Article Text

Abstract
Background Low socioeconomic status (SES) is a known risk factor for cardiovascular disease (CVD) but whether its effects are comparable in women and men is unknown.
Methods PubMed MEDLINE was systematically searched. Studies that reported sex-specific estimates, and associated variability, of the relative risk (RR) for coronary heart disease (CHD), stroke or CVD according to a marker of SES (education, occupation, income or area of residence), for women and men were included. RRs were combined with those derived from cohort studies using individual participant data. Data were pooled using random effects meta-analyses with inverse variance weighting. Estimates of the ratio of the RRs (RRR), comparing women with men, were computed.
Results Data from 116 cohorts, over 22 million individuals, and over 1 million CVD events, suggest that lower SES is associated with increased risk of CHD, stroke and CVD in women and men. For CHD, there was a significantly greater excess risk associated with lower educational attainment in women compared with men; comparing lowest with highest levels, the age-adjusted RRR was 1.24 (95% CI 1.09 to 1.41) and the multiple-adjusted RRR was 1.34 (1.09 to 1.63). For stroke, the age-adjusted RRR was 0.93 (0.72 to 1.18), and the multiple-adjusted was RRR 0.79 (0.53 to 1.19). Corresponding results for CVD were 1.18 (1.03 to 1.36), 1.23 (1.03 to 1.48), respectively. Similar results were observed for other markers of SES for all three outcomes.
Conclusions Reduction of socioeconomic inequalities in CHD and CVD outcomes might require different approaches for men and women.
- Epidemiology of cardiovascular disease
- SOCIAL INEQUALITIES
- META ANALYSIS
- CORONARY HEART DISEASE
- STROKE
Statistics from Altmetric.com
Introduction
Despite tremendous advances in the prevention and treatment of coronary heart disease (CHD) and stroke over the past 2 decades, cardiovascular disease (CVD) remains the leading cause of death in women worldwide, with an estimated 8.6 million women dying each year from a cardiovascular-related disorder.1 Moreover, despite the longevity of the widely held misperception that CVD affects mainly men, the absolute burden of CVD mortality in the USA is higher in women than men.2 Recent American Heart Association Scientific Statements highlighted the existence of important sex differences—most often to the detriment of women—at all points along the cardiovascular clinical spectrum beginning with how CVD presents through to its diagnosis, treatment and outcomes.3–5 These sex differences may be responsible for the excess rates of CVD in women. In particular, there is a growing awareness that there are a number of barriers that inhibit women from accessing timely and appropriate treatment for CVD that are thought to include social deprivation and poor educational attainment.
In high-income countries, it is well established that socioeconomic status (SES) is inversely related to the risk of CVD,6 7 with greater risks of CHD8–9 and stroke10 mortality and morbidity generally observed among individuals with a lower education, a lower income and for those living in more disadvantaged areas. In low-income and middle-income countries, the evidence is less consistent and dependent on a range of factors, including the stage of epidemiologic transition and the outcome examined.11 12 Although the evidence generally suggests that socioeconomic inequalities in CVD are more consistent and stronger in magnitude for women compared with men, the literature is inconsistent.13–15 Variations in reported sex differences in the relationship between SES and CVD likely result from a range of factors, including the choice and categorisation of SES indicator, the CVD outcome examined and methodological differences such as adjustment variables or may simply result from chance.16 17
To date, there has been no systematic synthesis of the literature comparing sex differences in the relationship between markers of SES and CVD. We, therefore, conducted a systematic review and meta-analysis to ascertain the most reliable estimate of the sex differences in the relative risks (RRs) of SES on the risk of incident CHD, stroke and CVD in the general population.
Methods
Search strategy and selection criteria
We searched PubMed MEDLINE (http://www.ncbi.nlm.nih.gov) on 14 September 2015 using a pre-defined combined text word and MeSH heading search strategy (see online supplementary appendix methods 1). The reference lists of all relevant original research and review articles were scanned to capture any further citations. All retrieved articles were scanned for inclusion and exclusion by two authors; any disagreements were mediated with a third author. A modified version of the Newcastle-Ottawa Quality assessment scale (see online supplementary appendix table S1) was used to assess the quality of included studies.
supplementary appendix
Cohort studies were included if they reported sex-specific RRs, or equivalent, together with a measure of variability, on the relationship between any indicator of SES and CHD, stroke or CVD among adults. In the event of missing information within a potentially relevant paper, we contacted authors for additional information. Studies were excluded if the available results were not adjusted for at least age, or if they were selected on the basis of a prior CVD event or an underlying pathological disorder.
