Article Text

Abstract
Objective: To examine the relation between socioeconomic position in early life and mortality in young adulthood, taking birth weight and childhood cognitive function into account.
Design: A longitudinal study with record linkage to the Civil Registration System and Cause of Death Registry. The data were analysed using Cox regression.
Setting: The metropolitan area of Copenhagen, Denmark.
Subjects: 7493 male singletons born in 1953, who completed a questionnaire with various cognitive measures, in school at age 12 years, and for whom birth certificates with data on birth and parental characteristics had been traced manually in 1965. This population was followed up from April 1968 to January 2002 for information on mortality.
Main outcome measures: Mortality from all causes, cardiovascular diseases, and violent deaths.
Results: Men whose fathers were working class or of unknown social class at time of birth had higher mortality rates compared with those whose fathers were high/middle class: hazard ratio 1.39 (95% CI 1.15 to 1.67) and 2.04 (95% CI 1.48 to 2.83) respectively. Birth weight and childhood cognitive function were both related to father’s social class and inversely associated with all cause mortality. The association between father’s social class and mortality attenuated (HRworking class1.30 (1.08 to 1.56); HRunkown class1.81 (1.30 to 2.52)) after control for birth weight and cognitive function. Mortality from cardiovascular diseases and violent deaths was also significantly higher among men with fathers from the lower social classes.
Conclusion: The inverse association between father’s social class at time of birth and early adult mortality remains, however somewhat attenuated, after adjustment for birth weight and cognitive function.
- birth weight
- cognitive function
- mortality
- social class
- longitudinal study
Statistics from Altmetric.com
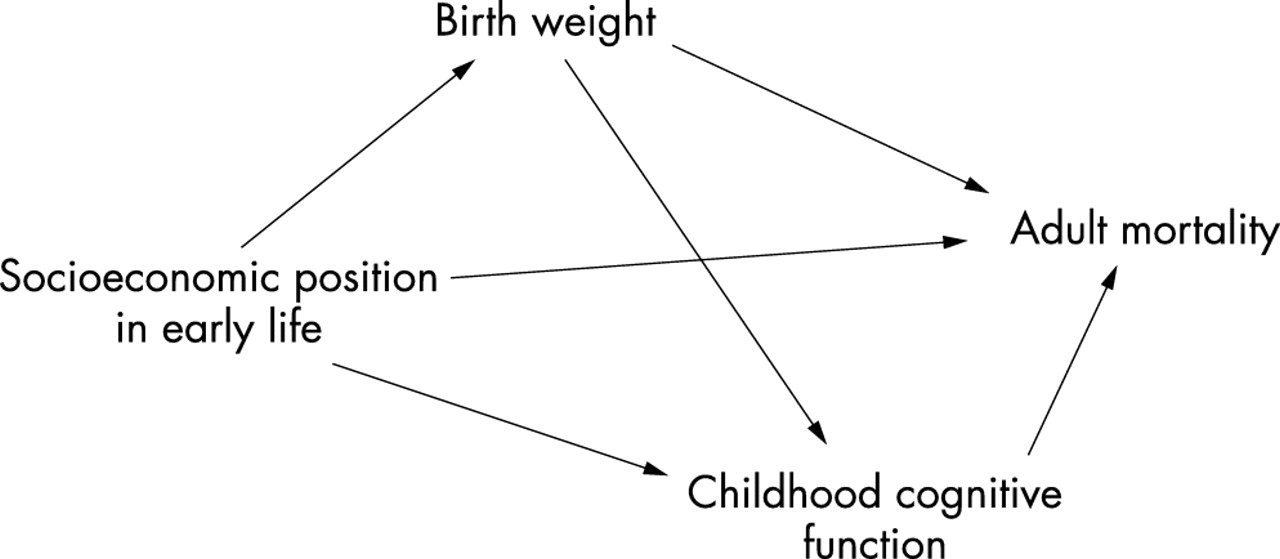
Recently, we have experienced an increased research interest in early life origins of adult chronic disease, and a number of birth cohort studies have shown that social factors operating during early life are related to mortality in adult life.1–5 The social environment in early life has also been linked to birth weight and childhood cognitive function,6–8 which are both related to mortality later in life.8–10 Furthermore, some studies have related size at birth to cognitive function in childhood or adolescence.11–13 Thus, as figure 1 suggests low birth weight and impaired cognitive function are possible mediators of the relation between socioeconomic position in early life and adult mortality. So far, however, no study has examined whether this relation is accounted for by, or acts independently of, birth weight and childhood cognitive function.

{kind=link}
Schematic representation of the examined potential pathways between socioeconomic position in early life and adult mortality, addressed in this study.
In this study, we analyse the relation between socioeconomic position in early life (that is, father’s social class and mother’s marital status at time of birth) and mortality in young adulthood in a cohort of Danish men born in 1953. The data allow us to look at later all cause and cause specific mortality, taking information on birth weight and childhood cognitive function into account. We also examine whether early socioeconomic position modifies the effects of birth weight and cognitive function on adult mortality.
METHODS
Study population
According to official statistics, 12 270 boys were born within the metropolitan area of Copenhagen during 1953. These boys formed the study population of the Danish longitudinal study called Project Metropolit: a sociological study that was carried out at the Department of Sociology, University of Copenhagen, from 1965 to 1975, with the aim of examining social mobility.14
In April 1968, the Danish Civil Registration System (CRS) was established, and a unique 10 digit personal identification number (which includes the day, month and year of birth of the person) was allocated to all persons alive and living in Denmark at that time. This register keeps updated information on vital status and emigration for each person.
