be used to identify and to set priorities in terms of prevention and health promotion. After a pretest search, we found that most relevant studies included self-rated health (SRH) as outcome; therefore, we focused our review on SRH. This indicator is widely used in public health and studies show that it is a good predictor of not only objective health status, such as mortality,29 ,30 but also for disease risks.31 In addition, it is recommended as a standard indicator in health surveys.32 ,33 Therefore, the aims of this study were to (1) summarise the evidence of observational studies, analysing material, psychosocial and behavioural pathways for explaining social inequalities in SRH and (2) to assess the independent (direct) and the shared (indirect) effect of the different explanatory approaches in addition to their relative contribution.
Methods
This systematic review was conducted according to the PRISMA guidelines for systematic reviews.34 A protocol of the review process can be found as online supplementary file.
supplementary file
Search strategy
Relevant electronic metadatabases, such as PubMed and ISI Web of Science, covering a wide range of different databases were searched.35 As Stronks et al14 were the first to disentangle the relative contribution of different explanatory pathways, the search was limited from January 1996 to August 2015 and updated on 8 January 2016. Search terms included not only a variety of measures for SES, such as income, education and occupation, but also broader terms, such as social class, social position or social deprivation. For SRH, subjective and self-assessed health were also covered. A second search term, including all combinations of two of the three pathways (material, psychosocial and behavioural factors), was used and then combined with the SES and SRH term. An overview of the final search strategy can be found in table 1 (see also online supplementary table S1 for more details). Besides the databases, reference lists of obtained articles were screened and relevant studies included.
Overview of search terms
Eligibility criteria
The following eligibility criteria for inclusion were established. Similar to other systematic reviews, for example, Kröger et al36 who consider only studies analysing health selection versus social causation or Niedzwiedz et al35 who took only studies into account that consider specific life course models and their relation to health, our review follows a conceptual approach by choosing only mediation models. We included all studies that focus on explaining socioeconomic inequalities