Article Text

Abstract
Study objective: The principle of equity aims to guarantee allocation of healthcare resources on the basis of need. Therefore, people with a low income and persons living alone are expected to have higher healthcare expenditures. Besides these individual characteristics healthcare expenditure may be influenced by country of birth. This study therefore aimed to investigate the role of country of birth in explaining individual healthcare expenditure.
Design: Multilevel regression model based on individuals (first level) and their country of birth (second level).
Setting: The city of Malmö, Sweden.
Participants: All the 52 419 men aged 40–80 years from 130 different countries of birth, who were living in Malmö, Sweden, during 1999.
Main results: At the individual level, persons with a low income and persons living alone showed a higher healthcare expenditure, with regression coefficients (and 95% confidence intervals) being 0.358 (0.325 to 0.392) and 0.197 (0.165 to 0.230), respectively. Country of birth explained a considerable part (18% and 13%) of the individual differences in the probability of having a low income and living alone, respectively. However, this figure was only 3% for having some health expenditure, and barely 0.7% with regard to costs in the 74% of the population with some health expenditure.
Conclusions: Malmö is a socioeconomically segregated city, in which the country of birth seems to play only a minor part in explaining individual differences in total healthcare expenditure. These differences seem instead to be determined by individual low income and living alone.
- healthcare utilisation
- ethnicity
- multilevel analysis
Statistics from Altmetric.com
Sweden has a universal system that supports all health care. Only about 6% of health care is provided by private care providers. The Swedish system is founded on the principle of equity,1 and aims to guarantee allocation of healthcare resources on the basis of need, rather than on the basis of either socioeconomic position, civil status, or country of birth. It is a known fact that low socioeconomic position (that is, a low income)2 and a weak social network (for example, living alone)3 impair physical and mental health.4 In Sweden people with a low income and people living alone are therefore expected to have higher health expenditures.
It is also possible that health and healthcare utilisation may be influenced by country of birth.5 People born in the same country may share similarities because in addition to their geographical origin and language they hold a number of economic, social, and cultural characteristics in common. This may condition similar patterns of health and health beliefs that might influence healthcare utilisation. A greater understanding of the influence of country of birth on healthcare utilisation is relevant for resource allocation,6 especially in cities with a large percentage of migrants, as is the case with Malmö, where 25% of the population are born abroad.
Using multilevel regression analyses we sought to study the effect of a low income and of living alone on total healthcare expenditure. We also aimed to investigate the role of country of birth in explaining individual differences in total healthcare expenditure.
POPULATION AND METHODS
Study population
The study population consisted of all 52 419 men aged 40–80 years from 130 different countries of birth, who were living in Malmö, Sweden, during 1999. The city of Malmö is the largest city (with 250 000 inhabitants) in the county of Skåne (with 1 170 000 inhabitants) in southern Sweden.
Assessment of variables
This analysis is based on the 1999 Register for Resource Allocation, which includes information on age, gender, civil status, income, country of birth, and individual direct health expenditures for all people in the county.
Individual total health care expenditures were calculated as a function of a patient’s own utilisation of all publicly financed health care, that is, all inpatient and outpatient hospital care, including visits to public and private general practitioners. Every contact with a specific health department generated a specific expenditure amount. Assessment of the expenditure for hospitalisation was based on expenditure itemised for diagnosis related groups; where this was not available (for example, in the case of oncological and psychiatric wards) costs were calculated as a function of the total cost per day in the ward. For outpatients, the cost was calculated by the visit rather than per day, using differentiated weights based on the category of the visit. Information on expenditures related to outpatient medication and nursing homes for the elderly population was not recorded.
Low income persons, for our purposes, were people with a pre-tax personal income less than the city median income of Kr179 235. “Pre-tax personal income” meant all income from capital, employment and business, and all income transfers (for example, pension payments, unemployment benefits, paid sick leave). The available information was on pre-tax personal income rather than household disposable income and people with a low personal pre-tax income may live in households with a high disposable income, a circumstance that is more common in women. Therefore, to improve the validity of income as a measure of social position we limited the study to the population of men.
People who were single, separated, or widowed were considered to be living alone. It needs to be emphasised that this definition did not consider unmarried couples or people cohabitating with other people in a household. If this bias would have been present it would have underestimated a possible association between living alone and healthcare expenditures.
Information was handled in such a way as to preserve the anonymity of the subjects. The use of this database for questions concerning resource allocation was approved by the Data Safety Committee at Statistics Sweden.
