Article Text

Abstract
Background The relationship between unemployment and poor health has been well established. Unemployment causes poor health, and poor health increases the probability of unemployment.
Methods A prospective study with 6 months' follow-up was conducted among unemployed participants receiving social security benefits who were capable of full-time employment and were referred to a re-employment training centre. Re-employment was defined as ending social security benefits for at least 3 months because of starting with paid employment. Health-related quality of life was measured by the 36-Item Short-Form Health Survey. A Cox proportional hazards analysis was used to determine the factors that predicted re-employment during follow-up. The influence of re-employment on changes in perceived health was investigated with linear regression analysis.
Results Unemployed participants with a poor health at baseline were less likely to return to paid employment during follow-up. Almost all dimensions of health at baseline had an influence on the likelihood of becoming employed. Among the re-employed participants, general health, physical functioning, social functioning, vitality, mental health, bodily pain and role limitations due to emotional or physical problems improved, with an effect size varying from 0.11 to 0.66.
Conclusions This study provides evidence that re-employment leads to improvement of self-perceived health within a short time window. This suggests that labour force participation should be considered as therapeutic intervention within health promotion programmes among unemployed persons.
- Self-rated health
- unemployment
- unemployment and health
Statistics from Altmetric.com
The relationship between unemployment and poor health has been well established, as demonstrated by a higher prevalence of illness and disability1 2 and a higher mortality among unemployed people.3 The association between health and employment is bidirectional: unemployment may cause poor health (causation hypothesis), and poor health may increase the probability of unemployment (selection hypothesis).
There is evidence for the selection hypothesis. A longitudinal study among European countries showed that in most European countries, a perceived poor health or a chronic health problem predicted becoming or staying unemployed.4 A community-based survey in the UK found that health-related job loss had become increasingly common, especially in relation to musculoskeletal disorders and mental illness.5 A 2-year follow-up study of long-term unemployed Norwegians reported that health-related selection to long-term unemployment explained a substantial part of the excess mental morbidity among unemployed people.6
However, there is also evidence for the causation hypothesis. Various studies have shown that unemployment gave rise to health effects, especially psychological distress, depression and reduced mental health. A review of 16 longitudinal studies concerning the mental health effect of unemployment concluded that loss of employment affected mental health but also that gaining employment improved mental health.7 A British longitudinal study found that transitions from paid employment to various forms of non-employment (unemployment, long-term sick leave, and maternity leave) had a negative impact on mental health. Transitions from non-employment to formal employment resulted in an improvement of mental health. The effects were felt most strongly within 6 months after the transition.8 A 5-year follow-up study among long-term unemployed Norwegians reported recovery of mental health after re-employment.9
“Work, matched to one's knowledge and skills and undertaken in a safe, healthy environment, can reverse the harmful effects of prolonged sickness absence or long term unemployment, and promote health, well-being and prosperity”. This is the main message of the so-called Black report, which reviewed the health of Britain's working-age population.10 11 In a review, Waddell and Burton12 concluded that re-employment leads to clear benefits in psychological health and some measures of well-being, although there is a dearth of information on physical health. A meta-analytic study of the psychological and physical well-being during unemployment also demonstrated that the bulk of research is focused on mental health outcomes, suggesting that other aspects of health need more attention.13 One study on re-employment indicated that physical and mental health improved among those working at 1-year follow-up compared with those not working.14 Another study also showed a positive association between gaining employment and physical functioning among older workers who were displaced.15 However, both studies were among older workers who were recently displaced or early retired. It is not known whether these results can be generalised to the whole working age population with a different unemployment history.
The impact of re-employment on mental health is reported by two meta-analytic studies.7 13 There is limited insight into the effect size of re-employment on other dimensions of health.13 The aim of this study was to investigate the effect of re-employment on different dimensions of health within a short period after entering paid employment.
