Article Text

Abstract
Economic and social resources are known to contribute to the unequal distribution of health outcomes. Culture-related factors such as normative beliefs, knowledge and behaviours have also been shown to be associated with health status. The role and function of cultural resources in the unequal distribution of health is addressed. Drawing on the work of French Sociologist Pierre Bourdieu, the concept of cultural capital for its contribution to the current understanding of social inequalities in health is explored. It is suggested that class related cultural resources interact with economic and social capital in the social structuring of people’s health chances and choices. It is concluded that cultural capital is a key element in the behavioural transformation of social inequality into health inequality. New directions for empirical research on the interplay between economic, social and cultural capital are outlined.
Statistics from Altmetric.com
Material as well as non-material resources have been found to be associated with population health and risk of disease.1–4 Studies on such resources that are typically connected to an individual’s social position, namely financial means and interpersonal support, often draw on theories of capital. Measures of economic and social capital have been used successfully in health research.5–8 Today, income, as a key indicator of economic capital, continues to be associated with health and risk of disease.9 10 Also, social capital, measured for instance through membership in support-providing networks, has been shown to be associated with health outcomes.11–13 Recently, however, empirical studies have appeared linking health inequality to cultural capital,14 15 and have argued that culture-based activities, knowledge and perceptions present a unique form of health-relevant capital. However, the contribution of those studies to the current discourse in social epidemiology remains limited for two reasons. First, they lack a specific definition of health-relevant cultural capital. Yet, such a definition appears mandatory for meaningful measurement of cultural capital in empirical studies on health inequalities. Second, regarding the multidimensional effects of social inequality,2 4 most studies attempt to filter out the unique contribution of culture-based factors by statistical adjustment for education or income. Those approaches can, however, be criticised for neglect of the more complex interactions between cultural, social and economic capital. In an attempt to close this gap, the present paper starts with a short summary of the findings from recent studies addressing the associations between cultural resources and health inequalities. Drawing on Pierre Bourdieu’s original notion of cultural capital,16 17 I then lay out those properties and functions of cultural capital that are instrumental in specifically addressing health inequalities. The paper adds to the emerging literature on cultural capital a theoretically derived definition of health-relevant cultural capital and illustrates the role of capital interaction in the social reproduction of health inequalities.
CULTURAL CAPITAL IN HEALTH RESEARCH
The general term “capital” refers to resources generated by labour. Cultural capital can be broadly defined as people’s symbolic and informational resources for action.18 Those resources (eg values, behavioural norms and knowledge) are acquired mostly through social learning, with learning conditions varying across the social classes, status groups or milieus.19
The concept of cultural capital has gained increasing attention in the social sciences19 20 with applications in health research recently emerging. Veenstra21 exploring relations between social space, social class and health inequalities used measures of economic, social and cultural capital. Familiarity with various sport figures, artists, novelists and books, and magazines were included in correspondence analyses as indicators of cultural capital. Linking cultural, social and economic capital variables he was able to identify distinct social spaces within which different health indicators could be situated. To study the direct effects of cultural capital on health outcomes, Khawaja and Mowafi15 examined associations between cultural capital and psychosocial health. They found that participation in cultural activities (ie reading books, volunteering for cultural events) was—net of the effects of socioeconomic status (SES) and social capital—a powerful predictor of self-perceived health among Lebanese women living in poor urban communities. Malat14 discussed the role of cultural capital (eg patients’ beliefs about their care, perceptions of physicians’ behaviours) in racial disparities in medical treatment, suggesting that “… non-whites are more likely to have a need to activate cultural capital” (p 310) to secure better treatment outcomes. In a particular medical setting, namely treatment of allergic contact dermatitis, Noiesen et al22 studied the resources needed by patients to understand medical advice and to adopt appropriate behaviours. From their findings they concluded that cultural resources such as the capacity for active information seeking and critical consumer behaviour contributed significantly to the explanation of social class differences in patients’ behaviour. In earlier research, a number of studies looked at participation in cultural events and culture-oriented leisure activities.23–25 Results from those studies suggest that participation in cultural activities is associated with lower mortality risk and perceived health.
