Article Text

Abstract
Objective: To analyse trends in mortality inequalities by educational level for main causes of death among men and women in Barcelona, Spain, at the turn of the 21st century (1992–2003).
Methods: The population of reference was all Barcelona residents older than 19 years. All deaths between 1992–2003 were included. Educational level was obtained through record linkage between the mortality register and the municipal census of Barcelona city. Variables studied were age, sex, educational level, period of death (four periods of 3 years) and cause of death. Age-standardised mortality rates for each educational level, sex and period were calculated. Poisson regression models were fitted to obtain relative index of inequality (RII) for educational level, adjusted for age for the time-periods.
Results: RII for all causes of death was constant (around 1.5), but rate differences were higher in 1995–7 (715.6 per 100 000 in men and 352.8 in women) than in other periods and tended to decrease in men over the periods. Analysis of inequality trends by specific causes of death shows a stable trend for the majority of causes, with higher mortality among those with less education for all causes of death except lung cancer and breast cancer among women having RII below 1.
Conclusions: Relative inequalities in total mortality by sex in Barcelona did not change during the 12 years studied, whereas absolute inequalities tended to decrease in men. Our study fills an important gap in southern Europe and Spanish literature on trends during this period.
Statistics from Altmetric.com
Trends in mortality inequalities by socioeconomic position during the 1990s have been studied in many countries, the majority of them having found an increase in health inequalities.1–7 In northern European countries, this increase is mainly the result of the faster proportional cardiovascular mortality decline in advantaged socioeconomic groups, whereas in southern European settings other causes of death seem to play a more important role.1 In countries from eastern Europe, the social disruption and increase in economic inequalities brought about by a rapid transition to a market economy appear to be the main determinants,4 the transition being more favourable for those with the greatest educational resources.6 7
In Spain, individually based studies are few, owing to the absence or poor quality of information on socioeconomic characteristics given in death certificates, together with a more restrictive legislation regarding the use of individual data than in most northern and central European countries.8–12 The majority of research on trends in mortality inequalities has been conducted using ecological or mixed designs,13 using individuals with geocoded socioeconomic data of their area of residence,14 15 or using individual data from working age (or employed) men in eight selected Spanish provinces (out of 50 Spanish provinces) where the occupation given in death certificates is most complete.16 17 The majority of these studies found an increase in mortality inequalities over the period studied. However, there are no trend studies based on individual data and international trend studies have not included Spain.1
In the city of Barcelona, the record linkage between the mortality register and the local census since 1992 permits the study of mortality inequalities by socioeconomic position at the individual level. Such data availability gives us an opportunity to fill this important gap in the literature on mortality trends in Spain. Therefore, the objective of our study was to analyse trends in mortality inequalities by educational level for the main causes of death among men and women in Barcelona at the turn of the 21st century (1992–2003).
METHODS
Design and study population
Barcelona, the second largest city in Spain (1 643 542 inhabitants in 1991 and 1 586 604 in 2004), is located on the north eastern coast of the Iberian Peninsula. We used a trend design using individual data. The population studied was all Barcelona residents older than 19 years of age. All deaths in the mortality register, which occurred among these residents between 1992 and 2003 and which had complete educational level information, were included (n = 183 018). The educational level of the deceased was obtained through record linkage between the mortality register and the municipal census of Barcelona (92.76% of cases were linked), the remaining deaths were excluded (n = 14 286). This is a confidential probabilistic linkage based on the name, the surname and the date of birth of the deceased.18 The underlying causes of death were coded using the International Classification of Diseases (ICD) 9th revision until 1999 and ICD-10 after 1999. We included the main causes of death and of premature mortality (see table 1).
Information on the population at risk, including age, sex and the highest completed level of education came from the Barcelona 1991, 1996 and 2003 municipal censuses, an administrative register not subject to statistical secrecy; we did not have data on the census by educational level for other years. Every resident in Barcelona is registered in the municipal census. This census is continually updated to incorporate data on migration, births and deaths. For the years between the three censuses an estimate of the intercensal population was obtained based on a geometric curve.19
Variables and indicators analysed
The variables studied were age, sex, education (highest level of education completed), year of death and cause of death.