Individual participant data (IPD) from four studies available to the authors were also used: the Asia Pacific Cohort Studies Collaboration (APCSC), the Atherosclerosis Risk in Communities Study (ARIC), the National Health and Nutrition Examination Survey III (NHANES) and the Scottish Heart Health Extended Cohort Study (SHHEC).6 ,18–20 The primary endpoints were combined fatal and non-fatal incident CHD, stroke or CVD. Where studies reported results for fatal outcomes only, we used this end point in our analyses; otherwise risks for combined fatal and non-fatal outcomes were used. We did not extract RRs according to different subtypes of stroke as insufficient data were available within the included studies. We extracted RRs for each sex both adjusted for age, without other CVD risk factors, and multiple adjusted, choosing adjustment sets that most closely matched to the conventional CVD risk factors (ie, smoking, diabetes, total cholesterol, high-density lipoprotein cholesterol and systolic blood pressure), while avoiding adjustment sets that included other measures of SES.
Statistical analysis
The meta-analysis was performed in accordance with the Meta-Analyses and Systematic Reviews of Observational Studies (MOOSE) guidelines.21 For each study, we pooled the sex-specific RRs for (where available) CHD, stroke and CVD for individuals in the lowest SES group versus individuals in the highest SES group. For the IPD studies, HRs (regarded as RRs) were obtained using Cox proportional hazards regression models. APCSC data were stratified by Asian and non-Asian countries for all analyses. The RRs of the two extreme categories, most socioeconomically disadvantaged versus least, were log transformed and pooled across studies using random effects meta-analysis with inverse variance weighting and then back transformed to obtain the pooled RR separately for women and men. To compare the sexes directly, we estimated women-to-men ratios of RRs (RRRs) from each study and pooled them similarly. The SE of the RRR was calculated by (1) taking the natural logarithm of the RR (lnRR) and the upper (lnUL) and lower limit (lnLL) of the CIs for each sex, (2) calculating the SE of the sex-specific lnRRs by taking the mean of the SE of the lnLL and LnUL ((lnRR-lnLL)/1.96+(lnUL−lnRR)/1.96)/2 and (3) calculating the sum of the sex-specific variances to derive the SE of the lnRRR by taking the square root (√(SEwomen2+SEmen2). When studies stratified their analysis by subgroups (eg, age), we pooled adjusted risk estimates weighted by the inverse of their variance using fixed effects meta-analyses to obtain a single sex-specific RR. For the one study22 that only reported risks according to subtype of CVD, we pooled estimates across the subtypes in a similar way. Finally, the study-specific RRs and RRRs were pooled using random effects inverse variance weighting. The I² statistic was used to estimate the percentage of variability across studies due to between-study heterogeneity. The presence of publication bias for all primary analyses was examined using funnel plots and Begg's test.
Since the causal pathway relating SES, conventional CVD risk factors and CVD is uncertain, we decided, a priori, to take age adjustment as our primary method of adjustment. Because the majority of studies provided results for highest level of education attained, we took this as our primary measure of SES. Hence, our primary results are pooled age-adjusted RRs (and consequent RRRs) for CHD, stroke and CVD, comparing the lowest with the highest reported level of education. For this primary analysis, we also conducted predefined subgroup analyses by age (split at 60 years), region (Asia or not), study baseline period (split at 1995) and event type (combined fatal and non-fatal or fatal outcomes only). Random effects meta-regression analyses were used to test differences across subgroups. We also pooled results for the three-level categorisation of primary, secondary and tertiary education, where available. Finally, because different studies were included in the age- and CVD risk factor-adjusted analyses, we compared age- and CVD risk factor-adjusted (adjusted for age, smoking status, SBP, TC, high-density lipoprotein cholesterol (HDLC) and diabetes) analyses using the IPD studies.
All analyses were performed using Stata V.12.0. A p value <0.05 was considered to denote significance.
Results
Of the 5300 articles that were identified, 179 articles qualified for full-text evaluation (figure 1). Of these, 44 articles, with information from 89 separate cohorts, provided information on sex differences in the association between SES and CVD outcomes (see online supplementary appendix table S2). Results from these cohorts were combined with those from 27 IPD cohorts, giving a total of 116 cohorts, including over 22 million individuals (35% women)—not counting 5 studies that used Census data—and 1 078 459 events (701 617 CHD, 82 036 stroke and 294 752 CVD). All included studies were of good to very good quality (see online supplementary appendix table S1).

