Article Text

Abstract
Study objective: To describe gender specific suicide rates associated with partner’s psychiatric disorder, loss of a spouse, or child by suicide or other causes, being a parent, and marital status.
Design: Nested case-control study. Information on causes of death, psychiatric admission, marital status, children, and socioeconomic factors was obtained from routine registers.
Setting: Denmark.
Participants: 9011 people aged 25–60 years who committed suicide; 180 220 age-gender matched controls; 111 172 marital partners; 174 672 children.
Main results: The suicide risk in women whose partner had been first admitted with a psychiatric disorder after 31 December two years earlier was 6.9 (95% CI 3.6 to 13.0), whereas their male counterpart experienced a risk of 3.9 (2.7 to 5.6); p value gender difference = 0.39. Men who had lost their partner by suicide or other causes of death experienced a suicide risk of 46.2 (18.3 to 116.4) and 10.1 (6.5 to 15.8), respectively; the analogous risk among women were about one third: 15.8 (6.6 to 37.4) and 3.3 (1.5 to 7.2), respectively. Child bereavement by suicide or other causes imposed an approximate twofold risk increase in their parents, whereas being a parent was protective in women. Except for widows (1.6, 1.2 to 2.0) and widowers (3.0, 2.3 to 3.9) the suicide risk associated with being separated (2.0, 1.8 to 2.3), divorced (1.8, 1.7 to 2.0), never married (1.4, 1.3 to 1.6), cohabitant (1.2, 1.1 to 1.3) was virtually the same in the two sexes.
Conclusions: The suicide risk is associated with partner psychiatric illness. Conjugal bereavement is particularly indicative of suicide in men, and spousal suicide is particularly indicative of suicide. Child bereavement is associated with parental suicide, while being a parent is protective against suicide in women.
- suicide
- psychiatric illness
- child loss
- marital status
Statistics from Altmetric.com
The importance of familial aggregation of suicides and psychiatric disorders in understanding suicidal behaviour and preventing suicide is well recognised.1–3 Some explanations have been that genetic factors play a part in mediating the transmission of familial suicides and psychiatric illness,4–6 or that the familial clustering could be caused by the effect of shared environmental factors.7 Although these explanations are inseparable in most studies, using information on twins,6 who share genes but also most often upbringing, and adoptees,5 who only inherit their biological parents genes, studies have tried to tease out the contribution of the genetic components. However, specific genes associated with suicide and psychopathologies in almost all psychiatric conditions are yet to be identified.8,9,10,11,12 A previous study13 by the author has suggested that the suicide or mental illness of a spouse imposes an environmental rather than a genetic influence. However, such a link might arise as a spurious association through assortative mating.13,14
Nevertheless, experiencing a spouse or a child dying, or a spouse suffering from a psychiatric disorder are stressful life events. Bereavement studies have confirmed that the mortality is increased in surviving spouses15 and parents,16 and particularly in widowers,17,18 and studies have suggested that spouses are affected by their partner’s mental health.19 Suicidal thoughts are not uncommon in the bereaved,20 and a previous study suggests that spousal bereavement through suicide increases the suicide risk more than bereavement by other modes of death.13 Losing a child is associated with the risk of suicide,16 whereas being a parent is protective against suicide.16
Few studies have examined gender differences for these risk factors, while adjusting for presumably important confounders and risk factors, such as own psychiatric admission,21 marital status,22 and labour market status,23,24 which is therefore the aim of this study.
METHODS
Data were obtained by linking Danish population based registers using the unique personal identification number, which is assigned to all persons living in Denmark and used across all registration systems.25
The Danish Civil Registration System25 was used to identify children. After April 1968, linking information between parents and children relies basically on birth registrations, and before 1968, parents were identified as the adults sharing the same address as the child. A link to a father would be missing if a woman, who was living alone, did not identify the father, which would be uncommon because of the father’s mandatory alimony pay to child support.
The Danish Medical Register on Vital Statistics contains dates and causes of all deaths in Denmark recorded from the cause of death certificates.26 Suicide was defined as ICD827 codes E950–959 and ICD1028 codes X60–X84. ICD9 was never used in Denmark.