Age of death was grouped in 14 five-year age-groups (20–24 years, 25–29 years, etc). Educational level was categorised in five groups: (a) no education: illiterate or people who only had 0–4 years of schooling, (b) elementary or primary education not completed: people with uncompleted elementary education (5–6 years of schooling); (c) primary education: people with complete primary education (7–9 years of schooling); (d) secondary education (10–14 years of studies), and (e) university education (15 years or more of schooling). To fit Poisson regression models, the years of death were grouped into four of three-year periods: 1992–4, 1995–7, 1998–2000, 2001–3 in order to have sufficient numbers of deaths in each period. The causes of death selected are listed in table 1 with their corresponding ICD-9 and ICD-10 codes.
Data analysis
All the analyses were performed separately for men and women because the relation between mortality and educational level may differ between men and women for several causes of death.20 Age-standardised mortality rates for each year and period of three years, standardised through the direct method, were estimated using the 1996 population of Barcelona as the reference population. Rate differences between the rates of the lowest and highest educational level were obtained for the four time periods.
Poisson regression models21 were fitted to obtain the relative index of inequality (RII) and its 95% confidence interval (95% CI) for educational level, adjusted for age for the four time periods. The dependent variable was the logarithm of the mortality rate, and the independent variables were educational level as a quantitative variable (with five values between 0 and 1, which reflect the educational level distribution in the population in each period) and age group. The RII can be interpreted as the ratio of mortality rates between the two extremes of the educational spectrum.22
In order to know whether the RII changed in the different periods, all deaths from all periods were pooled together and Poisson regression models were fitted with educational level, period and age as independent variables, as well as the interaction between educational level and period. If this interaction was statistically significant at the 5% level, the RII were considered to be different.
RESULTS
Table 2 shows the distribution of mortality by causes of death and educational level for each period and also the population at risk. The main causes of death were cardiovascular diseases among women and cancer among men. More than 60% of deaths of men and 80% of deaths of women corresponded to people with less than primary education.
The percentage of the population with no education was higher for women than for men and it decreased during the time periods. Conversely, the population with higher education increased over the 12 year period.
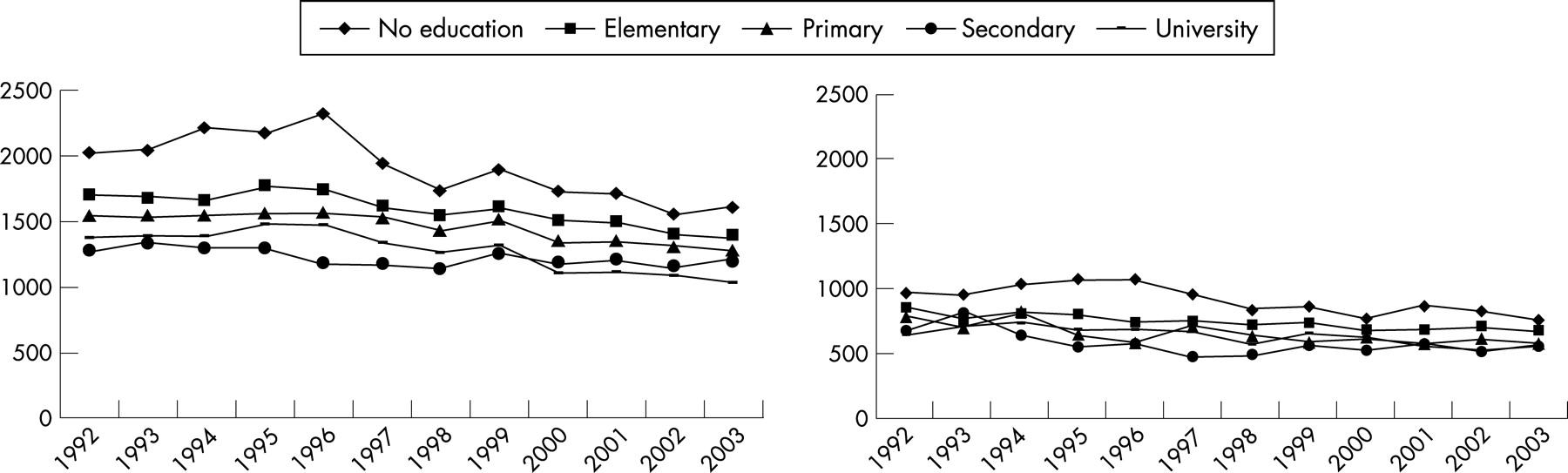
RII and rate differences by causes of death are presented in table 3 for men and women. RII for all causes of death was constant over the years (around 1.5 with no statistically significant differences between periods, p = 0.19 in men and p = 0.37 in women), but rate differences were higher in the 1995–7 period (715.6 per 100 000 population in men and 352.8 per 100 000 population in women) than in other periods and tended to decrease in men. This pattern can also be observed in figure 1 where the evolution of age-standardised death rates over the 12 years is presented by educational level.