Statistical methods
The analyses were performed first on the whole male population in the given age group and thereafter on the 74% (38 536 of 52 419) of the population who had some health expenditure. We made multilevel models7–11 using linear regressions for the continuous logarithmic transformed expenditure variable expressed in Swedish crowns, with individuals considered to be at the first level, and countries of birth at the second level. Of the 130 different countries of birth represented in the Malmö population, 59 countries had fewer than 10 people. However, this disparity in the number of people among countries of birth is adequately handled by the multilevel regression analysis.8
Multilevel analysis accounted for the possibility that people born in the same country may to different degrees be alike in relation to factors that influence health expenditure. Simultaneously, the multilevel analyses established whether country of origin was important in understanding individual differences in healthcare expenditure.9
We computed first level variance (that is, differences between people within countries) as well as second level variance (that is, differences between countries) and their 95% confidence intervals (CIs). We calculated the intra-country of birth correlation (ICC) (that is, the percentage of the total variance in expenditure attributable to country of birth) as:

where Vc = variance between countries of birth
and Vi = variance between individuals.
A large ICC would indicate that differences between countries were responsible for an appreciable part of all the individual differences in healthcare expenditure observed throughout the city (that is, that country of birth played a significant part in understanding individual differences). On the other hand, an ICC close to zero would indicate that country of birth could be effectively ignored as a factor to help explain differences in healthcare expenditure.
Countries were ranked according to second level residuals (with 95% CIs indicated). The second level residual is the difference between the logarithmic mean expenditure in the country of birth and the logarithmic mean expenditure in the entire city of Malmö (that is, logarithmic expenditure ratio).
The following two multilevel models using linear regressions were analysed. In the first model we included age as a continuous variable centred at 60 years and introduced a square term to allow for a possible quadratic association between age and expenditure. In the second model we added the variables low income and living alone. The associations between the variables studied and the health expenditures were appraised using β coefficient (95% CI) in the fixed part of the models.
We also performed several multilevel logistic regression analyses upon the whole study population, with the individual dichotomous variables living alone, low income, and having some health expenditure as dependent variables. We studied the ranking of countries according to the second level residuals in a manner analogous to the procedure used for health expenditures. In the multilevel logistic regression, the secondlevel residuals corresponded to the logarithmic odds ratios (ORs). We quantified the degree to which these individual characteristics were clustered within countries by analysing the ICC. For calculating the ICC in the logistic regression, the individual variance was considered to be π2/3, as discussed by Snijders and Bosker.8
Parameters were estimated using the restricted iterative generalised least squares (RIGLS) procedure. Extra-binomial variation was explored systematically in all binomial models (low income, living alone, and having some healthcare expenditure); however, we found no evidence for under-dispersion or over-dispersion. The MLwiN, version 1.1 software package,12 was used to perform the analyses.
RESULTS
In 1999 25% (13 286 of 52 419) of the men between the ages of 40 and 80 in the city of Malmö had been born in 129 countries other than Sweden, a percentage that is one of the largest of its kind in Sweden.
Key points
-
A multilevel regression analysis that considered country of birth as a higher level in which people are culturally nested seemed to be both statistically and conceptually a more appropriate analytical approach than a single level analysis.
-
Simple ethnic categorisations (such as migrant compared with Swedish born) do reflect socioeconomic position, but do not seem appropriate for studying the impact of socioeconomic or ethnic background on healthcare utilisation.
-
Although Malmö is a socioeconomically segregated city, country of birth seems to play only a minor part in total healthcare expenditure.
Figure 1 shows that people born in Sweden presented a comparatively high probability of living alone (fig 1A) but showed the lowest probability of having a low income (fig 1B). In fact, country of birth proved to be important in understanding income differences (18% of the total variation in the age adjusted probability of having a low income was attributable to this second level), as did living alone (13%). The proportion of people having some health expenditure (fig 1C) was fairly similar for all countries; only 3% of the total differences were at the country of birth level.

Multilevel analyses showing age adjusted, between country of birth differences (second level residuals) in the probability (logarithm ORs (log ORs)) of living alone (A), having a low income (B), and having some healthcare expenditure (C). Uncertainty around the estimations is appraised by 95% confidence intervals (CIs). Sweden as country of birth is highlighted as a grey, larger triangle. In the comparisons the entire population of the city of Malmö is used as reference. Analyses are based on 52 419 men aged 40–80 years from 130 different countries of birth, who were living in Malmö, Sweden, during 1999.
