Article Text

Abstract
This essay argues that work, and the socioeconomic class polarities it creates, plays a fundamental role in determining inequalities in the distribution of morbidity and mortality. This is by means of uneven exposure to physical hazards and psychosocial risks in the workplace, as well as by inequalities in exclusion from the labour market and the absence of paid work. Furthermore, this essay shows that the relationships between work, worklessness and health inequalities are influenced by the broader political and economic context in the form of welfare state regimes. This leads to the development of a model of the political economy of health inequalities, and how different types of public policy interventions can mitigate these relationships. This model is then applied to the case of work and worklessness. The essay concludes by arguing that politics matters in the aetiology of health inequalities.
- Political issues
- public health policy
- social epidemiology
- social inequalities
Statistics from Altmetric.com
Political economy (the study of the political and economic spheres) has a long, if often subdued, history in the study of health inequalities. Engels1 was arguably the first to analyse public health in this way in his study of the conditions of the working class in Manchester. More recent examples include the work of Doyal and Pennell,2 Coburn3 and the large body of work developed over a number of years by Navarro and colleagues.4 More recently, the political nature of health has been declared ‘public health's biggest idea’,5 and a number of articles have been written that consider how politics influences health and health inequalities.6–8 Reference has also been made to a subdiscipline termed ‘political epidemiology’.9 Even the popular work on equality and health by Wilkinson and Pickett,10 although not explicitly drawing on the political economy or political epidemiology traditions, is clearly influenced by them in that a lot of emphasis is placed on the influence of macro, as opposed to merely meso or micro, level economic and political factors.
The importance of political and economic systems for population health and health inequalities has been shown in various empirical cross-national studies. For example, Navarro and colleagues11 found that different political traditions and the dominant ideologies of governing parties impacted on infant mortality rates and, to a lesser degree, on life expectancy at birth. Western countries with longer periods in which more redistributive political parties held power for longer time periods (such as the Social Democratic-dominated Nordic governments) tended to have better health outcomes than those with more neo-liberal governments. This finding was also supported by work by Chung and Muntaneer.12 Social Democratic governments implement more universal policies that reduce infant and old age mortality, as shown in the comparative study of different pension and child support policies in continental and Nordic countries by Lundberg and colleagues.13 Likewise, the research of Wilkinson and Pickett10 has comprehensively shown that smaller income inequalities, as found in countries with a long history of redistributive governments, result in better population health outcomes. In terms of socioeconomic inequalities in health, relative inequalities in health do not appear to be smallest in more redistributive countries, but the absolute health of all social classes is better.14–16 Furthermore, the systematic review by Beckfield and Krieger7 of 45 studies of politics and health outcomes concluded that neoliberal policies and economic restructuring increased health inequalities.
This essay applies the political economy approach to the study of the contribution of work and worklessness in the development of health inequalities. The essay argues that work, and the socioeconomic class polarities it creates, plays a fundamental role in determining inequalities in the distribution of morbidity and mortality. This is by means of uneven exposure to physical hazards and psychosocial risks in the workplace, as well as by inequalities in exclusion from the labour market and the absence of paid work—worklessness. Furthermore, this essay draws on recent research to show that the relationships between work, worklessness and health inequalities are influenced by the broader political and economic context—‘welfare state regimes’.17 Work (paid wage labour) and worklessness (lack of paid work) are not the discreet activities of individuals, but are essential parts of the way in which the totality of society is politically, socially and economically organised. Work-based hierarchies are reflected to greater or lesser extents in wider societal hierarchies, and socioeconomic class is determined largely by occupation and work-related income. The health effects of work and worklessness also exist within the broader political and economic structures of society. Welfare state capitalism sets the parameters for the social determinants of health, and the way in which the state distributes financial resources and welfare services has consequences for social and economic hierarchies. The welfare state mediates the impact of the social determinants of health and also of socioeconomic class on health. The welfare state thus plays an active role in constituting work and working conditions, as well as the level of worklessness and the extent to which a certain standard of living can be maintained regardless of labour market performance—decommodification.18 This leads to the development of a model of the political economy of health inequalities, and how different types of public policy interventions can mitigate these relationships. This model is then applied to the case of work and worklessness. The essay concludes by arguing that politics matters in the aetiology of health inequalities.
