Article Text

Abstract
Background Alcohol policies around the world seek to delay the initiation of drinking. This is partly based on the influential idea that earlier initiation is likely to cause adult alcohol problems. This study synthesises robust evidence for this proposition.
Methods Systematic review of prospective cohort studies in which adolescent measurement of age of first drink in general population studies was separated by at least 3 years from adult alcohol outcomes. EMBASE, Medline, PsychINFO and Social Policy and Practice were searched for eligible studies, alongside standard non-database data collection activities. Data were extracted on included study methods and findings. Risk of bias and confounding was assessed for individual studies and a narrative synthesis of findings was performed.
Results The main finding was the meagre evidence base available. Only five studies were eligible for inclusion in this review. The existence of effects of age of first drink on adult drinking and related problems were supported, but not at all strongly, in some included studies, and not in others. Rigorous control for confounding markedly attenuates or eliminates any observed effects.
Conclusions There is no strong evidence that starting drinking earlier leads to adult alcohol problems and more research is needed to address this important question. Policy makers should, therefore, reconsider the justification for delaying initiation as a strategy to address levels of adult alcohol problems in the general population, while also addressing the serious acute harms produced by early drinking.
- ALCOHOL
- ADDICTIVE BEHAVIOUR/ADDICTION
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Across the world a key aim of alcohol policy is to delay the age at which alcohol is first drunk, most obviously with legal minimum purchase ages.1 A key rationale for such policies is that an earlier age of first drinking (AFD) makes alcohol problems in adulthood more likely. For example the US Surgeon General's Call to Action on underage drinking states that; “approximately 40% of individuals who report drinking before age 15 also describe their behaviour and drinking at some point in their lives in ways consistent with a diagnosis for alcohol dependence. This is four times as many as among those who do not drink before age 21” (Ref. 1, p. 12). Similarly, the official UK guidance on alcohol consumption, which advises against any drinking before the age of 15 years, is supported by the statement that “early age of drinking onset is associated with an increased likelihood of developing alcohol abuse or dependence in adolescence and adulthood”(on page 52).2
Although, the US and UK guidance documents cite a number of, mostly cross-sectional, studies to support the proposed association between earlier AFD and harmful alcohol use in adulthood, a systematic appraisal of the nature and strength of the relationship between AFD and later harmful alcohol use has not previously been performed.3–6 An understanding of this relationship is important to determine the value of preventive interventions in reducing longer term alcohol harms.7 An underlying causal relationship between earlier AFD and adult alcohol problems could exist if there is neurobiological or other developmental impairment or if alcohol involvement is otherwise promoted, for example via peer networks. If any such causal relationship exists, widely delivered early interventions which delay AFD could make a significant contribution to reducing population levels of alcohol problems. If there is no causal relationship, however, delaying age of drinking initiation will not reduce levels of adult alcohol problems, though it may still confer other benefits in relation to adolescent harms.2 Within the research community there has been debate about whether there is an underlying causal relationship between earlier AFD and alcohol problems in adulthood, and opinion has been divided on this issue.6 ,8 ,9 Obvious importance to policy and practice makes imperative evaluation of the research evidence to ascertain the strength of any associations and the likelihood of causation. Here we conduct a systematic review of cohort studies to examine the association between AFD and adult alcohol problems and consider the evidence for a causal relationship.
Methods
Cross-sectional studies are usually considered an inappropriate basis for causal inference, particularly so in relation to associations extending over time. Recall bias is an obvious threat. The longer the time interval between initiating drinking and reporting on it, the greater the scope for recall problems and telescoping forward, so as to report a later AFD.7 Adult problem drinkers may also have systematically different recall of their AFD, being more likely to report younger AFD, and/or different willingness to report it from those who do not have such problems.10 These problems also affect case-control studies. Cohort study designs which measure AFD prior to assessment of alcohol related harms provide a stronger basis for investigation of the strength of associations and consideration of possible causation. Particularly where measurement of AFD is soon after the event, they can potentially minimise recall bias and reduce the likelihood of differential reporting problems. A systematic review of cohort studies provides the strongest observational study design to evaluate evidence for causal inference.11 While experimental evidence would be preferable to observational evidence, there is sparse data on the effects of altering AFD due to the intractability of this intervention target.12
This report is guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.13 The following selection criteria were applied: Studies which defined AFD as the age at which a participant had a first drink of more than a few sips of alcohol were included, while studies which assessed only age of first intoxication or the initiation of regular drinking were excluded, because these will widely occur at a later age. Only cohort studies comprising general population samples were included, with a requirement for at least 3 years follow-up between initial measurement of AFD in adolescence and the assessment of alcohol related outcomes. This interval, somewhat arbitrarily allows for the development of problems after initiation. Included studies were also required to measure alcohol related outcomes in adulthood, defined here as 18 years or over. Studies of special populations such as children of alcoholics were excluded. Relevant alcohol related outcomes were defined as: measures of consumption, including measures of the frequency and quantity of alcohol use; Diagnostic and Statistical Manual of Mental Disorders or International Classification of Diseases defined alcohol dependence or non-dependence alcohol problems14 ,15; or other measures of harmful alcohol use, such as getting into fights while under the influence of alcohol. Studies were eligible for inclusion only if they reported the magnitude of an association between age of first drink and any of these alcohol related outcomes, for example, in the form of an OR or regression coefficient. Only peer reviewed studies were included. No language or date restrictions were applied.