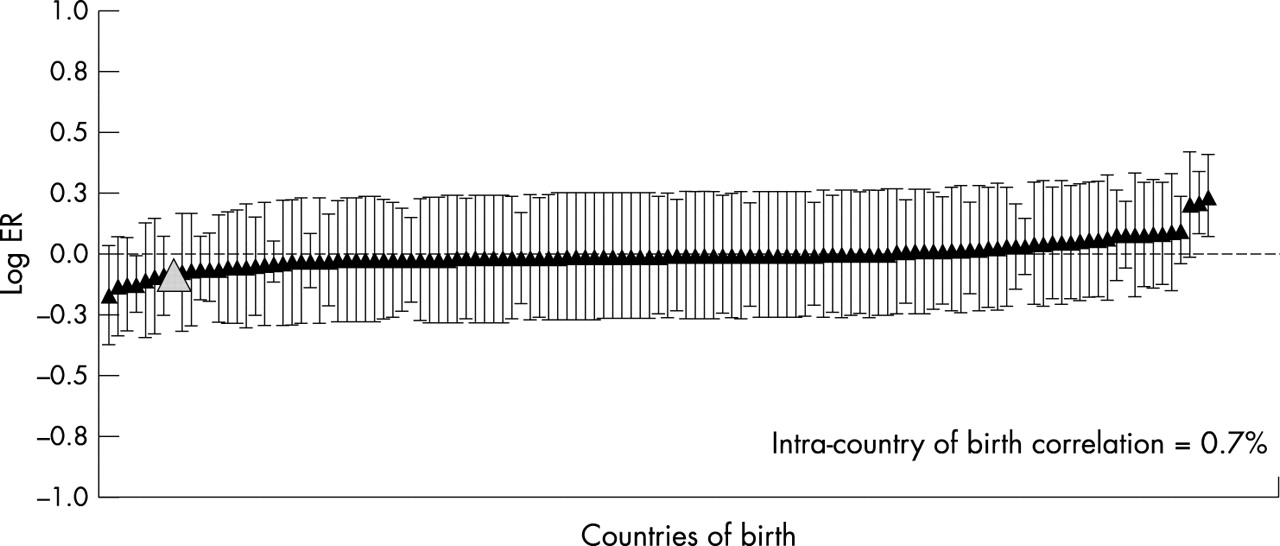
Expenditure increased with age, as well as with a low income and living alone (table 1). Differences in health expenditure among countries of birth, albeit very small, were statistically significant (table 1; fig 2). Only a few countries of birth could be distinguished with any certainty from either the city mean or other countries (fig 2). Country of birth did not provide much extra information for understanding health expenditures, as this second level only explained 0.7% of the total age adjusted variation in expenditure (table 1, model 1). The remainder (99.3%) was variation at the individual level, which proved to be unrelated to country of birth. After further adjustment for individual low income, and living alone, the intra-country correlation was reduced to 0.4% (table 1, model 2).
Multilevel analysis of health expenditures in the city of Malmö, Sweden, in 1999. Analyses are based on the 74% (38 536 of 52 419) of the men aged 40–80 years from 130 different countries of birth who had some health expenditure. Countries of birth are at the second, and individuals at the first level
{kind=link}
{kind=link}
Multilevel analysis showing age adjusted, between country of birth differences (second level residuals) in mean health expenditure (logarithmic expenditure ratios (log ERs)). In the comparisons the entire population of the city of Malmö is used as reference. Uncertainty around the estimations is appraised by 95% confidence intervals (CIs). Sweden as country of birth is highlighted as a grey, larger triangle. Analyses are based on 52 419 men aged 40–80 years from 130 different countries of birth, who were living in the city of Malmö, Sweden, during 1999.
DISCUSSION
Our study shows that in the study population low individual income and living alone were associated with higher health expenditures, and suggests that healthcare resources, as measured by total healthcare expenditure, are distributed according to individual needs, at least as they relate to these sociodemographic characteristics. In a health system characterised by equality in access to health care, use of health services reflects socioeconomic differences in health status.
Malmö is a socioeconomically segregated city, and country of birth seems to play an important part in understanding individual differences in the probability of having a low income (ICC = 18%) and living alone (ICC = 13%). However, country of birth was seen to play a minor part when it came to individual health expenditure. No more than 3% of the individual differences in the probability of having some health expenditure were attributable to country of birth, and this percentage was only 0.7% in relation to magnitude of cost in the 74% of the population who had some health expenditure.
It is noteworthy that Sweden had the lowest percentage of men with a low income, but a comparatively high percentage of men with some health expenditure, as revealed by a comparison of all the countries of birth (fig 1). This finding suggests that people born in Sweden may access the Swedish healthcare system more easily than people from most other countries of birth. However, once a person has accessed the healthcare system, country of birth seems irrelevant in relation to total healthcare expenditure (fig 2).
Policy implications
-
Authorities at both national and county level should be aware that health policies that distinguish between Swedish born and migrants implicitly mean that the underlying explanation rests on a person’s migrant status and may paradoxically promote the stigmatisation of migrants rather than their integration.
-
Even if in concrete situations a focus on specific ethnic minorities may facilitate our understanding of relative health and healthcare needs, broad ethnic taxonomies are not informative and should be avoided in public health reports.
-
When planning resource allocation in the city of Malmö, one way of potentially improving general societal integration might be to focus on socioeconomic inequalities in health wherever they are present, rather than on migrant status in itself.