Work and health inequalities
Physical work environment and health inequalities
Low occupation jobs are more exposed to adverse physical working conditions. European Working Conditions Survey data shows that professionals have at least 50% less exposure to the major physical hazards (exposure to dangerous chemicals, noise, vibrations, repetitive work, shift work and heavy lifting) than the bottom occupational groups.19 Industries with a high percentage of workers in lower socioeconomic classes (such as construction or manufacturing) are also those at elevated risk of occupational injuries and accidents, restricted posture, repetitive movements and heavy lifting.20 Often workers' exposures to such risk are multiple. The health problems associated with the adverse aspects of the physical work environment are more prevalent among manual than non-manual workers. For example, industrial injury rates in the UK exhibit significant occupational inequalities, with professional occupations having a fatal injury rate of 0.2 per 100 000 compared with a rate of 1.9 per 100 000 for the lowest grade occupations.21 Similarly, the all reported injury rate for professionals was 188.6 per 100 000, as opposed to 1725.1 for the lowest workers.21 Lower occupations are also more likely to develop ill health after exposure to hazards. For example, in the case of lead exposure, poor nutritional conditions such as irregular food intake, high fat intake and deficiencies in calcium and iron augment the physiological effects of lead uptake.22
Psychosocial work environment and health inequalities
The distribution of adverse psychosocial working conditions is also socially patterned, with jobs at the lower end of the socioeconomic class scale more likely to entail a higher exposure to adverse conditions than those towards the higher end. European Working Conditions Survey data shows that in terms of social support at work, there are few differences by occupation, with the lowest occupational groups and the highest occupational groups reporting broadly similar levels of social support.19 However, in terms of job demands (repetition, tight deadlines, machine paced, monotonous) and control at work (control over tasks or speed of tasks, consulted about changes), there are stark differences by occupational status between the highest and lowest occupations. For example, in terms of demands at work, monotonous work was approximately 50% higher among the lowest occupational groups. Similarly, workers in the two highest occupational groups were almost twice as likely to report that they were consulted about changes to the organisation of work as those in the two lowest occupational groups.19 The Whitehall studies have demonstrated that occupational class differences in the psychosocial work environment are important in terms of explaining the social gradient in health, with adjustment for adverse psychosocial working conditions reducing the inequality in coronary heart disease between the top and bottom occupational grades by 64% in men and 51% in women.23 Differences in psychosocial working conditions are also linked to inequalities in the distribution and development of musculoskeletal disease.24 Similarly, socioeconomic inequalities in psychological disorders are also strongly associated with inequalities in exposures to harmful psychosocial work environments.25
Worklessness and health inequalities
Unemployment, health and health inequalities
Unemployment is associated with poverty and social exclusion, and it tends to be concentrated in lower socioeconomic classes: employment rates are consistently higher among more educated groups.26 For example, according to English Census data, in 2001 in London 90.1% of men and 81.5% of women with a university degree were employed compared with just 69.2% of men and 51.8% of women with no qualifications.27 Ill health-related job loss also has a social gradient, with adverse employment consequences more likely for those in lower socioeconomic classes.28 The importance of unemployment to health inequalities was demonstrated in a recent English study, which found that for both men and women, not being in paid employment accounted for up to 81% of the inequalities in the prevalence of self-rated poor health between the most affluent and the least affluent socioeconomic classes in the English working age population.27 As an example, 5.6% of men living in owner-occupied housing did not have good general health compared with 19.1% of men in social rented housing, an age-adjusted difference of 13% points. After further adjustment for employment status this difference reduced to 2.5% points, a reduction of 81%. Adjusting for employment status reduced the prevalence of poor self-reported health in all socioeconomic classes, thereby substantially reducing the social gradient.27
Inequalities in health-related worklessness