The Danish Psychiatric Central Register includes all admission and discharge dates and diagnoses according to the World Health Organisation ICD8 and ICD10 classification of all psychiatric inpatient facilities in Denmark since 1969.29 There are no private psychiatric hospitals in Denmark, and all treatment is free of charge.
The Integrated Database for Longitudinal Labour Market Research30 covers the entire population and contains yearly information from 1980 and onwards with information from administrative registers. Furthermore, the register contains identification numbers of spouses and cohabitees recorded on 31 December. A cohabitee is a non-first degree relative of the opposite sex with an age difference <15 years who is sharing a residence with only two adults.
All subjects, aged 25 to 60 years, who had committed suicide during the period 1982 to 1997, were identified from the Danish Medical Register on Vital Statistics. Using a nested case-control design, each person committing suicide was matched to a random subsample of exactly 20 persons of the same sex, who were born the same year and who were alive at the particular matching date and age (in days)—that is, the gender-birth year stratified controls were at risk at the same age and date.31 To make the selection feasible and to minimise the computational burden, a random 5% sample was selected from the entire population within which controls were randomly selected. Cases and controls were only included if they had been living in the country during the two preceding years. All spouses and cohabitees living with the subjects on 31 December two years before, and children were then identified.
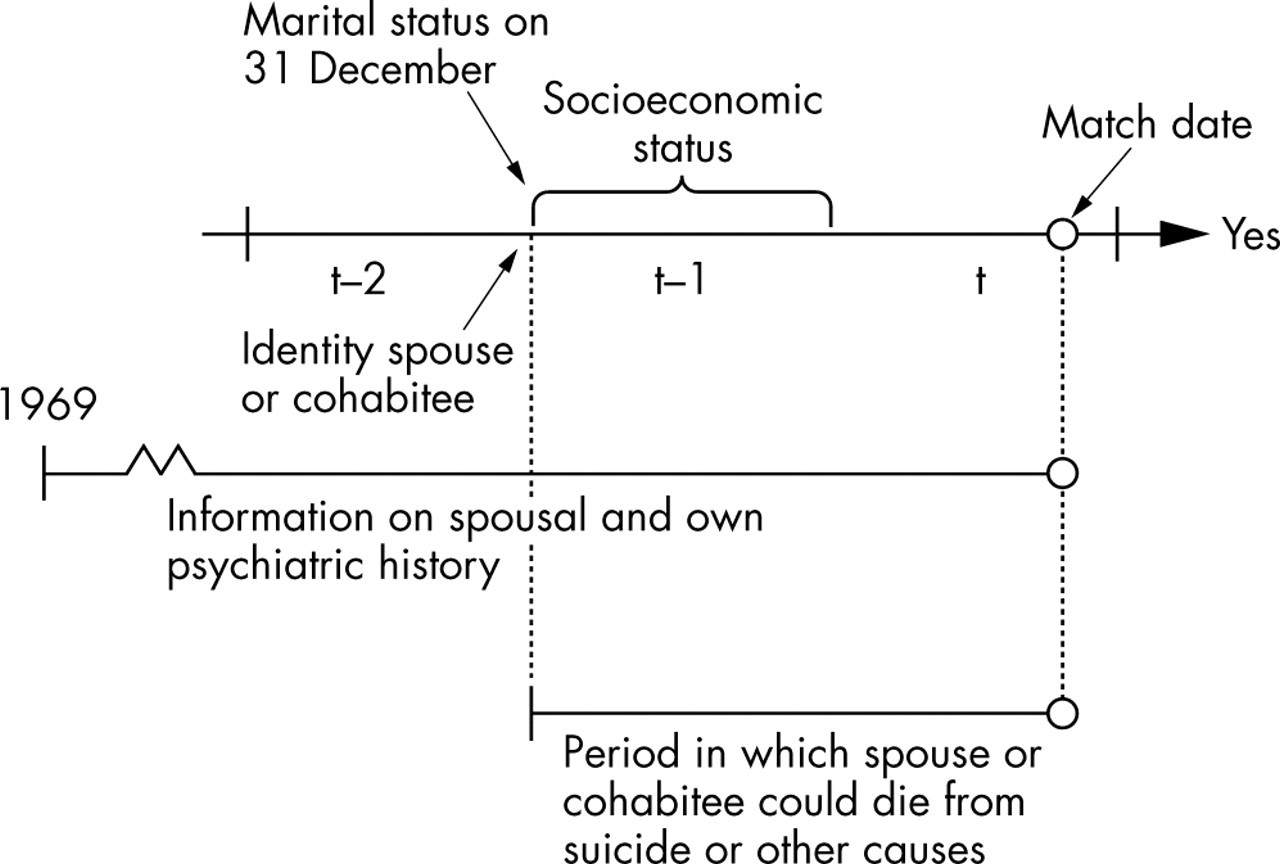
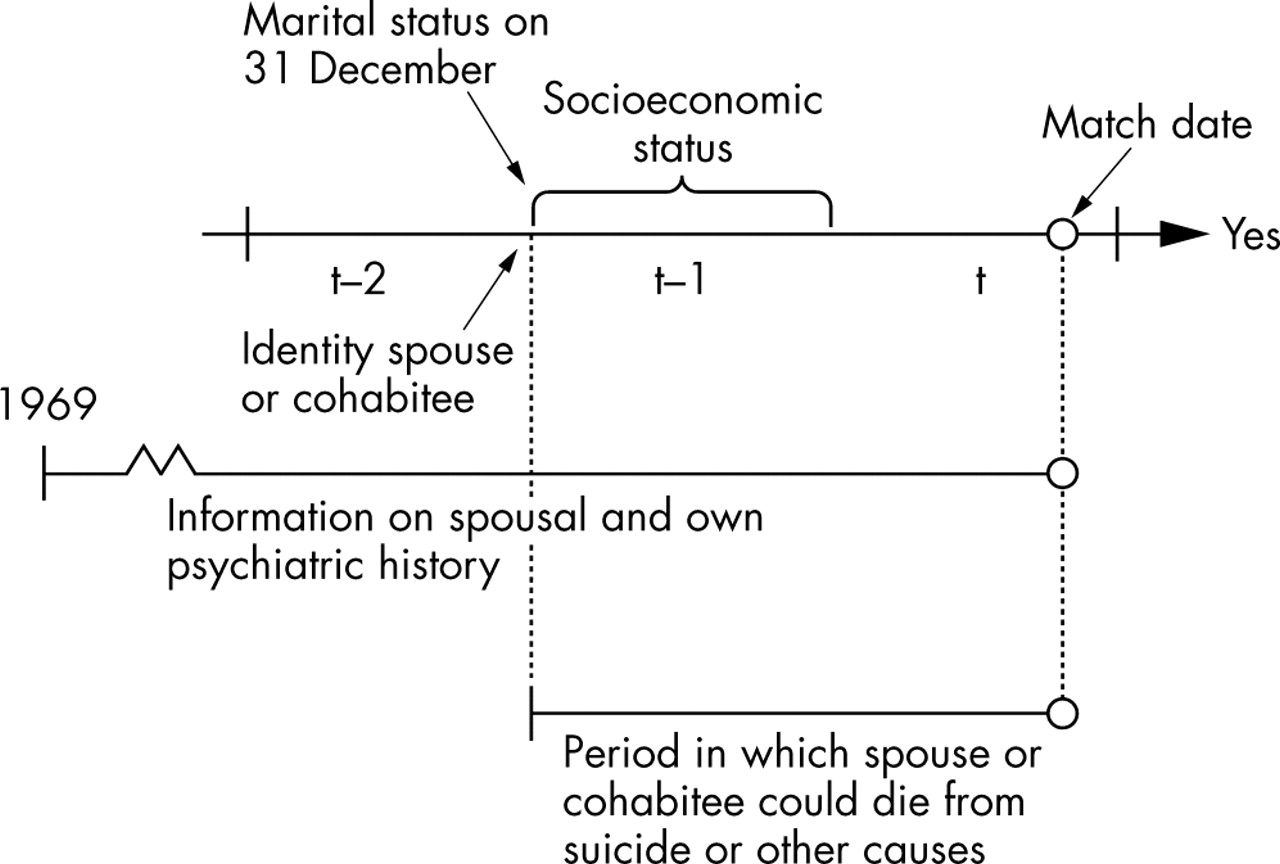
The variables derived from the Danish Psychiatric Central Register were duration of current discharge period and diagnosis at latest discharge. Information on the partner and children, before the particular matching date, was added from the Danish Medical Register on Vital Statistics. Figure 1 describes the study design. Note that a spouse can only die in the period between 31 December two years earlier and the matching date.