A search of the following databases for eligible studies was performed from inception to the present on 10 January 2013: Medline, Embase, PsychInfo and Social Policy and Practice. The final search terms used in Psychinfo are presented in box 1. The database search was complemented by backward searching, involving screening the reference lists of included studies, and forward searching of subsequent citations of these papers. Further relevant studies were identified by contacting 20 experts in this subject area of young people's drinking, and by screening the references of a recent, related review which also informed the design of the present study.16 Screening of abstracts was undertaken by the first author and both authors independently reviewed selected full texts for suitability of inclusion.
Database search strategy used in Ovid SP to search Psychinfo.
-
(“age at onset” or “age of onset” or “ first drink” or “age at first use” or “age at initiation” or “age of initiation” or “early initiation”).ab.
-
age of onset.sh.
-
1 or 2
-
(“drinking” or “alcohol”).ab.
-
(alcohol or drinking).sh.
-
4 or 5
-
3 and 6
-
(“alcohol-related problems” or “alcohol related problems” or “alcohol abuse” or “alcohol dependence” or “problem drinking” or “problem-drinking” or “hazardous drinking” or “hazardous-drinking” or “alcohol use” or “addiction” or “alcoholism”).ab.
-
(alcohol abuse or alcohol dependence or problem drinking or hazardous drinking or addiction or alcoholism).sh.
-
8 or 9
-
10 and 7
In addition to the data presented in table 1, the following data were extracted from the included studies using a dedicated form: Type of AFD variable (binary, categorical or continuous), data collection method (self-completion questionnaire or face to face), details of statistical analyses performed, unadjusted results and findings from subgroup analyses.
Study design, methods and key outcomes of included studies
A narrative analysis of the included studies was undertaken. Meta-analyses were not performed because they were judged inappropriate due to heterogeneity in the methods and outcomes of the included studies. Primary study methods were appraised to evaluate the potential for confounding and bias, with particular attention paid to selection, attrition, recall and reporting biases. With regards to confounding, the level of control for important background psychosocial and familial risk factors for alcohol problems including socioeconomic status, family history of alcohol problems, mental health issues or other early evidence of behavioural problems was assessed.8 ,17
Results
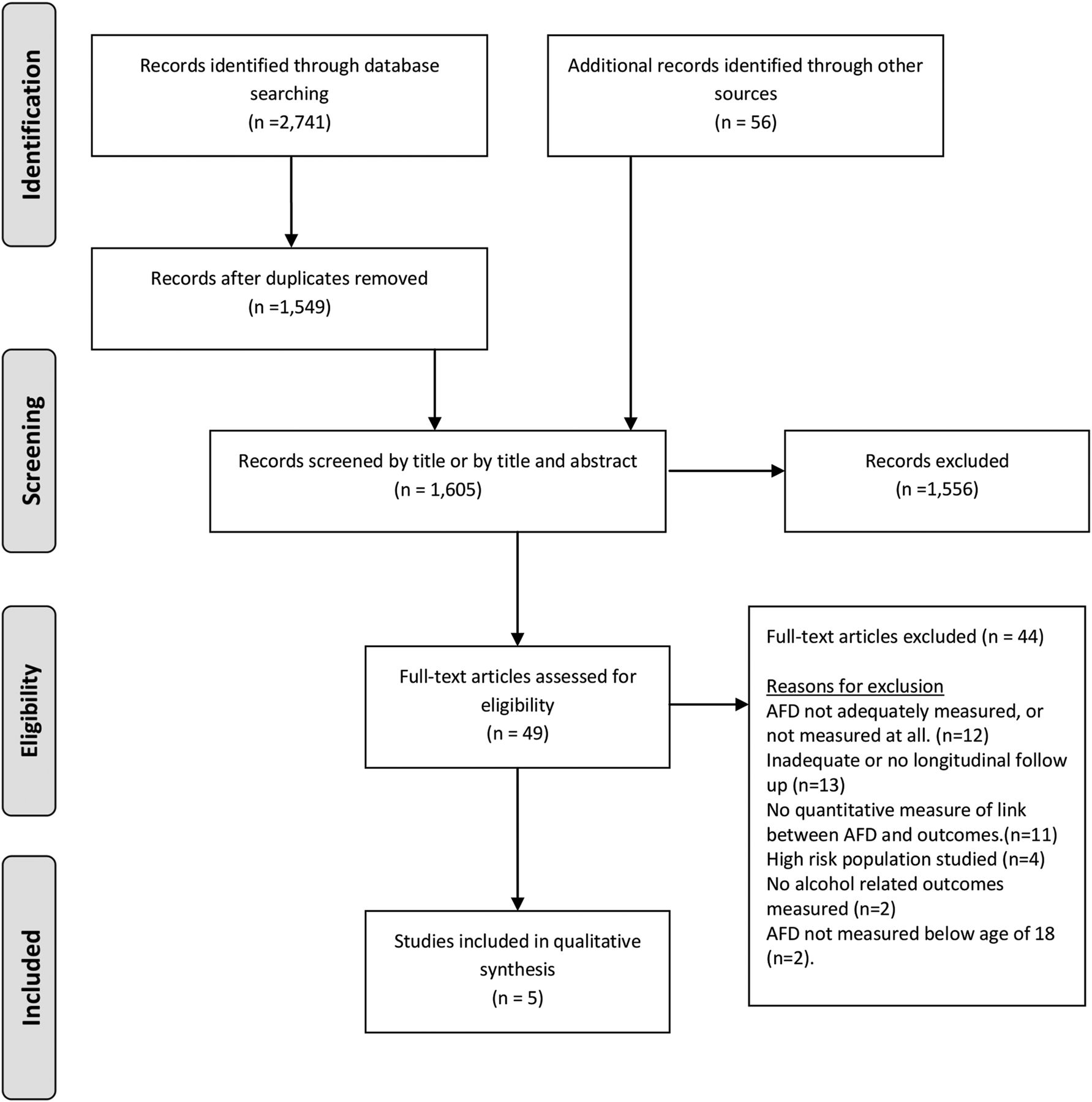