Ill health increases the likelihood of long-term worklessness. For example, a study of health-related worklessness in the UK using national household survey data found that the employment rates of people with a chronic illness or disability were 45.9% compared to 82.4% of those without an illness or disability.29 However, the worklessness associated with ill health (health-related worklessness) is also significantly unevenly socioeconomically and spatially distributed. A comprehensive comparative study found that there were significant educational inequalities in the employment rates of people with a limiting long-term illness.30 In the UK, the study found that, in 2005, employment rates of men with a low education and ill health were 65.6% less than healthy men with a low education, 58.7% less than highly educated men with ill health and 68.1% lower than healthy, highly educated men. These patterns were even starker for UK women: those with a low education and ill health had employment rates of 71.2% less than healthy women with a low education, 72.6% less than highly educated women with ill health and 79.4% lower than healthy, highly educated women. Internationally, these patterns were repeated to a greater or lesser extent, with the employment gaps between healthy highly educated men and low educated men with ill health ranging from 30.9% in Norway to 68.1% in the UK, and between healthy highly educated women and low educated women with ill health ranging from 57.7% in Sweden to 79.4% in the UK.30 Similarly, the geographical distribution of health-related worklessness is also skewed, with levels highest in the deprived de-industrialised areas (eg, the north east of England, the west of Scotland and South Wales) and smallest in the more affluent, mainly semi-rural non-deprived commuter and ‘stock-broker’ belt areas (eg, in the south east region of England).31
Public policy and the political economy of health
Work, worklessness and welfare state regimes
‘Welfare state regimes’ is a term used to refer collectively to the different political and economic arrangements of particular types of welfare state capitalism.32 Following comparative social policy research, advanced welfare states can be divided into at least four different types: Social Democratic (Nordic countries); Conservative (continental Europe); Liberal (English-speaking countries) and southern (Mediterranean European countries) (for an overview see Bambra, 2007).32 International research on the social determinants of health has increasingly examined how population health and health inequalities vary by welfare state regime type. These studies have invariably concluded that health is better in the more egalitarian Social Democratic welfare states.33
Research into the work environment, unemployment and health-related worklessness also suggests important variation by welfare state regime. In terms of the work environment, although there is little variation across advanced welfare states in terms of the influence of the physical work environment (although the Liberal welfare states are the least regulatory) on health outcomes,34 studies have shown important variation in the psychosocial work environment, work-related stress and the health effects of adverse psychosocial working conditions.35 For example, the relationship between job insecurity and poor health is less in those countries with more extensive social security systems, which improve the ability of individuals to cope with stressful events.36 Similarly, recent epidemiological work has shown that relationships between stressful psychosocial work environments and health differ by welfare state regime, with a lower prevalence of work-related stress in Social Democratic countries that have more comprehensive welfare states and where the psychosocial work environment is more regulated.20 37 38 These studies have also found that the effects on health and health inequalities of adverse psychosocial work environments are lessened in these countries.37 38
Social protection (particularly wage replacement rates) during unemployment varies by welfare state regime. A recent study examined the extent to which relative health inequalities between unemployed and employed people varied across European welfare state regimes.39 It found that in all countries, the relative health of the unemployed was consistently worse than that of those in work, and that these relative inequalities were largest for both men and women in the Liberal welfare states where benefit levels were lowest and where means-testing was more common. Similarly, in respect of health-related worklessness, recent studies have shown that the employment rates of people with an illness vary by welfare state regime.30 40 Health-related worklessness is lowest in the Social Democratic welfare states, where the worklessness rates of people with a chronic illness is less than 40%, and it is highest in the Liberal countries where it is over 50%.40 Socioeconomic inequalities in the employment consequences of ill health are also higher in the Liberal welfare states than in the Social Democratic states.30 40
Framework of the political economy of health inequalities
The effects of work and worklessness on health and health inequalities are therefore mediated by political, economic and social organisations—by welfare state regime. Drawing on this, figure 1 sets out a conceptual framework for understanding how socioeconomic class inequalities in health are a result of interactions between the political and economic systems, the state, the social security system, the labour market and the organisation of work. In this framework, political power relations and the economic system set the landscape and the structural parameters within which the social determinants of health operate.6 Politics is given prominence in the model both as an overarching macro actor, which has the ability to shape and reshape all the determinants (including the economic system), and also as an important factor working across the macro, meso and micro levels, contextualising the various intervention points (A–C). The (welfare) state is given a quasi-independent role in which it mediates the effects of the economic system, as well as the organisation of work and the labour market, on the extent of socioeconomic class inequality and on exposure to the social determinants of health (such as the work environment).