-
Sweden has had a long history of equitable and broad based social investments. It is possible that over time such investments help counteract discriminatory processes and help even out differences in access to healthcare resources between people who have different countries of birth.
The differences in healthcare expenditure between countries of birth were significant; however, the amount of individual variation related to the country of birth was very small compared with the overall variation (ICC = 0.4% after adjusting for age and individual socioeconomic composition of the countries). Consequently, it would be misleading to conclude that contextual factors related to country of birth are epidemiologically significant for understanding health expenditures in Malmö. In fact, excluding country of birth from the analysis would not have appreciable consequences for understanding determinants of health expenditures in the city. It seems that the city of Malmö, as previously reported for the country of Sweden as a whole,13 does not have a pronounced pattern of inequity in access to health care for ethnic minorities. Our study, however, neither focused on access to specific services, nor did it investigate specific patterns of healthcare utilisation, in which areas other authors have observed differences, both in Sweden and elsewhere.1415
In our investigation we analysed specific countries of birth rather than making simple ethnic categorisations (for example, migrant compared with Swedish born), which seemed inappropriate for capturing a possible heterogeneity in healthcare utilisation. In general the use of ethnic classifications in epidemiological and biological research has been questioned.16 Ethnicity is a socially determined variable that is confounded by socioeconomic status.17 Its complex nature makes it difficult to use as a valid classification,18 and the latter can certainly not be achieved by a simple dichotomisation.
Investigating the health status of migrants by comparing it with that of Swedish born people or using this dichotomisation as a proxy for social position19 implicitly means that the underlying explanation rests on migrant status, rather than upon class, lifestyle, or social position. This approach leads to uncertain assumptions about the existence and importance of cultural and biological differences being asserted as fact.17 The perception that the health of migrants is poor promotes the belief that migrants are a burden to society, and results in placing blame on migrants.16 As Bhopal says, “By emphasising the negative aspects of the health of the minority groups research may have damaged their social standing.”16 This is a teleological paradox, as most “migrant” studies, rather than being racist or tending to stigmatise migrants, aim to reduce inequity.
In analysing the extent to which the ethnic dichotomisation “migrant compared with Swedish born” was confounded by socioeconomic position we also performed a common regression analysis at the individual level, studying total health expenditures of migrants as compared with those of people born in Sweden, an approach adopted in many studies. We found an age adjusted expenditure ratio of 1.08 (95% CI: 1.05 to 1.12) that disappeared, to become 1.00 (95% CI: 0.96 to 1.03), after adjusting for individual income and living alone. Considering the above, simple ethnic categorisations (such as migrant compared with Swedish born) do reflect socioeconomic position, but do not seem appropriate for studying the impact of socioeconomic or ethnic background on healthcare utilisation. An appropriate way of improving general societal integration may be to focus on socioeconomic inequity wherever it is present, rather than on country of birth.
We were working with information on country of birth, but it is possible that second generation immigrants (that is, people born in Sweden but sharing the language and culture of their foreign born parents) have a different pattern of healthcare utilisation than do people born in Sweden of Swedish parents. This fact may lead to misclassification and reduce the differences in healthcare utilisation seen between Swedish born people and people born in other countries. However, only about 3% of the people in the age groups included in this study (that is, 40–80 years of age) were second generation immigrants.
By 1999 Malmö was divided into 10 different areas that may differ in healthcare availability. Therefore, area of residence may confound differences in healthcare expenditure between countries of birth in cases where people from a certain country are geographically segregated in specific city areas. To investigate this aspect we performed an analysis (not presented in the tables) adjusting for residential area as a fixed effect. Control for this geographical variable did not affect the fairly small size of variance in total healthcare expenditure between countries of birth. Because of the small number of city areas and because our investigation focused on country of birth rather than on geographical effects we did not perform a cross classified multilevel analysis.
In this study we performed a multilevel regression analysis that considered country of birth as a higher level in which individuals are culturally nested. This approach seemed to be both statistically and conceptually a more appropriate analytical approach than a single level analysis that disregards the natural structure of the data. In our analysis we focused mainly on the epidemiological interpretation of components of variance in health care expenditures (individual and country of birth) and used this information to understand the importance of relative average differences between countries of birth.9
Sweden has had a long history of equitable and broad based social investments, and has a very homogeneous healthcare infrastructure.20 It is possible that over time such investments help counteract discriminatory processes and “even out” differences in access to healthcare resources between different countries of birth. As our analytical approach is still fairly uncommon, it remains to perform similar analyses in other cities in which contextual factors related to country of birth may play a larger part as determinants of total healthcare expenditure.
REFERENCES
Footnotes
-
Funding: This study was supported by the Skåne County Council.
-
Conflicts of interest: none declared.