{kind=link}
Design and definition of primary explanatory information included in the analysis of suicide risk in the years ( = t) from 1982 to 1997. Information on children is available if they are born after 1968 or living with the parent after April 1968.
Demographic and socioeconomic factors included were variables describing marital status on 31 December two years earlier (cohabitating or married and living with the spouse, living alone and being widowed, divorced, married but separated, or never married), job status during the previous year (fully employed or self employed, unemployed for 1%–20%, 21%–80%, and 81%–100% of the year, recipients of other social benefits including disability pensioners, housewives, and a few students), educational achievement (university, bachelor or other of similar duration, vocational training, high school, primary school, and unknown), gross income the previous year (age-gender-year specific quartiles), number of children born before the matching date. Through the Danish Civil Registration System,25 historical information on widowhood and whether never married stems back to 1924, when local municipal registers were created.32 It is mandatory to report a change of address within five weekdays.
Data were analysed by conditional logistic regression, with each case forming a separate stratum, using the PhReg procedures in SAS (version 8.1), and relative risks, Wald statistics (W), 95% confidence bands, and associated p values were computed.31 Age interactions were tested by including age in years as a continuous covariate among the exposed and zero otherwise. The first model (model 1), the second model (model 2), and the third model (model 3) included the risk factors separately, simultaneously, and simultaneously by gender in a multivariable model.
RESULTS
In total, 9011 (2867 female) cases and 180 220 controls were identified. The distribution of cases and controls over the risk factors are shown in the first column of the tables.
The risk of suicide was increased if a spouse or cohabitee had been admitted with a psychiatric disorder (table 1: age and sex adjusted risk rates; model 1), and particularly, if the first admission had been within the period from 31 December two years earlier and until the matching date, which is a period of less than two years. The suicide risk was less pronounced if the partner had been admitted before 31 December two years earlier.
Suicide in relation to spousal or cohabitant’s psychiatric admission, suicide, or other mode of death for the 9011 people who committed suicide and 180 220 controls
The risk of suicide was increased among people whose spouse or cohabitee had died. The death of a spouse or a cohabitee by suicide was more indicative of suicide, whereas there were no differences between spouses and cohabitees. People who were married and living with their spouse had a lower suicide rate, while the suicide rate was increased among people who were separated, and slightly increased in cohabiting couples.
When all factors, including the persons’ own psychiatric admission, death of children, and socioeconomic status, were considered (table 1: column 4; model 2), the suicide risk remained increased among people whose spouse or cohabitee had been admitted with a psychiatric disorder. This increase was particularly pronounced if the spouse or the cohabitee had been first admitted during the period since 31 December two years before. The concordance of psychiatric admission in both partners (risk ratio 1.02; 95% confidence interval, 0.78 to 1.34, no cases/controls = 235/363) and the partner’s psychiatric diagnosis did not affect the suicide rate (W = 2.98, df = 4, p = 0.56). The death of a spouse or cohabitee remained strongly related to suicide in the surviving partner. Suicide bereavement was more indicative of suicide in spouses (W = 6.83, df = 1, p = 0.009) and cohabitees (W = 4.90, df = 1, p = 0.03) but not statistically different for spouses and cohabitees. Compared with the married, people who were cohabiting or living alone were at a higher risk of suicide. The effect decreased slightly with age in the divorced and the never married persons.