Overall, the findings from these studies indicate that culture-based resources may play a significant role in the unequal distribution of health. Yet, a closer look reveals some methodological weaknesses and theoretical shortcomings. For instance, the relevance and validity of indicators such as “hours of TV consumption”15 or “frequency of theatre visits”25 as meaningful indicators of cultural capital needs to be critically discussed. Moreover, indicators such as participation in—often costly—cultural events or TV consumption in poor countries may both be highly related to peoples’ social class position and thus their economic resources and social relations. Those associations pose challenging questions and make it necessary to explain the genuine meaning of cultural capital beyond the well-known effects of economic and social resources on health. Moreover, the associations between specific cultural resources and economic and social capital clearly warrant further clarification.
CULTURAL CAPITAL: ITS PROPERTIES AND FUNCTIONS RELATING TO HEALTH INEQUALITIES
Cultural capital refers to the operational skills, linguistic styles, values and norms that one accrues through education and life-long socialisation.17 20 It comprises people’s social abilities and competence for action, including their perceptions, values, norms, cognitive and operational skills.16 26 Cultural capital emerges in three different forms: incorporated (e.g. values, skills, knowledge), objectivised (eg books, tools) and institutionalised (eg educational degrees, professional titles) cultural capital.17
Applied to health research, Bourdieu’s general notion of cultural capital can be used to define health-relevant cultural capital as comprising all culture-based resources that are available to people for acting in favour of their health. In its incorporated form it comprises health-related values, behavioural norms, knowledge and operational skills. For instance, health literacy—a resource for health-promoting behaviours that is known to be unequally distributed across educational classes27 28—can be explained as part of people’s incorporated cultural capital. Also, behavioural norms and preferences that were linked to health in the studies mentioned above can be explained as incorporated cultural capital. For example, associations between attendance of cultural events and survival outcomes23 may partly be because those cultural activities are part of distinct and often healthier lifestyles. Moreover, cultural activities may promote feelings of belonging or activate other health resources such as social support. Effects related to social distinction may also help to explain associations between TV consumption and subjective health in a Lebanese urban setting, as observed by Khawaja and Mowafi.15 In social cultural contexts where possession of a TV set is a privilege of the “well off”, TV consumption may promote psychological well-being and increase individuals’ subjective health.
Health books and internet access (as sources of health knowledge) or recreational equipment (eg for physical activity) represent examples of objectivised cultural capital closely linked to health and health-promoting behaviour. Outdoor exercise equipment is a good example of objectivised cultural capital and its functional and symbolic use: as Veenstra21 observes, cycling to work—in his study of Canadians in British Columbia a typical middle-class lifestyle behaviour—is not only associated with better health status through physiological processes activated by the functional use of the bicycle. Objectivised cultural capital (the helmet, the back pack, the rain gear) may also “…induce social distance in every day interaction by providing subtle messages to members of other classes to ‘keep their distance’ and ‘stay in their place”.[21, p.30] Thus, depending on a particular social cultural context the use of these objects (bicycles and their “accessories”) may serve both: physical health and subjective well-being through physiological effects and social distinction.
In the present paper I focus on incorporated cultural capital as it is in this form that cultural capital becomes a key component that links people’s social position with the behavioural aspects of health inequality (for a separate discussion of objectivised and institutionalised cultural capital in health promotion see Abel).29
Incorporated cultural capital becomes directly relevant to health through distinct lifestyle patterns.21 Definitions of health-relevant lifestyles have focused on collective patterns of health behaviours and orientations.30 31 Health lifestyle patterns are developed by groups of individuals according to the material and non-material resources available to them.32 Cultural capital in the form of health values, perceptions, health knowledge and behavioural norms provides the non-material resources needed to develop healthy lifestyle patterns and deal effectively with health issues on an everyday basis. The fact that the acquisition of cultural capital depends on the social class-specific learning context19 20 explains why the health resources that emerge from it are also unequally distributed across the social classes. In that sense cultural capital—expressed and effective through collective lifestyles—is not only a determinant of individual health, but also a crucial component in the social reproduction of health inequalities through social class-specific health lifestyles.21 33
CULTURAL CAPITAL: INTERACTIONS AND TRANSFORMATIONS RELEVANT TO HEALTH
The interplay between the different forms of capital can be understood as a basic principle operating in the processes that lead to social distinction, inequality and the reproduction of social class.34 Economic, social and cultural resources are correlated and feed on each other (see fig 1).