in SRH, covering at least two of the three main pathways (material, behavioural or psychosocial factors) and analysing the relative contribution of these approaches in separate and joint models. Studies were excluded if (1) they focus on only one pathway or if they include other pathways than material, psychosocial or behavioural, (2) they do not include the relevant outcome (SRH), (3) they were not empirical studies and (4) they include selected population (eg, patients with diseases). Studies that did not indicate the relative contributions of the explanatory factors but allow the calculation of these were included. The relative contribution was then calculated manually by the lead author (IM). Although material factors often also cover working conditions, studies focusing only on working characteristics were not considered in the review, as they only partly reflect the materialist pathway and are dependent on the economic sector.
Study selection and data extraction
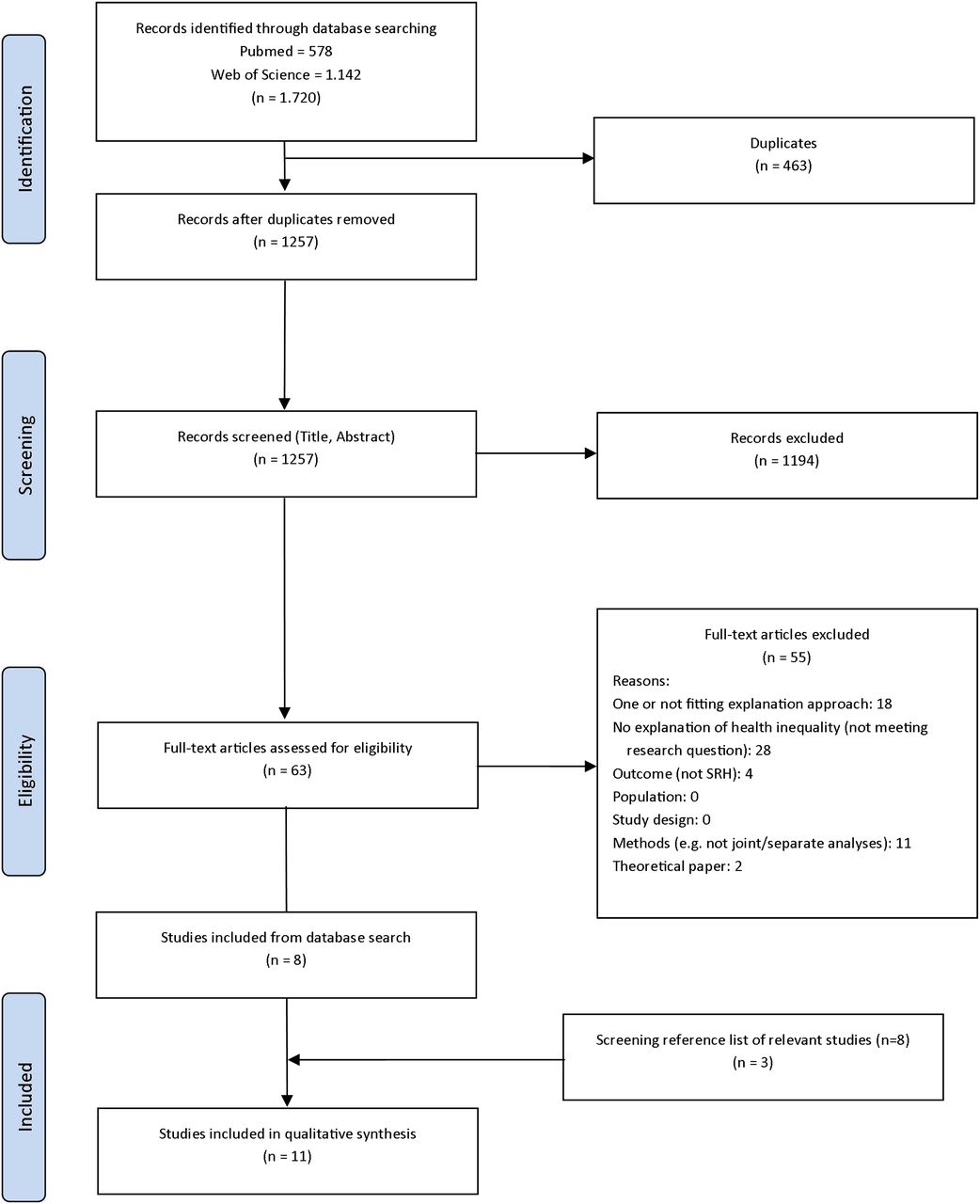
The search generated 1720 articles that were screened by two reviewers (IM and SC) based on title and abstract.37 Sixty-three full texts were retrieved for further assessment, eight of them met the criteria and were included in the systematic review (figure 2, PRISMA flow diagram). Three more references could be included after screening the references of obtained articles. When there was doubt, a third reviewer was enlisted to reach an agreement (MR). Data synthesis was performed by the extraction of general information about the study (authors, published year, country), study characteristics (sample size, study design, age group, survey), participant demographics (age, gender), measurement of SES and pathways taken into account (material, behavioural, psychosocial and others). These are presented in table 2.
Data syntheses of study characteristics

{kind=link}
{kind=link}
PRISMA (2009) flow diagram for search strategy.
Critical assessment and level of evidence
To evaluate the methodological quality of the studies, the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement was used.38–40 Those items of the checklist were selected, which are relevant for evaluating the included studies based on the study design and the aim. For every item, 0 (not fulfilled), 0.5 (partly fulfilled) or 1 (fulfilled) point was assigned and presented in percentage of maximum points achieved. The quality assessment was carried out by two independent reviewers (IM and SC), and discrepancies were discussed with a third reviewer until consensus was reached (MR).