Table 2 shows the results concerning the effect of the confounding risk factors (model 1 and 2). There were higher rates of suicide in psychiatric patients—especially shortly after hospital discharge (model 2). Among people previously admitted to a psychiatric hospital, patients admitted with depression experienced a higher suicide risk, whereas the rate associated with schizophrenia and alcohol misuse was smaller than the rate associated with other psychiatric disorders. Compared with the general population, the risk ratio associated with a specific diagnosis must be multiplied by the relevant risk ratio associated with duration since last discharge. The unadjusted suicide risk seemed more closely related to suicide than other modes of death of a child. This difference disappeared after adjusting for parental psychiatric admission (data not shown). Being a parent was protective against suicide, especially if to more than one child. The suicide risk was increased in the unemployed and those outside the labour market, in those with lower income, but unrelated to educational attainment.
Suicide in relation to psychiatric admission; suicide and death among children and number of children, income, labour market affiliation, and educational attainment
Table 3 shows the results from the gender stratified model (model 3). Although not statistically distinct by gender, the partner’s recent psychiatric admission increased the suicide rate numerically more in women. Bereavement by suicide was more indicative of suicide in women (W = 7.06, df = 1, p = 0.008) and men (W = 8.42, df = 1, = 0.004) than bereavement after other modes of death. The association with a partner’s death by other causes was more pronounced in men (rate = 2.92, W = 6.02, df = 1, p = 0.01), and although not statistically significant, the rate was considerably higher (about 3.05) in men whose partner committed suicide compared with their female counterparts. The suicide rate in widowers was significantly higher than the suicide rate in widows. The rates associated with losing a child differed little by gender and cause of death, and having children was only protective in mothers. While the interaction between own and partner’s psychiatric admission was non-significant (W = 1.89, df = 2, p = 0.39), the additional interaction effect of own psychiatric admission and partner’s death (risk ratio 0.35; 95% confidence interval, 0.16 to 0.79, number cases/controls = 15/29) and the additional interaction effect of partner’s death and partner’s admission (0.31; 0.15 to 0.66, number cases/controls = 55/26) did not further increase the suicide risk.
Suicide in relation to partner’s psychiatric admission, death by suicide, or other modes of death and marital status
DISCUSSION
Main results
Suicide is more common in both husbands and wives whose marital partner has been admitted to a psychiatric hospital, especially if the first admission has been within the past two years, if their partner or child has died, especially if the partner died by suicide or the subject is male, if they are living alone whether they are separated, divorced, or never married. While the impact on the suicide risk of partner’s admission with a psychiatric disorder did not differ by gender, being a parent is only protective against suicide in women.
Partner’s psychiatric admission
In keeping with a previous study,13 the results further show that spousal psychiatric illness increases the suicide risk in both husbands and wives, which suggests that mental illness could have an impact on other family members beyond a social impact.33 The suicide risk increase associated with partner’s recent admission is almost two times higher in women, but had the study, in contrast with fact, found a significant gender difference, then the association would more probably have been causal.
Although people tend to marry people with resembling traits,14 such as those associated with psychiatric illness,34 and while a study has suggested that patients with schizophrenia might find a marital partner during admission,35 and even if shared environmental factors may put partners at risk of the same diseases,36 the suicide risk is not further influenced by the concordance of psychiatric admission. However, this does not entirely rule out the possibility that generic factors are at play through assortative mating, as psychiatric illnesses cluster in families.37
Partner’s suicide and death
Conjugal bereavement has an impact on the mortality among surviving spouses,38 and spousal suicide bereavement might increase the suicide risk more than bereavement after other modes of death.13 In this study, spousal loss by suicide increased the suicide risk more in both genders, than spousal loss after other modes of death. Furthermore, men experienced an approximately three times higher suicide risk increase than their female counterparts when their partner died by other causes, which is in keeping with studies on elderly widowers.18,39 Although non-significant, the results could show that this is also true for men bereaved by suicide. Men might be less prone to seek help, choose more lethal methods, be more impulsively violent, inclined to substance misuse,40 and might be more likely to suffer from untreated or undertreated mental illnesses.1 Furthermore, the data might cover a few cases of dyadic deaths,41 where men more often are the perpetrators.42
Key points
-
Husbands and wives whose marital partner has been admitted with a psychiatric disorder are at increased risk of suicide.
-
Conjugal bereavement is particularly indicative of suicide in men.
-
Spousal suicide is particularly indicative of suicide.