The analysis of inequality trends by specific causes of death shows that for the majority of causes there is a stable trend with higher mortality among those with less education for all causes of death except lung cancer and breast cancer among women who have RII below 1 (for breast cancer the 95% CI includes 1).
For major causes of death (that is, cardiovascular diseases and cancer), the RII are higher than 1. RII of cardiovascular diseases is higher for women than for men although rate differences are similar (fig 2). Although statistically non-significant, inequalities tended to increase for ischaemic heart disease and decrease for cerebrovascular disease.

For cancer mortality, RII and rate differences among educational levels are more important among men, with a stable trend in both sexes. Figure 2 also shows this pattern. Among men, for specific causes of cancer, the highest RII corresponds to stomach and lung cancer, while the highest rate differences correspond to lung cancer, owing to the higher rates of mortality of this cancer. Among women, the majority of RII of specific causes of cancer are not different from 1 and the rate differences are very low. It is worth mentioning that the RII was below 1 (with 95% CI that does not include 1) for lung cancer in the last three periods.
Respiratory diseases show a stable trend, the RII and rate differences being higher among men (RII higher than 2 and rate differences higher than 100 per 100 000 inhabitants) than among women. Endocrinal diseases show a stable pattern with highest RII among women. Cirrhosis has RII higher than 2 among men and higher than 3 among women, the rate differences decreasing mainly in men (53.6 per 100 000 inhabitants in 1992–4 and 18.3 in 2001–3).
AIDS mortality is the cause of death that has changed the most during the period studied (fig 3) showing an increase in all educational levels up until 1995 and after this a decrease. This is reflected mainly in the large rate differences in the 1995–7 period (rate difference = 133.9 per 100 000 inhabitants in men and 43.6 per 100 000 in women). Infectious diseases also show similar changes over the years.

{kind=link}
{kind=link}
{kind=link}
Traffic injuries inequalities tend to decrease in men (p = 0.06) but not in women. Drug overdose shows the highest RII, mainly among men, tending to decrease, and also decreasing rate differences, due to the decreasing of rates in all groups (fig 3). Injury mortality relative inequalities increased among women (RII = 1.36, 95% CI:0.97 to 1.92 in the first period and RII = 2.27, 95% CI:1.70 to 3.04 in the last period) (table 3).
DISCUSSION
This study has provided evidence on the evolution of educational level inequalities in mortality in a southern European setting at the turn of the 21st century. As reviewed in the introduction there is lack of data on individual level trend inequalities in southern Europe and in Spain in particular. In previous articles only data from the city of Turin (Italy) were available.1 This is an important point since time-trend patterns on mortality inequalities across European countries may be different, and this may provide clues to identify the main causes of health inequalities.