Methods
Study population
A prospective study with 6 months' follow-up was conducted among unemployed participants. The study population consisted of persons on social security benefits who were capable of full-time employment and who were referred by the Employment Centre of the City of Rotterdam, The Netherlands, to one of the four re-employment training centres in the area for a re-employment training. Some of the participants did have chronic health problems but were declared fit enough to be capable of full-time employment after investigation by a physician, a psychologist and an employment specialist. From December 2004 until December 2007, every week, a mean of 19 participants were enrolled in the study after referral to a re-employment training centre. In total, 2754 eligible participants were included in the study. Participation in this study was voluntary. The Medical Ethics Committee of Erasmus MC provided a declaration of no objection.
Data collection
The first questionnaire was sent to prospective participants immediately after the referral to the re-employment training centre. The follow-up questionnaire was sent 6 months later. The procedure of data collection was similar at baseline and follow-up. The first questionnaire was sent to the home address of the participants, followed by two reminders 2 and 4 weeks later. Additional actions were undertaken to include more participants. As a large part of the study population had a non-Dutch background, the questionnaire and the covering letter were translated in Turkish and sent in addition to the Dutch questionnaire to participants with a Turkish surname. If participants of the study population needed help with filling out the questionnaire, they could get in touch with an interviewer. Participants who did not reply to the postal questionnaire were visited by an interviewer at their home address with four attempts at different day times during a 2-week period. The interviewers were matched with the participants based on ethnicity, age and sex and could offer an interview in the mother tongue (Dutch, Arabic or Turkish).
Sociodemographic variables
Sociodemographic variables, such as ethnic background, highest educational level, age, sex and marital status were included in the questionnaire. The ethnic background of the respondent was based on the country of birth of the mother. In case the mother was born in The Netherlands, the country of birth of the father was leading.16 Different ethnic groups were defined based on differences in geographical and cultural distance from The Netherlands. Three ethnic minority groups were defined: (1) Turks and Moroccans, (2) Antilleans and Surinamese and (3) a miscellaneous group with all other countries of origin. The participants were divided into three groups according to their highest level of educational attainment. A high educational level was defined as higher vocational training or university, intermediate educational level was defined as higher secondary schooling or intermediate vocational training and low educational level was defined as no education, primary school, lower and intermediate secondary schooling or lower vocational training. Marital status was used to distinguish from others those participants who were married or living together.
Psychological measures
Mastery was measured by the Personal Mastery Scale,17 which consists of seven items (eg, “I have little control over the things that happen to me”, “There is little I can do to change many of the important things in my life”), answered on a four-point Likert scale (strongly agree to strongly disagree). The mean scores across items were calculated, ranging from 1 to 4, with a higher score indicating a higher level of mastery. In case three or more items were unanswered, no score was computed.
Self-esteem was measured with the Rosenberg Self-Esteem Scale,18 with 10 items (eg, “On the whole, I am satisfied with myself”, “All in all, I am inclined to feel that I am a failure”), answered on a four-point Likert scale (strongly agree to strongly disagree). Mean scores across items were calculated again, ranging from 1 to 4; a higher score indicated a higher level of self-esteem. In case three or more items were unanswered, no score was computed.
Re-employment training
A re-employment training centre provided a standardised approach of a re-employment training, characterised by a broad re-orientation on employment and employability, enhancement of job search skills and intensification of job search efforts.
Re-employment
The start and end dates of the social security benefits were registered at the Employment Centre of the City of Rotterdam, The Netherlands. In these registers, additional information about reasons for ending benefits was also administered. Re-employment was defined as leaving the social security benefit services for at least 3 months because of starting with paid employment, verified by the national social security agency. Participants who quitted their registration for a social security benefit for other reasons—for example, moving in with a partner or moving out of the city of Rotterdam, were censored from the moment that their benefit payment was quitted by the social security services.
Health measures
Health-related quality of life was measured with the Dutch version of the 36-Item Short-Form Health Survey (SF-36).19 20 Self-reported health was measured with the first item of the SF-36 by asking participants to rate their overall health on a five-point scale, ranging from “excellent”, “very good”, “good” and “fair” to “poor”. Those reporting less than “good health” were defined as having a poor health.21
The other 35 items of the SF-36 were used to calculate scores on eight dimensions: physical functioning, general health, mental health, bodily pain, social functioning, vitality, role limitation due to emotional health problems and role limitation due to physical health problems. Scores could range from 0 to 100, with a higher score indicating a better health-related quality of life.