The different forms of capital can be converted as it is, for example, the case when personal income (economic capital) is used for advanced education (cultural capital). Interactions can also include intergenerational transmission of capitals. For instance, parents invest their financial resources in their children’s higher education. Their children’s higher educational status may later not only lead them to better paid jobs, but also be instrumental in acquiring social capital, for example by increasing their chances for membership in powerful networks. The basic principle of capital conversion can also be applied to issues of health inequalities. It suggests that cultural, social and economic capital affect people’s health through distinct patterns of interactions.
Cultural resources affect the use of economic capital for health!
Economic capital provides people with options, many of which are relevant to their health: paying for medical services or insurance plans, being able to afford to live in a health-promoting, supportive and safe neighbourhood or having the money to buy healthy, yet often more expensive food. These are but three examples of how financial resources determine people’s range of health-enhancing options. However, for people when operating within a given economic frame of options, cultural resources come into play. This is the case, for example when health-related values and norms, perceptions and knowledge guide people’s health lifestyle choices.35 36 Whereas the range of choices for health-relevant consumer goods is dependent on financial means, cultural capital is of particular importance for using those financial resources for specific healthy choices. Nutritional behaviour and patterns of physical activity may be referred to as two respective examples: values attached to health, knowledge about health effects of certain food products and norms that guide health behaviours are all cultural resources that structure people’s preferences and choices, including their eating and physical activity habits.
Economic capital approaches often fall short of elucidating the social differences observed in those health behaviours that cannot be explained by financial determination: unhealthy patterns of consumption such as smoking, excessive eating or drinking or sedentary lifestyles are in large parts more determined by people’s norms and values than by insufficient financial means. Income explanations alone provide no convincing answers to questions on how unhealthy lifestyles have become normative in different groups, milieus and social classes. Referring to the above examples, it appears reasonable to argue that cultural capital in the form of values, perceptions, knowledge and behavioural norms is instrumental in the use of economic resources for health gains.
Cultural resources affect social capital for health!
Social capital provides people with access to interpersonal support systems that may, among other benefits, be helpful in matters of personal health and community health action.37 38 To acquire social capital, to sustain and use it successfully, other resources are needed. Financial investments in the form of entrance fees or costs of socializing may be mandatory in some cases, for example for membership in support groups and clubs. However, beyond monetary resources, certain behaviours and value orientations are expected from all those who want to belong to social capital-providing networks.39 40 Sharing similar values, knowing how to approach other members properly, the ability to use appropriate language and communication styles are examples of non-material conditions and cultural techniques required for people to enter those networks.
Once a member, cultural resources may also facilitate an individual’s use of social capital for health gains. In the form of shared values and operational skills cultural capital provides the means to actively participate in and benefit from social capital networks that offer interpersonal support in health matters. What this suggests is that particular cultural resources are mandatory in the acquisition and instrumental in the use of health-effective social capital.
Economic and social resources affect cultural capital for health!
People’s chances to acquire health-effective cultural capital increase with the availability of other types of capital. Economic capital may be required, for instance, to participate in activities that encourage or re-enforce health choices such as health promotion events or sports club programmes. Money is often needed to gain access to particular learning facilities and programmes. Examples may range from buying health books to attending health promotion classes or paying for personal health internet tools or services. Social capital, on the other hand, can also increase people’s chances to accumulate health-relevant cultural capital, for instance through informal access to health information, expert knowledge and advice. Memberships in networks or social groups such as patient’s organisations, neighbourhood initiatives and self-help groups have been found to improve health knowledge.41 42 Thus the acquisition of health-relevant cultural capital is in major parts directly dependent on the availability of other types of resources, namely economic and social capital.