Only five studies met eligibility criteria for this review,18–22 three of which were published within the past 3 years.20–22 The PRISMA flow chart summarising the data collection process is shown in figure 1. Reports from four separate cohorts, comprising three reports from two US cohorts,19–21 and two reports from two cohorts in Norway18 ,22 were included. Sample sizes ranged from 447 19 to 1311.22 The cohorts were either school18 ,20–22 or community based.19 Study design, methods and results are summarised in table 1.
{kind=link}
Flow diagram to show process of identifying and screening studies for inclusion. AFD, age of first drinking.
Pedersen and Skrondal18 examined the effects of AFD in a school-based cohort of 522 participants. They defined AFD as consumption of a half of bottle of beer, 100 mL of wine or 25 mL of spirits and chart initiation in annual waves of data collection, using the first reported age of drinking as a continuous variable for their analysis. Outcomes were measured in a single follow-up wave at age 18–21 years. After controlling for peer and parental influences in structural equation models they identify a large independent effect, strikingly estimating that a 10% delay in AFD would lead to a 35% reduction in subsequent alcohol consumption and also a large effect on alcohol problems. The authors acknowledged that more stringent control of confounding would weaken this association and that further studies were needed.
Warner and White19 selected those who provided data at all follow-up intervals from a larger cohort study and were assessed at the earliest age of 12 years, specifically to minimise recall bias in respect of AFD (median AFD was 10 years). The final sample size was 447. They separately enquired about AFD in family and other contexts and gathered data on various aspects of the experience of the first drinking episode. They defined early AFD as reported drinking prior to age 11 years. Data on AFD were collected at age 12 years, 15 years and 18 years, with additional follow-ups at age 25 years and age 30 years or 31 years. Early AFD in family (OR 2.39: 95% CI 1.10 to 5.20) and other contexts (OR 5.75: 95% CI 1.53 to 21.54) were associated with lifetime problem drinking by age 31 years in a model adjusting for various characteristics of the first drinking episode as well as gender, socioeconomic status and religion. However, neither AFD nor context of first drink was a statistically significant predictor of alcohol problems in a multivariate model adjusting also for other risk factors (regression coefficient: −0.0631, p>0.05). The strongest predictor of adult alcohol problems was whether one felt drunk at first episode and this was highly significant in all analyses, including the multivariable model with the most rigorous adjustment for confounders (regression coefficient: 0.3848, p<0.0001).