Flow chart of the systematic review.
In total, 22 cohorts were from Asia, 75 from Europe, 7 from North America and 12 from Australasia. Individuals were between 20 and 107 years of age at study baseline and the duration of follow-up ranged from 1 to 32 years across studies. Ninety-five cohorts gave results using educational attainment as the indicator of SES, 17 using area-level deprivation (generally based on postcodes/zip codes), 12 using type of occupation and 8 using income. The categorisation of SES indicators (thresholds for categories and number of categories) varied across studies; however, education was the most consistently categorised, with the majority of studies reporting RRs for three similarly defined groups (see online supplementary appendix table S3). Multiple-adjusted results commonly adjusted for at least smoking, diabetes, blood pressure and cholesterol.
The pooled age-adjusted RR for CHD for the lowest versus highest level of education was 1.66 (95% CI 1.46 to 1.88) for women and 1.30 (1.15 to 1.48) for men (figure 2). These RRs remained significantly above unity when pooling results that adjusted for CVD risk factors (see online supplementary appendix figure S1). Women with the lowest level of education were at a 24% higher excess risk of CHD compared with men with the lowest level of education: age-adjusted RRR 1.24 (1.09 to 1.41) (figure 3). After adjustment for major CVD risk factors, the corresponding RRR was 1.34 (1.09 to 1.63). There was no evidence of publication bias (p=0.68; see online supplementary appendix figure S2).

Age-adjusted pooled relative risk of cardiovascular disease outcomes associated with lowest versus highest socioeconomic status in men and women. Lines show the 95% CIs. SES: socioeconomic status.
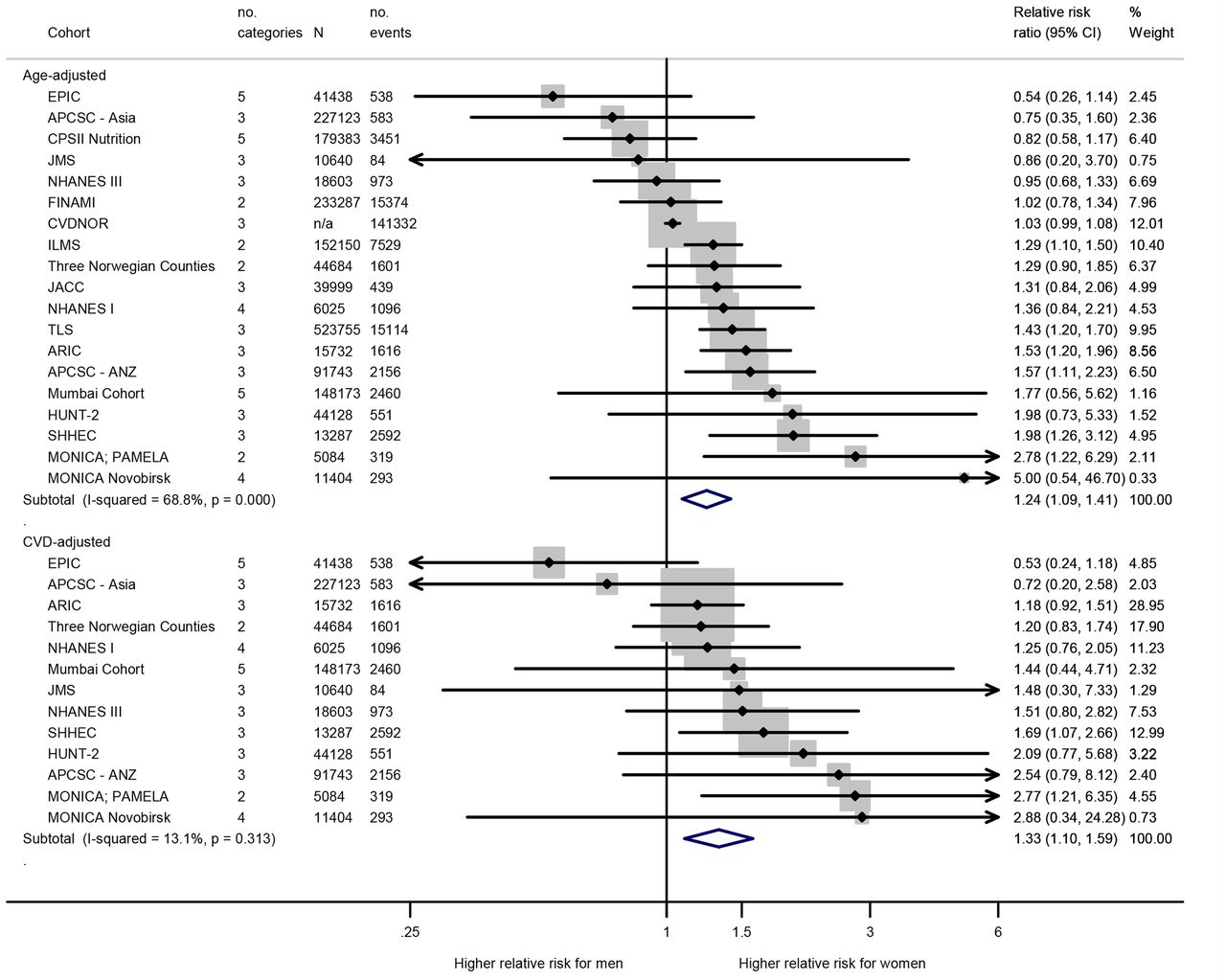
Age-adjusted and multiple-adjusted women-to-men ratio of relative risks of coronary heart disease, lowest compared with highest educational attainment. Lines, and width of the summary diamond, show 95% CIs. Boxes are in proportion to study weights. The p value is for a test of homogeneity. SES: socioeconomic status; See online supplementary appendix table S2 for full cohort names.
For SES measured by area deprivation, occupation and income, the pooled age-adjusted RRs comparing extreme categories were broadly similar to those observed for education for both sexes (figure 2), and remained largely unchanged following multiple adjustments (see online supplementary appendix figure S1). The pooled women-to-men age-adjusted RRRs for CHD were 1.19 (1.09 to 1.29) for highest versus lowest level of area deprivation (see online supplementary appendix figure S3), 1.21 (0.92 to 1.61) for lowest versus highest level of income (see online supplementary ppendix figure S4) and 1.14 (1.04 to 1.48) for manual versus non-manual occupation (see online supplementary appendix figure S5). The corresponding multiple-adjusted RRRs were 1.16 (0.98 to 1.37), 1.03 (0.74 to 1.42) and 0.99 (0.63 to 1.56), respectively.