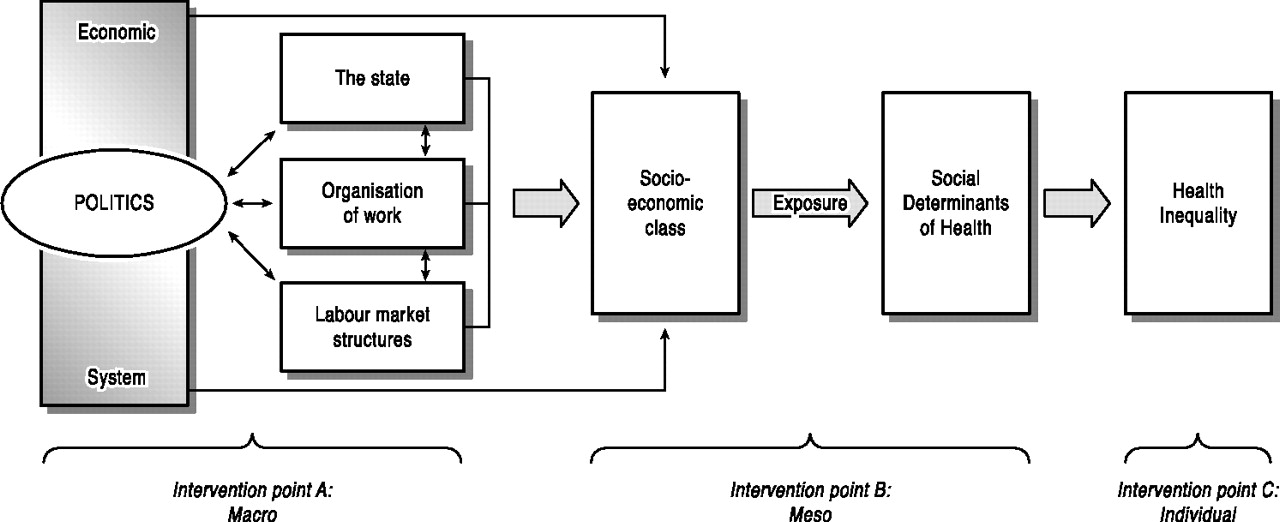
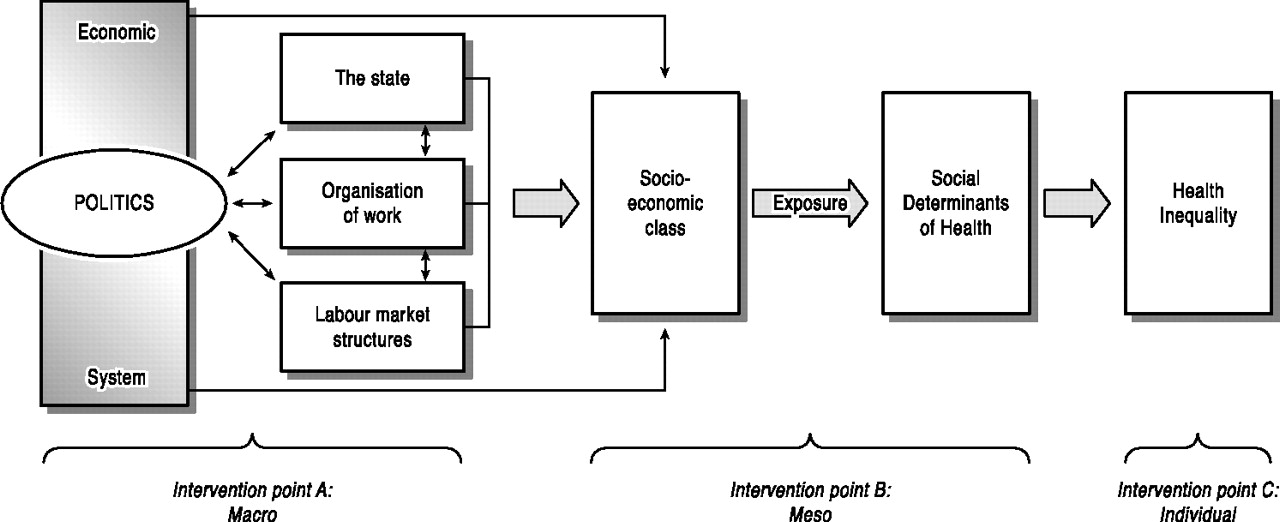{kind=link}
A model of the political economy of health inequalities.
The intervention points (A–C) can be understood in the following ways: intervention point A includes macro-level changes to the political and economic context (the economy, the state, the organisation of work, the social security system or the labour market); point B refers to meso-level environmental changes to the social determinants (such as housing or the work environment); and interventions at point C focus on the individual and ‘treating’ the structural effects of inequality. A and B can thus be considered as primary and secondary prevention intervention points, whereas point C is effectively the treatment point. Interventions at point A are expected to be the most beneficial in terms of reducing health inequalities and those at point C the least. Interventions at points A and B treat the causes, whereas interventions at point C treat the symptoms.