Statistical analysis
All statistical analyses were conducted by means of the statistical package SPSS V.15 for Windows, and the level of significance was set at 0.05.
In the analyses, two groups of respondents were compared: those who were still unemployed at follow-up and those who were re-employed at follow-up. The baseline characteristics of both groups were compared with the χ2 test for dichotomous data and the t test for continuous data. Non-response to the first questionnaire and loss to follow-up during the 6 months until the second questionnaire were investigated by logistic regression analysis with potential determinants: individual characteristics, perceived health, participation in re-employment training and re-employment.
A Cox proportional hazards analysis was used to determine the factors that predicted re-employment during the follow-up period. The follow-up period was censored at the date of re-employment. Independent factors were individual characteristics, self-esteem, mastery and the eight dimensions of the SF-36. The variables were coded in such a manner that a hazards ratio (HR) >1 indicates an increased likelihood of re-entering paid employment. For each dimension of the SF-36, a standardised HR was calculated based on a mean score across items, representing the effect of an increase of 1 SD in the mean score at baseline on the likelihood of entering paid employment. Individual characteristics with a significant univariate effect on re-employment were entered first in the multivariate model. Subsequently, the health measure with the largest goodness of fit in the univariate analysis was entered in the multivariate model. After that, the effect of the other measures of health was investigated for their additional effect on goodness of fit.
The association of re-employment with changes in perceived health was investigated with linear regression analysis. The association of re-employment with each dimension of health was adjusted for age, sex, ethnic background, education, duration on benefit, participation in a re-employment training and also the baseline value of the health dimension under study. For each dimension of health, Cohen's d was calculated as a measure of effect size by dividing the difference in health before and after re-employment by their pooled SD.22
Results