Results
Characteristics of included studies and study quality
Table 2 presents a summary of the studies included in this review. In total, 11 publications from 9 data sources met the criteria for inclusion in this review. There has been a considerable increase in efforts to disentangle the relative contribution of different pathways over the years, as most of the publications (n=8) were published after 2009. All publications are based on cross-sectional data. Sample sizes range from 90219 to 117 460.18 Two publications each were from Israel, Finland and Germany and one publication was each from Japan, Norway and the UK. Two publications included cross-national data.18 ,41 Almost all studies focused on adulthood or older population (n=9), but only Richter et al42 and Moor et al18 analysed young people. Measures of SES included educational level (n=4), occupational status (n=3), an index of SES (n=2) and income (n=1) for adults and the Family Affluence Scale for adolescents (n=2). More than one measure of SES was included in three publications. Behavioural factors were considered in almost all studies (n=10), followed by material/structural factors (n=8) and psychosocial factors (n=8). Besides the three pathways, four studies also took other pathways into account, such as community factors (n=1), childhood circumstances (n=1), cultural (n=1) or occupational factors (n=1). In regard to different combinations of the pathways, three publications included at least psychosocial and behavioural factors, three studies included material/structural and behavioural factors, one included material/structural and psychosocial factors and four studies considered all three.
Study quality scores of the studies ranged from 63% to 83% (table 2). The quality of the studies was reduced, in particular, when studies, for example, failed to describe potential sources of bias in their methodology or were not clear on the methods. Most of the included articles clearly described the background and rationale for the studies as well as the discussion part with methodological limitations.
Measurements of material, behavioural and psychosocial factors
There was no ‘gold standard’ for measuring material, psychosocial or behavioural factors leading to an inconsistent measurement of these factors (table 2). However, to cover material or structural factors, studies often included living/housing conditions (eg, crowding, homeownership),41 ,43 working characteristics (eg, employment status, working conditions) or financial issues (eg, financial problems and relative income).15 ,17 ,19 One study also included current circumstances (eg, education, economic activity, family structure)44 which we considered as material/structural factors. Measurements of behavioural factors were more homogenous and often considered substance use (eg, smoking, alcohol consumption), physical activity and dietary habits.18 ,19 ,43 ,44 Psychosocial factors focused on perceived stress,7 social support, coping efficacy or life events.19 ,42 There was also an overlap in the measurement of material factors and SES indicators. For example, two studies included household income as part of material factors;15 ,45 however, household income was also used as SES indicator in another study.43
Separate analyses
The contributions of material, psychosocial and behavioural factors in explaining social inequalities in SRH were extracted from each study and presented in table 3. Across all studies, the contributions of these factors to the explanation of socioeconomic inequalities in SRH were heterogeneous. For example, the explanatory power of material factors in separate models ranged from 11%43 to 76%,41 psychosocial factors contributed from 4%43 to 49%46 and behavioural factors from 7%43 to 45%.46 Including all explanatory approaches in the analyses, socioeconomic inequalities in SRH could be explained by 20%43 to 100%.41 However, in separate analyses, the majority of the studies (n=6) showed that the contribution of material factors was higher than that of other pathways.15 ,17 ,19 ,41–43 Besides the three key pathways, other pathways, such as occupational factors (35–52%)41 and community factors (26%),19 also show a high separate contribution. Childhood circumstances had a very low (8%) contribution, and cultural factors made none contribution to the explanation of social inequalities in SRH.19 ,44
Contribution of material, psychosocial and behavioural factors to the explanation of social inequalities in SRH (results of separate and joint analyses with direct and shared (indirect) effects, in %)
Joint analyses
Seven of 11 studies provide analyses of independent (direct) and shared (indirect) effects.15 ,17–19 ,41 ,42 ,46 They showed that the independent (direct) contribution of material factors was generally higher than that of psychosocial and behavioural factors. Furthermore, the contribution of material factors has an additional indirect (shared) effect, as their contribution was working—to a larger extent—through psychosocial35 and/or behavioural factors.17 Psychosocial factors were also acting indirectly through behavioural factors,18 ,46 while the independent contribution of behavioural factors was generally quite low and ranged from 5%19 to 22%.42
Results by SES indicator, gender and age
Independently of SES indicator, material, psychosocial and behavioural factors contribute to the explanation of social inequalities in SRH. Occupational status (n=3) and educational level (n=4) were most often used as SES indicators. Inequalities by occupational status could be explained by 22%43 to 100%,41 while educational inequalities in SRH were explained by 42%45 to 56%.44 Seven studies adjusted for gender; four studies did a gender-specific analysis that distinguished differences between males and females. In total, the included pathways explained more inequalities in SRH in females than in males,15 ,42 ,43 with the exception of Aldabe et al.41 Material, psychosocial and behavioural factors were not only relevant in adulthood and older age but also for explaining social inequalities in adolescent SRH.18 ,42 The results reveal that in total from 53%18 to 84%42 of health inequalities in young people could be explained.