For stroke, the pooled age-adjusted RR for stroke for lowest versus highest education was 1.34 (1.07 to 1.69) for women and 1.53 (1.27 to 1.86) for men (figure 2); both remained significantly in excess of unity when pooling multiple-adjusted results (see online supplementary appendix figure S1). There was no evidence for a difference between women and men in the excess risk of stroke associated with the lowest level of education versus the highest: the pooled age-adjusted RRR was 0.93 (0.72 to 1.18) (figure 4). There was weak evidence of publication bias (p=0.06).

Age-adjusted and CVD risk factor-adjusted women-to-men ratio of relative risks of stroke, lowest compared with highest educational attainment. See figure 3 for explanations.
For all the three alternative measures of SES, the pooled age-adjusted RRs for stroke were broadly similar to those observed for education in both sexes, and when the estimates were adjusted for other CVD risk factors (figure 2 and see online supplementary appendix figure S1). The pooled age-adjusted RRRs of stroke were 0.98 (0.82 to 1.18) for highest versus lowest level of area deprivation, 1.09 (0.86 to 1.38) for lowest versus highest level of income and 1.22 (0.72 to 2.06) for manual versus non-manual occupation (see online supplementary appendix figures S6–8). Similar results were obtained using multiple adjustments.
The pooled age-adjusted RR for CVD for the lowest versus highest level of education was 1.66 (1.43 to 1.92) for women, and 1.42 (1.25 to 1.63) for men; both remained significantly in excess of unity when pooling studies that adjusted for other CVD risk factors (figure 2 and Appendix figure 1). The pooled age-adjusted RRR of CVD for women compared with men associated with level of education was 1.18 (1.03 to 1.36; figure 5), with no evidence of publication bias (p=0.74). Pooled estimates that adjusted for CVD risk factors were similar in magnitude to those observed for age-adjusted analyses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age-adjusted and CVD risk factor-adjusted women-to-men ratio of relative risks of cardiovascular disease, lowest compared with highest educational attainment. See figure 3 for explanations.
The lowest SES was associated with a greater risk of CVD than the highest SES in women and men, when area-level deprivation or level of occupation was used to measure SES; these elevated RRs remained statistically significant after further adjustment. The age-adjusted RRRs for CVD were 1.08 (0.98 to 1.19) for highest versus lowest level of area deprivation (see online supplementary appendix figure S9) and 1.06 (0.91 to 1.24) for manual versus non-manual occupation (see online supplementary appendix figure S10), and were similar following adjustment for other CVD risk factors. Lack of data precluded analysis by income.