Figure 1 shows that 2754 participants were enrolled in the study after referral to a re-employment training centre. One third (n=932) of the participants had chronic health complaints, but were declared to be fit enough to be capable of full-time employment after investigation by a physician, a psychologist and an employment specialist. From the 2754 participants who received the first questionnaire, 1829 (66%) participants filled out and returned the questionnaire. More than two thirds (70%) of the respondents returned the baseline questionnaire by post, whereas almost one third (30%) of the respondents had a face-to-face interview. Non-response was statistically significantly higher among younger participants and men.
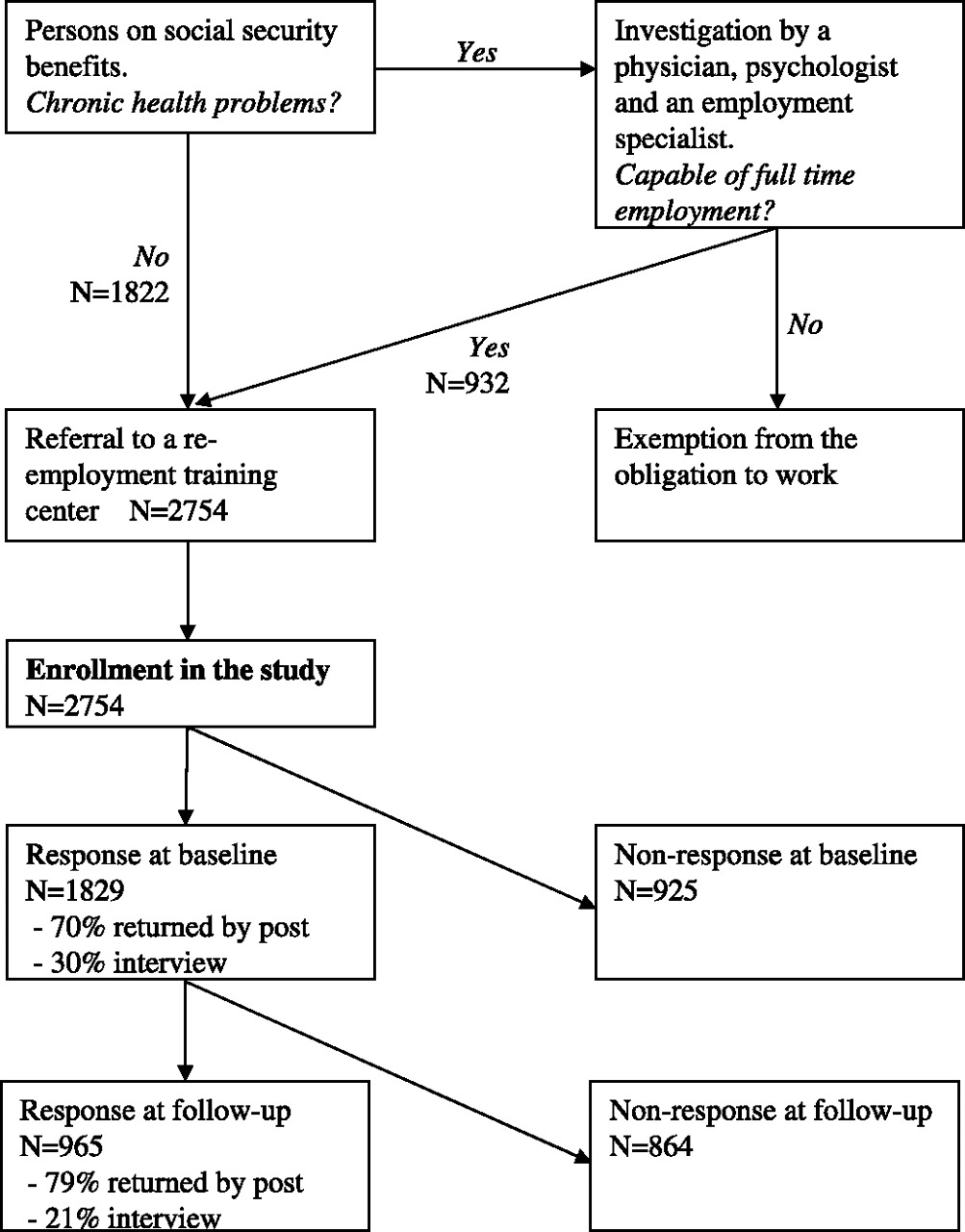
Flow of the participants and response at baseline and follow-up.
The response at follow-up was 53% (965/1829). Loss to follow-up was statistically significantly higher among the younger participants, the men and the participants of non-Dutch origin but not related to marital status, employment history, duration on benefit or health at baseline. The participants who had started with a re-employment training (n=461) were less often lost to follow-up (OR 0.8; 95% confidence interval (CI) 0.7 to 1.0), whereas the participants who had returned to paid employment (n=123) were more often lost to follow-up (OR 1.9, 95% CI 1.3 to 2.7). However, among those who returned to paid employment, health at baseline did not differ significantly between non-respondents (n=76) and respondents (n=47) at follow-up.
Table 1 shows the characteristics of the respondents to the first questionnaire. The mean (SD) age of the respondents was 39.7 (9.5) years, 49% were man, 57% had a low level of education, 75% belonged to an ethnic minority group and 43% received social security benefits for >5 years. During the follow-up period, 30% of the respondents had started with a re-employment training.
Characteristics of respondents to the first questionnaire (n=1829)
Figure 2 shows that health at baseline was better among the participants who returned to paid employment during the follow-up period. All the dimensions of health improved among the re-employed participants, whereas the health status of the unemployed participants remained unchanged.

{kind=link}
{kind=link}
Health at baseline and follow-up for the participants who continued to be unemployed (n=918) and the participants who re-entered paid employment (n=47) during the follow-up period of 6 months.