Guttmannova et al20 investigated possible effects on adult alcohol misuse and dependence (whether any within 12 months prior to interview and for how many follow-up waves) of AFD and the initiation of regular drinking among a sample of 808 people who had initiated drinking prior to the US legal age of 21 years. For analysis purposes AFD was categorised into four age ranges, less than 11 years old, 11–14 years old, 15–17 years old and 18–20 years old. Data on alcohol-related outcomes were collected at 3-yearly intervals from age 21 years to age 33 years. The authors found no association between AFD and alcohol misuse. While AFD was not related to the occurrence of any diagnosis of dependence to age 33 years, it was associated with the number of interviews for which a past year diagnosis was applicable, with AFD before 11 years being at elevated risk compared with ages 11–14 years in a model controlling for demographic and other adolescent substance use variables (OR 1.68, p<0.05). The authors were particularly interested in evaluating a sensitive period hypothesis, that vulnerability was greater if AFD occurred between ages 11 years and 14 years, and found no evidence to support this. Although AFD itself was not generally associated with adult alcohol problems, the authors found that initiation of regular drinking between 15 years to 17 years of age was consistently associated with alcohol misuse and dependence.
A later report by this group evaluated the finding of an association of AFD with chronicity of dependence in a subset of 706 people in the same cohort in greater detail after splitting the exposure into AFD before age 11 years or not.21 This study extension was principally concerned to test three competing hypotheses for the association between AFD and chronicity of dependence using mediation analyses in structural equation regression models. These hypotheses related to: confounding by other risk factors (the marker hypothesis, see later); developmental impairment leading to greater involvement with alcohol; and increased adolescent substance use. None of these hypotheses were supported.21
In a study of 1311 people, Rossow and Kuntsche22 used a binary measure of whether participants reported alcohol consumption by age 13–14 years as their exposure variable, based on questions about the most recent drinking occasion. Participants were followed up once at age 26–27 years to measure adult alcohol consumption patterns. At follow-up, AFD by age 13 years or 14 years was associated with frequent intoxication (OR 1.5: 95% CI 1.2 to 1.9) and high Alcohol Use Disorders Identification Test (AUDIT) scores (OR 1.6: 95%CI 1.3 to 2.1) in models adjusting only for gender. When the authors also adjusted for conduct problems in adolescence, these ORs attenuated and were no longer statistically significant (OR for frequent intoxication, 1.2: 95% CI 0.9 to 1.6, OR for high AUDIT scores, 1.2: 95% CI 0.9 to 1.6). The authors identify these findings as coherent with findings from studies with other designs which suggest that delaying AFD will not reduce alcohol problems in adulthood.22
Discussion
The most important study finding is the meagre evidence base available, with only a small number of heterogeneous studies providing an insecure basis for making conclusions on the relationship between AFD and adult alcohol problems. There is some evidence of at least small, rather inconsistent, effects of AFD on adult alcohol problems in all studies, however these effects attenuate or disappear with more rigorous control for confounding. The included studies are not without limitations which are important to consider before drawing conclusions.
Attrition does not generally present a significant threat of bias as follow-up rates were in excess of 80% in all studies. Perhaps of greater relevance were the various forms of selection employed in sample construction, particularly for the smaller studies, which mean that generalisability of findings must be carefully considered. The definition of the exposure, AFD, among included studies is robust, with studies excluded if this was problematic.23 ,24 Similarly outcome measurement is reliable, generally making use of validated measures, and where there are minor deviations from Diagnostic and Statistical Manual of Mental Disorders, for example in timeframes used, these are well justified.
Most studies used a rigorous approach to AFD measurement by collecting data on this variable at multiple points during adolescence, and taking the first report of alcohol use in their analysis.18–21 Confounding is most extensively controlled for by Warner and White19 with reasonable levels of control also employed by Guttmannova et al20 ,21 and to a lesser extent by Rossow and Kuntsche.22 The possibility of overadjustment should be borne in mind, where for example peer variables may lie on the causal pathway to adult outcomes as well as being implicated in earlier AFD.
As with any systematic review of observational studies, we may have missed studies meeting inclusion criteria if the AFD or outcome data were not prominently reported. We examined all studies included in a related systematic review,16 and went to great lengths in identifying further studies through subject experts. If there is significant publication bias and included studies represent a biased sample of all studies that have been undertaken, then overestimation of associations will have occurred. Given the somewhat contested nature of alcohol and drugs issues, this area seems highly vulnerable to publication bias.25 ,26 This possibility seems likely to occur where preliminary explorations of cohort study datasets are deemed to yield no interesting findings.16 It is striking that there were no reports drawn from birth cohort studies and we judge that the possibility of publication bias poses a profound threat to the certainty with which any inferences can be made on this subject.