There was no evidence that the age-adjusted RRRs of CHD, stroke or CVD associated with education differed materially by age, baseline study period, region or outcome (fatal and non-fatal or fatal only) (see online supplementary appendix figure S11). The RRRs for CHD and CVD, comparing tertiary with primary educational attainment were higher than the RRRs comparing secondary with primary educational attainment, suggesting a socioeconomic gradient in these sex differences. No such educational gradient was observed for stroke (see online supplementary appendix figure S12). RRRs did not substantially differ when comparing age- and multiple CVD risk factor-adjusted analyses using the IPD studies (see online supplementary appendix table S4).
Discussion
In this large-scale meta-analysis with information on more than 1 million incident CVD events, indices of SES were inversely associated with cardiovascular risk in both sexes but, the association with CHD and CVD was significantly stronger in women: the excess risk of CHD and CVD associated with the lowest, compared with the highest, level of education attained was 24% and 18% greater for women compared with men, with similar results for other measures of SES. For stroke, there was no evidence of a sex difference with SES.
While our search was not restricted to particular countries, our results are derived primarily from studies conducted in high-income countries. Although we did not find any statistical evidence of effect modification by region (Asia or not), we cannot preclude the possibility that having more data from low- and middle-income countries may have altered our findings. The transition from rural to urban lifestyles in many lower middle-income countries is resulting in a greater prevalence of major vascular risk factors across the population,23 which may differ by sex. For example, cigarette smoking is generally far more common among men compared with women in lower middle-income countries, whereas obesity is generally more prevalent among women in some of these countries.23 Understanding the role of sex in this transition will be particularly important to allocate (often limited) preventive resources to those who stand to benefit most. Our review highlights a necessity for additional studies to examine this within low- and middle-income settings.
The mechanisms underpinning this excess cardiovascular risk conferred by low SES in women, compared with men, remain speculative but they are unlikely to be governed solely by sex differences in major risk factors for two reasons. First, adjustment for conventional CVD risk factors (for both the pooled analyses and when comparing age- and CVD risk factor-adjusted analyses within the IPD studies) did not remove the excess cardiovascular risk associated with education in women. Second, these risk factors also impact on stroke risk for which there was no evidence of a sex difference. We have previously published results that show a female disadvantage in terms of excess risk of CHD conferred by diabetes24 and smoking,25 and similar, but weaker, corresponding results for stroke26 ,27—so these two risk factors are prime candidates for explaining the sex differences (or lack of) seen here. However, when adjusting for diabetes, in addition to age, smoking, total and HDLC in our IPD studies, we found no appreciable differences in the RRRs for lowest versus highest education level for CHD, stroke or CVD (see online supplementary appendix table S5). A similar lack of effect of additional adjustment for smoking was found in our IPD. It is plausible, however, that sex differences in the influence of SES on alternative risk factors, such as diet, physical activity and/or psychosocial factors, which may not have been fully accounted for with the traditional CVD risk factors, including anthropometry, that were adjusted for in our included studies, may play a role.
An additional explanation for the observed sex differences observed for CHD and CVD may be differential identification of high CHD and CVD risk and access and adherence to preventative treatment and risk factor management for men and women across levels of socioeconomic disadvantage. Adults with a lower SES and women, more generally, have been shown to be less likely to initiate and receive preventive treatments for CVD in some,28 ,29 but not all,30 ,31 studies. For example, several studies have demonstrated that compared with men, women with acute myocardial infarction present later—with up to a day and a half later in one study.32 ,33 Needless to say, such delays in seeking treatment will have significant adverse effects on subsequent outcomes. Treatment delays in women, due either to a longer time until presentation, time to diagnosis and/or time to treatment, are frequently attributed to a woman's lower risk awareness and less typical clinical presentation of acute coronary symptoms.3 Sex differences in treatment delays for acute stroke symptoms are generally smaller or absent.33
In most of our analyses, to be able to pool the maximum number of studies, we pooled estimates from the extreme categories of SES indicators. However, there is a known socioeconomic gradient in the risk of CVD,6 and the sex differences that we have observed may also occur across the socioeconomic gradient. We were only able to show such a gradient in the RRRs in women compared with men for three education groups in a restricted number of studies. As with the main results, this gradient was seen for CHD and CVD, but not stroke.