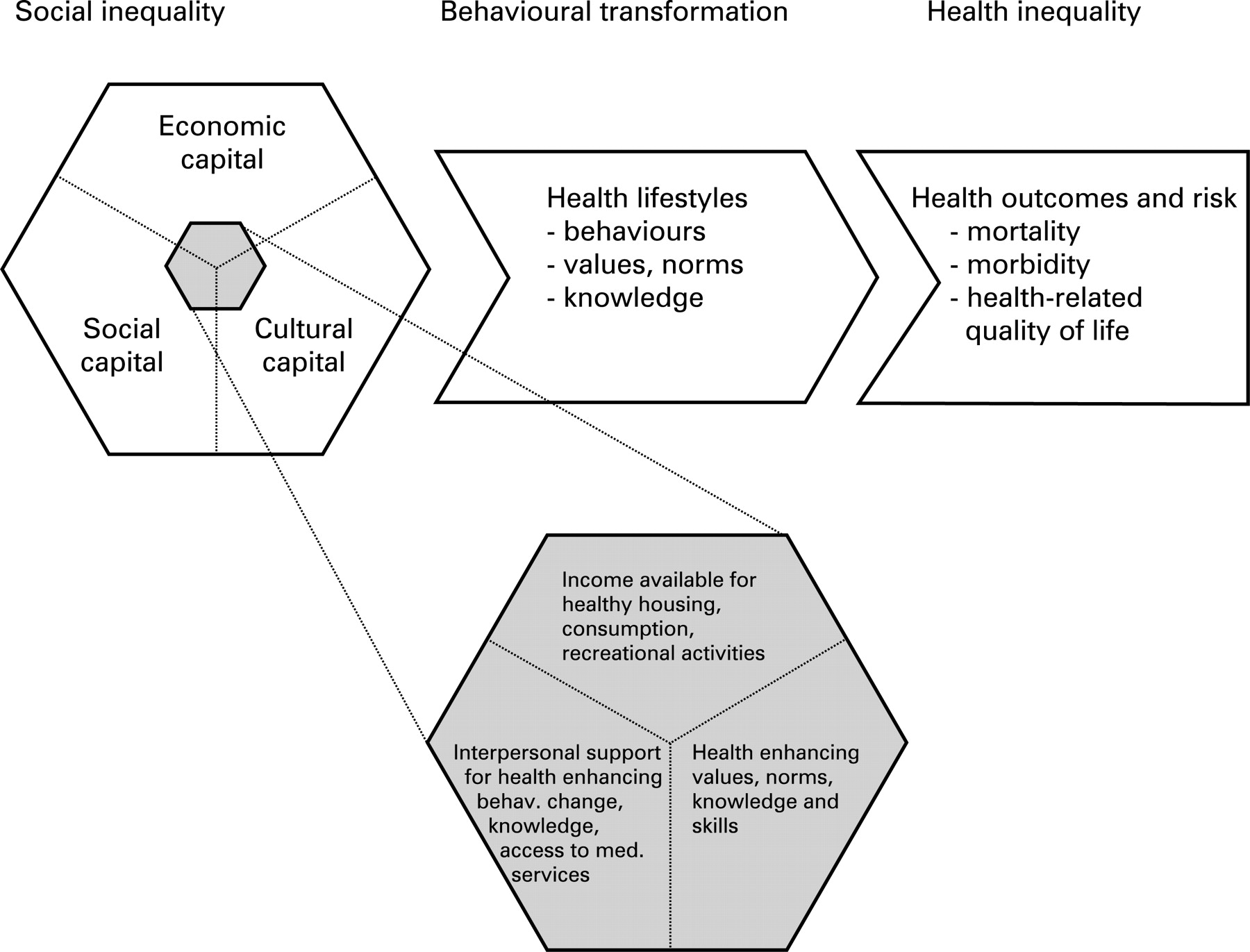
Figure 2 provides a visualisation of the links between social inequality and health inequality focussing on behavioural transformations through collective lifestyle patterns. Relationships between health-related lifestyles and peoples’ social class or status have been described earlier.30 32 35 36 43 Those authors have argued that the chances to realise a health-promoting lifestyle are closely tied to people’s social class and status position. The new model presented here goes beyond this general observation by identifying the resources that facilitate health-promoting lifestyles. It provides the grounds to distinguish between health-relevant economic, social and cultural resources and shows their integration within a broader pattern of capitals available. The model suggests focusing on the interplay between the three different forms of health-relevant capital, including measures of cultural capital. Moreover, it draws attention to the fact that the resources needed to select or adopt specific health-relevant lifestyles emerge from the interplay between economic, social and cultural capital. In this dynamic form social inequalities affect—through collective behavioural variations—people’s health status and risks.