Discussion
The study is the first to systematically review the evidence on studies which quantify the relative contribution of material, psychosocial and behavioural factors in explaining socioeconomic inequalities in SRH. Although the results are quite heterogonous, we made several observations: (1) studies using separate analyses of material, psychosocial and behavioural factors show that they all are important pathways contributing to the explanation of socioeconomic inequalities in SRH. (2) However, joint analyses illustrate the ‘overlap’ between the pathways, indicating that material factors contribute more because of their stronger independent (direct) effect and additional shared (indirect) effect though psychosocial and behavioural factors. (3) The independent contribution of psychosocial and behavioural factors is much lower than that of the separate analyses initially suggested and shows that their effect is shared with material factors. (4) These results seem to be largely independent of gender, SES indicator and age.
Interpretation and comparison
We found material, psychosocial and behavioural factors to be important explanatory variables for socioeconomic inequalities in health. Other studies support our results for explaining social inequalities in mortality and morbidity.6 ,24 ,47–49
Although these studies show that multiple mechanisms are important to comprehend the causes of socioeconomic inequalities in health, health behaviour has been the focus of research and health promotion, while material living conditions were rarely considered.50 ,51 This raises the risk of ‘blaming the victim’52 by postulating an individual attribution of responsibility which is, in fact, a social and structural mechanism, shaping individuals' circumstances and beyond individual control.53 Our findings support the materialist hypothesis as material factors revealed the strongest mediating effect on the association between SES and SRH as they also affect psychosocial resources and health-related behaviour.24 ,48 ,54 ,55 Thus, health behaviour can be rather seen as a consequence of these contextual conditions. Health policy that focuses solely on a change in the individual lifestyle will have limited success, not only because health-damaging behaviour is substantially socially determined50 but also because of the influence of health behaviour is often overestimated.
Our results underline that studies need to include different pathways in order to quantify their relative importance, considering the direct as well as shared contribution. Moreover, further pathways, such as occupational or community factors, should be taken into account in order to prove their contribution. As these pathways were represented in only one study in this review, interpretation is limited. Other studies show that working conditions26 ,49 or biological factors56 are also relevant when explaining socioeconomic inequalities in health should, therefore, be included in further studies.