-
Child bereavement is associated with parental suicide in both parents.
-
Being a parent is protective against suicide in women.
-
Being separated, divorced, never married, or being cohabitant induce a similar suicide risk in both sexes.
Nevertheless, these gender differences suggest that assortative mating is a less likely explanation for a suicidal behaviour, and therefore, that this result is more probably attributed to an environmental factor than to a genetic susceptibility.
Interactions between psychiatric admission and spousal death
Although highly associated with suicide, the death of a partner increased the suicide risk less in previously admitted patients. This might suggest that psychiatric inpatient treatment could prevent suicide, or that a behavioural trait associated with some disorders (for example, a violent behaviour43) is related to the death, or simply, that there is an upper limit to grief. Likewise, experiencing a partner dying did not increase the risk to the same extent when the partner had been admitted with a psychiatric disorder. Recognising suicidal behaviour as a concomitant of psychiatric illness may alleviate the strain caused by the death of the mentally ill partner. However, a reverse causal relation cannot be ruled out as a study has suggested that people with severe mental illness are at increased risk of homicide.44 Nevertheless, effect modifications should be interpreted with caution when the main effect is very strong. Lastly, the analysis could not distinguish the rates associated with whether the partner had been admitted with depression, schizophrenia, alcohol misuse, mania, or other psychiatric disorders.
Child bereavement and parenthood
Losing a child has an impact on parents’ mental wellbeing45 and increases their suicide risk.16 The unadjusted analysis suggests that suicide bereavement of a child is more indicative of parental suicide than bereavement by other causes, while the adjustment for parental psychiatric admission level out the difference. However, parental psychopathology could be an intermediate stage on the causal pathway, and not only a confounding factor. In keeping with earlier studies,16 the results suggest that being a parent is protective against suicide only in women. However, a suicidal behaviour might diminish the chance of becoming a parent.
Policy implications
The suicide, death, or psychiatric illness of a family member can have a huge impact on the wellbeing of other family members
Marital status
People who are living alone have a higher suicide risk, or similarly marriage could be protective against suicide.40 This study further suggests that the highest risk increase is in widows/widowers followed by separated, divorced and never married people, and the results confirm that widowers have a higher risk than widows. In contrast with a previous paper published in this journal,22 the results show that divorced men and women experience almost the same risk increase. Two explanations seem possible: one is that Danish women are often integrated on the labour market, so that they have the same social support and do not suffer a much higher economic loss when divorced, as explained by Kposowa.22 Another possible explanation is that the results are based on updated information on marital status as suggested earlier,46 and furthermore, the test for non-proportionality46 with age suggests that the risk increase associated with divorce declines with age. However, it is important to remember that there are more than two male suicides per female suicide.
Weaknesses of the study
This study has a number of shortcomings. For instance, the findings depend on the availability of data: an illness episode, which did not lead to admission, or a suicide reported as an accident or an open verdict, or missing links to children who were not living with their parent in 1968, could lead to a misclassification bias. In some instances, the statistical power is rather limited especially when considering gender differences associated with partner or child bereavement.47 As in most observational studies, the effects presented here do not necessarily equal the desired causal effects.48 A marital breakdown or other unobserved events in period between 31 December two years ago and the matching date could have influenced the results. Although the highest suicide rates are to be found among the elderly population,49 this study includes only people aged 25 to 60 years, which is an age range where spousal death is rare, usually sudden, and unanticipated.
In conclusion, the suicide risk is increased in people, whose partner has been admitted with a psychiatric disorder, whose child or partner has died, especially if the partner has died by suicide or if the subject is male, whereas having children seems only to protect against suicide in women but not in men. Despite the very high rates and because of the rarity of these stressful life events and suicide, targeting prevention efforts at families where such an event has occurred could probably prevent few suicides. On the other hand, few, if any strategies, for preventing suicide have been shown to reduce suicide.50,51
REFERENCES
Footnotes
-
Funding: the study was financially supported by the Stanley Medical Research Institute. The National Centre for Register-based Research is funded by the Danish National Research Foundation.
-
Competing interest: none declared.
Linked Articles
- In this issue