{kind=link}
{kind=link}
CONCLUSIONS
How can we explain the relationship between material and non-material resources for health? The present paper has addressed this question by focusing on cultural capital and its interdependencies with economic and social capital. Health-relevant cultural capital has been defined as the culture-based resources that are available to people for maintaining and promoting their health. Health values and norms, health knowledge and operational skills have been identified as key elements of health-relevant cultural capital. The possession of that form of capital gains people health advantages whereas its acquisition and use is tied to the availability of other forms of capital.
By explaining people’s culture-based health resources as parts of their health-relevant capital, this approach places cultural determinants firmly in the discourse of structurally based health inequalities. Cultural capital is considered a non-monetary form of capital that interacts with economic and social capital to constitute people’s health chances and choices. As such, the concept links structural and behavioural determinants of health by explaining how people’s behavioural options and preferences are constrained and structured by their cultural, social and economic resources.31 35 In health inequality research cultural capital explanations can help to elucidate the translation of social disadvantage into poor health.44 It does so by identifying the resources behind the socialization processes that lead to health inequalities.45
The theoretical considerations underlying the present focus on the interaction between the different forms of capital have significant implications for future empirical investigations. Whereas the vast body of evidence on social health inequalities led to concepts of “general susceptibility”46 and “fundamental cause”,47 aetiological explanations seem to require a specification of what particular form of social disadvantage leads to poor health.48 49 For measuring social disadvantage this means that “education, income and occupational class cannot be used interchangeably as indicators of a hypothetical latent social dimension”.50 On those issues the concept of cultural capital provides a theoretically meaningful distinction between three major forms of health-relevant capitals. Moreover, in its attempt to account for the dynamic relations among the different forms of health resources, the present approach suggests to move beyond questions on the relative importance of single social determinants of health, and explore the relational effects among material and non-material health resources. The guiding question for future theoretical and empirical research would then become: how and under what circumstances is the accumulation of and the interaction between cultural, economic and social capital beneficial to health?
To realise the full potential of the cultural capital approach in health inequality research some more work is needed. Extended conceptual work is required to understand and integrate other social factors involved, such as gender and ethnic identity. Through cognitive and social learning processes, incorporated cultural capital is invariably tied to the body of a person.18 Thus biological factors such as genetic dispositions and physical conditions may also need to be considered in models explaining the role of cultural capital in the unequal distribution of health.
Of foremost importance for empirical investigations are the development of valid and reliable indicators of health-relevant cultural capital and the design of appropriate statistical models. Recent attempts to operationalise cultural capital may provide a helpful starting point. Theoretical guidance might be helpful to move beyond the currently available indicators and develop more comprehensive measures. In the present paper I have described health-related values and norms, knowledge and operational skills as key elements of health-relevant cultural capital. Those should next be operationalised and applied as indicators in empirical studies. Future statistical models need to estimate the effects of cultural capital on health outcomes, including interaction effects with other forms of capital. Also, sophisticated multilevel models could be developed that help to identify the social and biological factors that determine people’s chances to acquire health-relevant cultural capital.
What this study adds
This paper provides a theory-based definition of health-relevant cultural capital and identifies health values and norms, knowledge and skills as key elements of health-relevant cultural capital.
A new focus in inequality research is suggested that explains social inequalities in health as resulting from the unequal distribution of economic, social and cultural capital.
Interactions between the three forms of capital are described as key processes in the social reproduction of health inequalities.
Acknowledgments
The author wishes to thank the colleagues who have provided helpful comments on an earlier version of the manuscript.
REFERENCES
Footnotes
Competing interests: None.