Table 2 shows that the unemployed participants with a poor health at baseline were less likely to return to paid employment during follow-up (OR 0.39, 95% CI 0.2 to 0.7). All the dimensions of perceived health at baseline had an influence on the likelihood of becoming employed, except for mental health. Physical functioning had the strongest influence on the likelihood of becoming employed (OR 2.76, 95% CI 1.8 to 4.3). Ethnic background, marital status, self-esteem, mastery and participating in a re-employment training were not significant in the univariate model.
The influence of individual characteristics and dimensions of self-perceived health among long-term unemployed persons (n=965) on the likelihood of re-employment (n=47) during a follow-up period of 6 months (Cox proportional hazards analysis)
In the multivariate analysis, physical functioning at baseline had the strongest association with re-employment. Because of the correlations of the other health measures with physical health (general health, r=0.56; bodily pain, r=0.62; mental health, r=0.26; social functioning, r=0.43; vitality, r=0.41; role functioning: emotional, r=0.27 and physical, r=0.55), these measures of health did not have a significant contribution to the multivariate model including physical functioning.
Table 3 shows that among the re-employed participants, general health, physical functioning, social functioning, vitality, mental health, bodily pain and role limitations due to emotional or physical problems improved during the follow-up period, with an effect size varying from 0.11 to 0.66. The largest relative improvements were observed for mental health, social functioning and role limitations due to emotional or physical problems, whereas physical functioning showed the smallest relative improvement. For those participants who remained unemployed, the effect sizes varied from −0.04 to 0.06, indicating that their health status remained virtually unchanged during the 6 months' follow-up period. Participation in a re-employment training was not associated with change of health status (data not shown).
The influence of re-employment on the changes in the eight dimensions of health measured by the SF-36 health questionnaire among the long-term unemployed persons during a follow-up period of 6 months
Discussion
Unemployed participants with a poor health at baseline were less likely to return to paid employment during follow-up. Almost all the dimensions of health at baseline had an influence on the likelihood of becoming employed. The strongest association was found between physical functioning at baseline and re-employment. Among the re-employed participants, general health, physical functioning, social functioning, vitality, mental health, bodily pain and role limitations due to emotional or physical problems improved, with an effect size varying from 0.11 to 0.66. Hence, re-employment positively influenced mental health and physical health.
Loss to follow-up was significantly higher among the younger participants, the men, the participants of non-Dutch origin and the participants who had returned to paid employment. However, among those who found employment (n=123), health at baseline did not differ between non-respondents (n=76) and respondents (n=47) at follow-up. Therefore, we assume that the effects of re-employment on health were not influenced by selective loss to follow-up.
The participants who were referred to a re-employment training centre were included in the study. The policy of the Employment Centre of the City of Rotterdam was to refer everybody who was able to work and could use some help with searching for a job. Hence, the participants were not included in the study when they were not able (owing to health problems) or not obliged (owing to family obligations or education) to work. In addition, recently unemployed persons who were supposed to be able to find paid employment by themselves were not included. This may have affected the results with respect to health status and re-employment probabilities.
The re-employed workers got their jobs at different times during the follow-up period of the study. Therefore, some persons may have been back at work for much longer than others; thus, the length of exposure to the health benefits of re-employment varied among the re-employed sample. Unfortunately, because of the small number of persons who gained employment, it is not feasible to analyse the relation between time at work and health benefits due to re-employment.
The study is based on self-reported health status. Therefore, justification bias may have influenced the present results. The respondents who were still unemployed at follow-up may have reported more easily that they had a poor health than those who found paid employment to justify the fact that they did not find a job.23
Because of the observational design of the study, the results may have been influenced by selection bias. The participants who found employment differed from those who stayed unemployed with respect to health at baseline and personal characteristics. These variables were adjusted for in the analysis, but there may have been other variables that influenced both health change and re-employment—for example, motivation to work, that were not included in the analysis. However, two psychological measures that were included in the study, self esteem and mastery, did not have a significant influence on the likelihood of re-employment. In addition, these psychological measures did not influence the estimated effects of re-employment on health.