A key finding of our study is that relative inequalities in total mortality by sex did not change during the 12 years studied, whereas absolute inequalities tended to decrease in men. The major causes of death (that is, cardiovascular, cancer and respiratory diseases) also had a stable trend in relative terms and a decrease in absolute differences among men. Inequalities for digestive diseases tended to decrease. The main changes during this period were found for AIDS and injury mortality (among females).
Although it is difficult to compare the size of educational level inequalities in mortality, the results found in this study are not different from those obtained in previous studies from western European countries.22–24 The RII for total mortality were slightly smaller for women than for men, whereas the rate differences were higher for men. This may arise because causes of death for which inequalities in mortality are large have fewer deaths among women, such as AIDS, drug overdose, cirrhosis, etc. In addition, women present fewer inequalities for some causes of death such as cancer.
It is worth mentioning that southern European countries such as Spain, are among the countries with the highest AIDS rates in Europe,25 mainly as a result of AIDS acquired by drug users through sharing of drug-injection paraphernalia. Moreover, AIDS was the main cause of death among young adults during the 1990s26 and drug overdose the second,27 and these causes of death present high socioeconomic inequalities.28 29
The absence of an increase in inequalities in mortality in Barcelona in these 12 years contrasts with the results found in other studies where widening inequalities are found.1–4 6 7 10 14 16 30–32 Several factors can have influenced these results. Firstly, universal access to health services articulated in the 1986 General Health Bill facilitates access to health services for all the population.33 Secondly, after recovering democracy in the mid 1970s, the field of public health has been a priority of the Barcelona administration. The annual health report evolved in its scope, presenting comparisons by municipal districts and neighbourhoods, which led to the identification of territorial inequalities in health, which in turn pointed to issues to be tackled by health policies or interventions that were partially evaluated.34 The worsening of various social and economic factors during the 1990s such as temporary employment (especially among young people and women) or the strong increase in the cost of housing and of renting a house, with their ensuing deprivation, may not yet have had an impact on mortality indicators.
Among adult men, many of the causes of death (cancer, cardiovascular, respiratory diseases) are related to tobacco consumption, which is higher among men in more deprived social classes.35 Lung cancer mortality is higher in men with less education, and the trends are stable through the periods. Among women, attention should be drawn to the positive associations (more mortality among the highest educational levels) of lung cancer, a pattern that does not change over the years, because the rates increase for all educational levels. It should be noted that currently in Barcelona it is still the women in privileged social classes who smoke most and mainly the oldest ones, a fact which parallels the situation in both Spain as a whole and in other southern European countries.36 Findings on smoking support the conclusions by Lynch et al,37 whereby one cannot make universal predictions with regard to social class inequalities in health. Relative and absolute differences seem to depend on socio-historical factors (for example, gender attitudes) that shape the distribution of risk factors (for example, exposure to tobacco) in different socioeconomic classes.
It has been previously described that breast cancer is more common in women of higher socioeconomic groups, mainly due to reproductive factors,38 but in our study trends were stable, with a small positive association. A French study on time trends (1968–96) found that this positive association progressively weakened and no association remained in the 1990s, although it disappeared earlier among younger women.39 The authors comment that factors related to differential changes in reproductive behaviours (having fewer children), cancer prevention and cancer survival among educational levels can explain the results. Similar processes might be affecting Catalan women during the period considered. It is worth mentioning that a screening programme of breast cancer has existed in the city of Barcelona since the mid 1990s and was implemented first in one of the poorest districts of the city.40
Trends in cardiovascular mortality inequalities found in Barcelona are similar to those described by Avendaño et al41 for several European countries, in the sense that cerebrovascular inequalities are stable, while ischaemic heart disease inequalities are increasing. However, these results differ from a study done in Spain including active men from eight provinces, where an increase of inequalities between 1980 and 1990 was described.16 In Barcelona, cerebrovascular mortality decreased at all educational levels, and this fact may be related to the quality improvement of primary health services. These services have been reformed in Spain since the 1980s in order to offer a more longitudinal and comprehensive care, implying better quality. One of the changes of this reform has been the implementation of preventive practices, including the control and treatment of hypertension, itself a consequence of egalitarian local policies. In Barcelona this reform started in the poorest neighbourhoods, a fact that can also be related to the trends found.42 43