The main strengths of this meta-analysis were the large number of participants, the diversity of study populations included and our subgroup analyses to explore possible sources of heterogeneity in our data. Nonetheless, unexplored heterogeneity in the definitions of SES and CVD outcomes across included studies is likely. Even when SES indicators appeared to be defined in a similar manner, the scale of SES exposure may differ as a result of country-specific educational systems, economic situations and neighbourhood settings. Likewise, the definition of CVD outcomes varied considerably between studies. However, we would not expect such sources of variation to have materially influenced our conclusion concerning sex differences, as we deliberately only included studies that had data form both sexes, and any variation from the norm should have affected men and women from the same study to a similar extent.
Our results expand the growing body of evidence of clinically meaningful sex differences in risk factors for CVD and have several implications for the way in which CVD preventive measures are developed and targeted, at least in high-income countries. First, our findings support the release and implementation of sex-specific clinical guidelines for CVD3–5 ,34 and indicate these should emphasise more strongly the importance of the socioeconomic inequalities on cardiovascular health in women as well as in men. In particular, our observation that SES remains a strong independent risk factor for all CVD outcomes, even after accounting for traditional CVD risk factors and with disproportionally stronger effects in women than men, supports the continued development and implementation of sex-specific CVD risk scores into clinical guidelines and practice, which incorporate a measure of socioeconomic disadvantage.34 Second, in future attempts to reduce socioeconomic inequalities in CVD, it is likely that prevention and treatment efforts will need to be tailored to men and women and for different local contexts. A recent analysis of the determinants of educational inequalities in CHD in 15 European populations showed that these determinants vary by region and sex. For example, smoking was identified as the major mediator of CHD inequalities among European men, but not for women from Central/South and East Europe where less educated women were less likely to smoke. In this study, HDLC was identified as the main driver of the socioeconomic inequalities in CHD observed for European women.35 Similar sex differences in the socioeconomic patterning of CVD risk factors have been identified in other studies.36 Further, a focus on particularly intense risk detection among disadvantaged women and targeting of prevention and management strategies (in the primary care and public health context) on non-traditional CVD risk factors for socially disadvantaged women may be required.
Our study also emphasises the importance of the design, evaluation and implementation of effective interventions aimed at decreasing treatment delays (ie, time to presentation, time to diagnosis and/or time to treatment), particularly for women from disadvantaged backgrounds. Interventions outside of the health sector (eg, in the labour market) may also be required to address possible psychosocial drivers of these sex differences.37–39 However, such efforts should be guided by an improved understanding of how cultural and societal differences between men and women affect risk factor behaviour and health outcomes. All such prevention and management efforts should be directed to women across the gradient of socioeconomic disadvantage with the scale and intensity proportionate to the level of disadvantage to address the socioeconomic gradient in health rather than simply the ‘gap’.39 A better understanding of the causes of these sex differences may enable a more effective reduction of socioeconomic inequalities in CHD risk for women. Finally, our results demonstrate that education represents a consistent and robust marker of SES to target prevention and management strategies in cardiovascular health.
What is already known on this subject
Although the evidence generally suggests that socioeconomic inequalities in cardiovascular disease (CVD) are more consistent and stronger in magnitude for women compared with men, the literature is inconsistent. A better understanding of possible sex differences of the relationship between socioeconomic status (SES) and CVD outcomes will enable preventive and management strategies to be better targeted, and thereby lead to a more effective reduction of socioeconomic inequalities in CVD.
What this study adds
In this large-scale meta-analysis with information on more than 1 million incident CVD events, indices of SES were inversely associated with cardiovascular risk in both sexes but, the association with coronary heart disease and CVD was significantly stronger in women compared with men. These results suggest that tailored interventions and risk assessment strategies aimed at reducing the burden of CVD are required, particularly for women from disadvantaged backgrounds.
References
Footnotes
KB and SAEP contributed equally.
Twitter Follow Kathryn Backholer at @KBackholer
Contributors KB, SAEP and MW designed the study and drafted the paper. KB, SAEP and SHB collated and analysed the data. AP and RRH contributed to interpretation of results and redrafting of the manuscript.
Funding KB is supported by a National Heart Foundation of Australia (NHF) Post-Doctoral Fellowship (PH 12M6824) and Collaboration and Exchange Award. MW was supported by an Australian National Health and Medical Research Council (NHMRC) Principal Research Fellowship. AP is supported by a NHMRC Career Development Award.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.