To control for the systematic differences in health at baseline between the unemployed and re-employed participants, stratified analyses were conducted, showing that re-employment resulted in an increase of health for both the participants with a poor health at baseline and the participants with a good health at baseline. In general, the participants with a poor health at baseline showed a larger increase in health after re-employment than the participants with a good health at baseline (data not shown). However, after finding paid employment, the health status of recently re-employed participants still lagged the health status of long-term employed persons.24
The unemployed participants with a good health were more likely to return to paid employment during follow-up. Therefore, the results of this study support the selection hypothesis. These findings are in accordance with a study of the European Community Household Panel, which found that a poor health or chronic health problem predicted staying or becoming unemployed in European countries.4 A 2-year follow-up study of the long-term unemployed in Norway showed that health-related selection to long-term unemployment explained a substantial part of the excess mental morbidity among unemployed people.6
This study also showed that the health status of re-employed participants improved, whereas the health status of unemployed participants remained unchanged. Re-employment did not only have a positive influence on mental health but also on physical functioning, which was in accordance with findings from two other studies.14 15 Based on these findings, it seems most likely that starting with paid employment results in health improvement. However, because of the design of the study, it cannot be ruled out that it is the other way around; a change in health status may increase the likelihood of finding paid employment. However, a review showed that an increase in health status of the long-term unemployed is rather unlikely.2 Therefore, it is assumed that the health status of the participants increased shortly after re-employment, supporting the causation hypothesis. This is in congruence with findings from other studies, which found an increase in mental health status after re-employment.8 9
In the present study, an effect size of 0.66 was found for the improvement of mental health after re-employment. This result is in accordance with findings from two meta-analytic studies7 13 reporting that gaining employment impacts on mental health with an effect size of 0.54 and 0.89. The effects on other dimensions were slightly lower, but because different dimensions of health were associated with each other, it is difficult to infer that mental health seems more important than physical health. This is in accordance with the results of the Whitehall II study of civil servants, which showed that physical and mental health were correlated for participants with a low socioeconomic position.25
In the current study, only 5% (47/965) of the participants found paid employment within 6 months. This low re-employment rate is in accordance with a study among persons receiving social security benefits in the city of Amsterdam, The Netherlands, which showed that only 8% of the persons found paid employment in a 2-year period from 2004 to 2006.26 The current study, population is characterised by a long-term unemployment history. The long-term unemployed participants often have much difficulty in finding paid employment, especially for those with a poor health. All the participants in the study were referred to a re-employment training centre for a re-employment training. However, this re-employment training did not have a positive effect on the probability of re-employment or on the health status of the participants. Therefore, other measures seem to be required to increase the chance of re-employment for the long-term unemployed with a poor health.
In the recent Black report on the health of the British working age population, Black appealed for changing perceptions of fitness for work. Instead of sticking to the idea that one cannot work unless 100% fit, it is recommended that a campaign should be launched to make employers, healthcare professionals and the general public aware that work is in general good for health.10 This study provides evidence that work is indeed good for your health; thus, work should be considered as an important part of health promotion programmes among unemployed persons. In policies for health equity, public health measures are required to include persons with a poor health in the labour market and to prevent workers with ill health from dropping out of the workforce.
What is already known on this subject
The relationship between unemployment and poor health has been well established.
Unemployment may cause poor health, and poor health may increase the probability of unemployment.
What this study adds
Among re-employed persons, general health, physical functioning, bodily pain, mental health, social functioning, vitality and role limitations due to emotional or physical problems improved, with an effect size varying from 0.11 to 0.66.
Re-employment leads to improvement of self-perceived health within a short time window.
Socioeconomic inequalities in health can be reduced by increasing labour participation.
References
Footnotes
Funding This study received support from the Public Health Fund (Fonds OGZ), Laan van Nieuw Oost Indie 334, 2593 CE Den Haag, The Netherlands.
Competing interests None.
Ethics approval This study was conducted with the approval of the medical ethics committee of the University Medical Center Rotterdam, Erasmus MC, Rotterdam, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.