With regard to AIDS, in a previous study we examined whether AIDS mortality before and after the introduction of highly active antiretroviral therapy (HAART) had increased or decreased differentially by socioeconomic group in Barcelona. We found that although AIDS mortality evolved differently for different socioeconomic groups (both increasing and decreasing more in lower socioeconomic groups), the pattern of AIDS mortality inequalities by socioeconomic group remained stable, in the sense that more deprived socioeconomic groups had higher mortality than their wealthier counterparts. In addition, inequalities did not narrow after the introduction of HAART, possibly suggesting the existence of problems of access, or adherence, to HAART among persons in low socioeconomic groups.44 Another study described inequalities in AIDS mortality in terms of educational level and community-level variables using a multilevel approach. Apart from individual educational level, the area deprivation also had an effect. This community-level effect could be related to the marginalisation of the population in those deprived areas, implying that apart from educational level, other factors related to poverty and living conditions are important.28
The pattern of drug overdose mortality and inequalities tends to decrease. Probably the intervention programmes addressed to this group of people play a role.45 These programmes were designed to assist drug users, dealing not only with specific health problems (infectious disease, mental health, etc) but also with practical needs (housing, food, etc). Moreover, the harm reduction programmes include active case-finding and treatment of organic problems (such as tuberculosis), methadone maintenance programmes,46 syringe exchange, outreach programmes and legal and occupational support.
These programmes have a clear redistributive effect, as drug users tend to benefit more from them, thus reducing inequalities.
Limitations
One of the limitations of the study is the presence of missing values for the educational level indicator. They were higher in the first period (11.0% of deaths in men and 11.8% in women) than in other periods (4.3% in men and 5.5% in women in the last period). We do not think that these missing values are related to educational level and for this reason they do not affect the RII, but rate differences may be slightly underestimated in the first period. Missing data on educational level are mainly related to the fact that the death occurred outside the city, because the linkage to the census is more difficult.
Another limitation is the measure of the socioeconomic position used (educational level) because we did not have the occupation, income or social class of the deceased. Several limitations of educational level are: firstly, its inability to refer to social groups arising from interdependent economic relations; secondly, it is less predictive than class position of ownership of capital assets; and, thirdly, it does not have a universal meaning because its implications are related to age, gender, race, birth cohort and class position.47
Conclusions and recommendations
Contrary to the widening of socioeconomic inequalities found in other European settings, in Barcelona, relative inequalities in total mortality by sex did not change during the 12 years studied, whereas absolute inequalities tended to decrease in men.
Our study fills an important gap in southern Europe and Spanish literature on trends during the 1990s and early 2000s. As Spain joined the core of wealthy countries in the EU during that period its profile of health inequalities is consistent overall with findings from other EU countries. In addition, local policies in Barcelona seem to have a distinct effect on the local reduction of mortality inequalities. A direct evaluation of local programmes with the potential to reduce mortality inequalities (for example, targeting drug users) will be necessary to confirm these suggestions.
What this paper adds
Trends in mortality inequalities by socioeconomic position during the 1990s have been studied in many countries, the majority of them having found an increase in these inequalities. In Spain, there are no trend studies based on individual data and international trend studies do not include Spain.
Contrary to studies done in other countries, relative inequalities in total mortality by sex in Barcelona did not change during the 12 years studied, whereas absolute inequalities tended to decrease in men. Our study fills an important gap in southern Europe and Spanish literature on trends during the 1990s and early 2000s.
Policy implications
Policies on health inequalities must be included in the political and policy agenda because tackling health inequalities will improve the health of the whole population as well as decrease socioeconomic inequalities. A direct evaluation of local programmes with the potential to reduce mortality inequalities (for example, targeting drug users) must be implemented.
Acknowledgments
This study was partially financed by the grant number 04/2013 of the Fondo de Investigaciones Sanitarias and by the Red de Centros de Epidemiología y Salud Pública (C03/09).
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- In this issue