Strengths and limitations
The review has strengths and limitations. We followed current recommendations for systematic reviews using the PRISMA guidelines.34 Using different search terms and combinations in international databases revealed the majority of relevant publications. However, some limitations need to be acknowledged. First, it is possible that some relevant studies were not found or had not been published with no or not significant effects (publication bias). Second, the different characteristics of the studies limit their comparison across studies because of various criteria for defining material, psychosocial and behavioural factors as well as because of the selection of the variables and the amount of variables included to represent one pathway which differed across the studies and probably reduced their influence.19 For instance, one study used only perceived stress to represent the psychosocial pathway.43 Another study used only household income to define the material pathway.45 Furthermore, the use of some indicators in different national contexts might influence the results of the studies. For example, material living conditions in Israel might have a different value than material factors in Germany. Third, it is important to acknowledge that the relative contribution of the included factors should be considered as approximate measures of importance rather than as ‘absolute parameters’,24 particularly since the relative contribution depends on how many approaches are included. Therefore, the rank of the pathways in accordance with their relevance is more important than the absolute percentage of the results. The percentage change is sensitive to the inclusion of explanatory approaches or variables and thus vary between the studies, while the main conclusion—that material factors are most important—is shown in the majority of studies. Fourth, all of the included studies are based on cross-sectional data which limit the possibility of causality. Studies with longitudinal data would be able to examine the causal pathway. Longitudinal studies support our interpretation as they show that social status is more likely to affect health through material, psychosocial and behavioural factors than the other way round.23 ,57 However, there is also evidence for selection effects, for example, health behaviour, to effect on educational attainment.58 Future research should consider material, psychosocial and behavioural factors (or even more pathways) in a joint analysis using longitudinal data. Fifth, the outcome, SRH, needs to be discussed. Although there are good reasons to use SRH, there is a lack of information regarding the consistency of perceptions about SRH across populations in different cultural and socioeconomic contexts.59–61 It is widely used in public health but also poorly understood why SRH has a prognostic value for mortality.30 ,62 In our review, all studies dichotomised SRH; however, some studies used four and some five response categories. The way the response categories were dichotomised also varied between the studies. Although the distributions of SRH are not directly comparable between the studies, Jürges et al63 ,64 and Jylhä30 argue that they represent a parallel assessment of the same phenomenon and that they show concordant answers. Finally, there are more recent methods regarding mediation analysis which none of the included studies used, for example, alternative methods, such as marginal structural models (using inverse probability weighting),65 ,66 indirect effects for non-linear models using rescaling67 or inverse OR-weighting.68 Further studies using these new methods could help to reveal whether the findings are similar or whether there are differences between the methods.
Conclusion
Despite some methodological limitations, this review has several important insights for explaining socioeconomic inequalities in SRH. The results of the systematic review emphasise that studies aiming to explain social inequalities in health need to consider more than one pathway. Our review might serve as evidence for policymakers that multiple factors are important for tackling social inequalities in health. Priority should be given to material/structural living conditions as they shape conditions of psychosocial resources and health behaviour. Focusing on material conditions does not include financial resources alone, the living and working conditions are also of high relevance and contributed to the explanation of socioeconomic inequalities in SRH. Further systematic evidence is needed to evaluate whether the results of this review can be applied to other health outcomes, such as mortality and morbidity, by adding more explanatory mechanisms (eg, biomedical, cultural or working characteristics) besides material, psychosocial and behaviour factors.
What is already known on this subject
Previous research on the explanation of health inequalities emphasises the importance of material, psychosocial and behavioural factors.
So far, the available evidence on the contribution of material, psychosocial and behavioural factors has not been systematically reviewed.
What this study adds
The findings showed that all three factors contribute to the explanation of socioeconomic inequalities in self-rated health. However, material factors contribute the most due to their higher independent (direct) and additional shared (indirect) effect through psychosocial and behavioural factors.
Health policy should focus on material/structural living conditions as they shape the conditions of psychosocial resources and health.
Acknowledgments
The authors thank Astrid Fink and Sara L Schröder for the helpful comments on the manuscript. The authors also thank Sandra Cieslak for helping to screen the references and critical assessment of the included studies.
References
Footnotes
Contributors IM designed the study and had primary responsibility for all parts of the study, including the methods and the search, writing the draft and the interpretation of the data. MR provided substantial contributions by critical feedback on the conception of the study and revisions of the draft. JS assisted in reviewing and finalising the manuscript. All authors read and approved the final manuscript.
Funding This study is part of the project ‘Explaining health inequalities in adulthood. A life course perspective using the German Socioeconomic Panel study (SOEP)’, which is funded by the German Research Foundation (DFG), with grant agreement number RI2467/2-1.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.