Work, health and welfare policy interventions
In terms of specific work, health and welfare policy interventions, the minimum income for healthy living proposed by Morris and colleagues41 is an example of a macro primary prevention policy intervention. The minimum income for healthy living is a way of ensuring that social security benefits and wages are of a sufficient level to maintain health and wellbeing (a living wage), and that there is a right to a certain standard of living for all citizens (a citizen's income) regardless of their employment status. Based on the link between income and health, Morris and colleagues41 have illustrated how health can be improved and inequalities in health reduced by the public provision of a minimum income to meet basic and social needs relating to nutrition, physical activity, housing, psychosocial interactions, transport, medical care and hygiene. The 2010 Marmot Review recommended implementation of the minimum income for healthy living, and it is also supported as a policy to tackle health inequalities by the WHO.42 43 Less specific examples would include improving job security, making wages more equitable and increasing income equality (either at source as is the case in Japan or through the tax system as is the case in Sweden), or reducing the unemployment rate (by public employment for example).10 44
Changes to the physical and psychosocial work environments can be considered as secondary prevention measures. Health and safety legislation to reduce exposure to the adverse aspects of the physical work environment, such as the 1975 Health and Safety at Work Act in the UK or the 1970 Occupational Safety and Health Act in the USA, are examples of secondary prevention. However, while regulations exist, for them to be effective they need to be well implemented and enforced.20 45 In terms of the psychosocial work environment, systematic review evidence suggests that organisational changes that increase workers' control and participation improve occupational health.46–48 In 1994 the European Union issued a directive to increase participation at work, and countries such as Sweden and Norway have implemented extensive regulation of the psychosocial work environment in order to prevent occupational ill health.49 50
In terms of ‘treatment’ interventions, most measures to improve the health of the workless, or enhance the employment of the chronically ill, would come under this category as they are dealing with existing inequality and ill health. For example, many interventions intended to increase the employment rates of people with a disability or chronic illness are supply-side focused and thus target the individual (in terms of skills, job searching, interview skills—employability) rather than trying to increase demand from employers or alter the structural barriers that people may face in terms of, say, workplace design or working hours.51 Other examples of individual focused interventions to reduce health inequalities would include workplace strategies to help workers cope better with workplace stress or with the desynchronisation of shift work.44 46 52
Conclusion
This short essay has drawn on epidemiological research to show the importance of work and worklessness in the development of health inequalities. It has also shown that the health effects of work and worklessness vary by welfare state regime and that politics matters: how society is economically and socially organised is vital in terms of influencing the social determinants of health and health inequalities.53 This political economy analysis also shows that, even within the constraints of unequal capitalist societies, things can be done to improve health and reduce health inequalities. A model of the political economy of health inequalities has been proposed and applied to the case of work and worklessness. It has shown that interventions that increase income, eradicate or reduce exposure to known hazards in the workplace, or include health concerns in the planning of production, can improve population health and, given the uneven socioeconomic distribution of work-related ill health, thereby decrease health inequalities.54
What is already known on this subject
Political economy — the study of the political and economic spheres — has a long, if often subdued, history in the study of health inequalities. In general, recent political economy research has focused on the macro level relationships between political ideologies, welfare state regimes and population health outcomes.
What this study adds
This essay instead applies the political economy approach to the study of the contribution of specific social determinants — work and worklessness — to the development of socio-economic health inequalities. It summarises research in this area and develops a model of the political economy of health inequalities which is used to identify possible labour market and work environment intervention points. Examples of interventions in relation to work and worklessness are also provided.
Policy implications
Policy interventions can be made at the macro, meso or individual level requiring primary prevention, secondary prevention and treatment interventions respectively. In terms of work, health and welfare policy interventions, the minimum income for healthy living is an example of a macro level primary prevention intervention; changes to the physical and psychosocial work environments (such as health and safety legislation or measures which increase worker's control) can be considered as secondary prevention measures, whilst individual focused interventions to reduce health inequalities include work place strategies to help workers cope better with work place stress, and supply-side interventions intended to increase the employment rates of people with a disability or chronic illness.
Acknowledgments
The ideas outlined in this essay are explored in more detail in Bambra.17
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.