Other limitations of this small literature should also be borne in mind. There are no included studies from low income and middle income countries, or from any country with a Mediterranean culture. The consequences of earlier AFD should be expected to vary cross-culturally, as early socialisation processes may promote or inhibit learning behavioural control, and alcohol harms are also managed in different ways in different cultures.
Study findings are broadly consistent with the results of a prospective case-control study of children of alcoholics, which was not included in the review and found that earlier AFD was unrelated to alcohol dependence when confounding factors were taken into account.27 A similar pattern of results was seen in two studies based on the very large (more than 40 000 participants) National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) cohort, representative of the population of the USA.28 ,29 These were excluded from the present review by virtue of the absence of AFD measurement in adolescence and are thus vulnerable to recall and related biases. Both found small effects of AFD on adult outcomes.
The finding of a weak or absent association between AFD and later alcohol problems, after observed associations are attenuated with rigorous control for confounders, provides some support for a marker hypothesis.8 Put simply, those who possess an underlying vulnerability to alcohol problems may also be likely to start drinking early. Further support for the marker hypothesis may be inferred from the lack of strong evidence for the long-term effectiveness of interventions which aim to reduce alcohol related harm by preventing underage drinking.12 ,30 ,31 These reviews suggest that delaying AFD does not impact on long-term problems. The most recent findings by Guttmannova et al21 rejecting a marker hypothesis should, however, be borne in mind.
Among the studies that were included, larger and arguably more important effects on the risk of adult alcohol problems were observed in relation to feeling drunk during the first episode and the initiation of regular drinking than AFD itself.19 ,20 These variables representing more significant involvement in alcohol use, or lying a little further along a putative causal pathway, and showing more noteworthy effects, are important to consider carefully. AFD may represent an important event in the acquisition of this new behaviour, whose effects are much more likely to be felt on proximal rather than distal outcomes.16 ,32 ,33 The characteristics of the first event, such as were studied by Warner and White, and other early drinking episodes should be fruitful to explore.34
Despite the challenges involved in interpreting the detail of study findings, the sparse data available carry implications for policy makers. There is no strong evidence for delaying AFD as a means of preventing future adult alcohol problems. However, because alcohol is an important cause of car crashes, violence and suicide, the leading causes of death among adolescents and young people globally,35 there remains a clear rationale for interventions seeking to help young people avoid or better manage alcohol consumption, regardless of whether earlier AFD is a causal component in the aetiology of adult alcohol problems. Decision making in relation to prevention should thus be based on the acute and short-term harms associated with drinking among children and adolescents rather than on uncertain long-term harms.
The most important implication, however, of the findings of this study is the need to develop a very underdeveloped literature in order to support evidence-based prevention practice. Apart from the early study by Pedersen and Skrondal with weak control for confounding,18 the existence of effects of AFD on adult drinking and related problems is supported, but not at all strongly in the first study by Guttmannova et al.20 The opposite possibility is supported by the second study from that cohort, and those by Rossow and Kuntsche and Warner and White.19 ,21 ,22 This rather mixed evidence available from the aforementioned studies, and also the strong likelihood of publication bias indicates the need for caution in making inferences about any such effects. The most sensible conclusions are that we do not yet know whether starting drinking earlier leads to adult alcohol problems and that we need to develop our understanding of drinking behaviour, across the life course and across the globe.
What is already known on this subject
-
A proposed relationship between an early onset of drinking and alcohol problems in adulthood has been used as an important rationale to justify efforts to prevent drinking among children and young people. Although a number of observational studies appear to support this relationship, the evidence for such a link has not previously been systematically examined.
What this study adds
-
There is a meagre evidence-base of high-quality cohort studies to evaluate the relationship between an earlier onset of drinking and adult alcohol problems. These studies do not provide clear evidence of a causal relationship. Policy makers should concentrate on minimising the acute and short-term harms associated with drinking among children and adolescents rather than on uncertain long-term harms.
Acknowledgments
The authors are grateful to David Batty for comments on a draft of this paper.
References
Footnotes
-
Contributors WM: conceptualised and designed the study, carried out data collection and analysis, wrote the first draft of the manuscript and approved the final manuscript as submitted. JM conceptualised and designed the study, carried out data collection and analysis, revised the manuscript and approved the final manuscript as submitted.
-
Funding The work of the second author was supported by a Wellcome Trust Research Career Development Fellowship in Basic Biomedical Science (WT086516MA).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.