A total of 11 532 of the males born in the Copenhagen region in 1953 were registered in the CRS (that is, alive and living in Denmark in 1968). Those not identified in the CRS in 1968 were either dead (n¬500) or had emigrated from Denmark.14 We excluded 156 subjects from the dataset because they had requested that the CRS not disclose any information for research purposes. The remaining 11 376 persons constituted the Metropolit2000 Cohort which is the study population in this study.
Data sources and variables
In Denmark, data from all births are thoroughly entered into registers and birth certificates. When Project Metropolit was established in 1965, all available information from such certificates and registers was collected manually for the entire original study population.14 Information on date and place of birth, singleton or multiple birth, birth weight and length, father’s occupation, and mother’s age and marital status at time of delivery was included.
In 1965, the members of this cohort were given a questionnaire by their teachers in the classroom. The survey included an IQ test developed by Kell Härnquist, translated from Swedish,15 and a test of creativity (the Remote Associates test), developed by Sarnoff A Mednick.16 A number of boys, corresponding to 7877 (68.3%) of the Metropolit2000 cohort, participated in the school survey. The main reasons for non-participation in the survey were reported as general non-participation in school or class, individual absence from school on the day of data collection, and severe handicap or enrolment in special schools.14 Non-participants had the same mean birth weight than participants (3390 g), were more often born to single mothers (11.1% compared with 6.5%), and had a higher proportion of fathers with unknown occupation (15.1% compared with 8.7%).
In January 2002, the Metropolit2000 cohort was followed up for information on vital status in the CRS. If the person was not alive, or was living outside Denmark, information on date of death/emigration/disappearance was gathered. We identified causes of death for the period of April 1968 to December 1998 by record linkage to the Cause of Death Registry at the National Institute of Public Health. A total of 152 boys (1.9%) born as twins or triplets and 232 boys (3.0%) with missing birth data were excluded, leaving 7493 cohort members for the analyses.
From birth records, we used information on birth weight and the two available indicators of socioeconomic position in early life: father’s social class and mother’s marital status at the time of delivery. Father’s social class was classified according to the father’s position in the occupational structure of the society. Subjects were assigned, on the basis of father’s occupation, into 23 strata: non-urban self employed (4 strata); urban self employed (6 strata); white collar workers (5 strata); blue collar workers (5 strata); pensioners; students; and unknown. The preliminary data analyses showed that the estimates for self employed and white collar workers were very close, and they were consequently combined, leaving three categories: high/middle class, which included self employed and salaried employed; working class, which included skilled and unskilled workers; unknown, which also included the small groups of pensioners (n=1); and students (n=44). When the analyses were stratified according to social class, we combined working class and unknown in one category, termed “low social class.” Marital status of mothers was treated in two categories: married, and unmarried (that is, single, divorced, widowed). Birth weight was recorded in 100 gram groups and was analysed both as a continuous variable and in each of the five categories: <2500; 2500–2999; 3000–3499; 3500–3999; and ⩾4000 g. The initial data analyses showed that the estimates were nearly the same for the second and third and for the two largest categories, and, consequently, they were combined.
From the school questionnaire, we used the information on IQ and creative potential. The IQ test consisted of spatial, arithmetic and verbal sub-tests. In the spatial test, students were asked to choose one out of four alternative three dimensional figures, corresponding to a flat, two dimensional template. In the arithmetic test, students were to determine the logical sequences for a series of six numbers. In the verbal test, students were to identify, out of four alternatives, the antonym of a given word. Each sub-test included 40 problems, with a correct answer counting for one point, resulting in a range of 0–40 points. The overall test ranged from 0 to 120 points, with the highest value reflecting the best score. In the creativity test, students were to come up with a word that was associated somehow with three other rather different words. This test included 25 different word series, and each correct answer counted for 1 point, giving a scoring range of 0 to 25 points. Cause of death was based on official death certificates coded using the 7th Revision of the International Classification of Diseases for the years 1968–1969, the 8th Revision for 1970–1993, and the 10th Revision for 1994–1998. Cause of death was classified into the following selected end points: CVD (ICD7-codes 330–468; ICD8-codes 390–458; ICD10-codes I00-I52,I60-I99; ICD10-code K70); injuries and suicide (ICD7-codes 800–999; ICD8-codes 800–999; ICD10-codes V01-Y99); and other causes (all other codes).
Statistical methods
Associations between covariates were analysed using logistic and linear regression models. Associations between socioeconomic position in early life and mortality were analysed using Cox’s proportional hazards regression models, with age as the underlying time scale, and age in 1968 as time of entry. Men who emigrated or changed identity were censored at the date of this event. The proportional hazards assumption was evaluated for all variables by comparing estimated ln(-ln) survivor curves over the different categories of the variables being investigated, compared with ln(analysis time)—the so called “log-log” plots—and by tests based on the generalisation of Grambsch and Therneau.17 Statistical interaction between father’s social class and other covariates was evaluated using a likelihood ratio test. Statistical analyses were performed using STATA version 7.
RESULTS
During follow up, 541 men had died, and 275 were censored due to emigration (n=264) and disappearance or change of identity (n=11). The 300 censored subjects did not differ from the remaining cohort with respect to mean birth weight (3400 g) or percentage unmarried mothers, but they had a higher mean IQ (72.2 points versus 67.6 points) and their fathers were more often high/middle class (56.2% versus 45.7%). A total of 174 men had missing information on one or both cognitive tests and were excluded from the analyses presented here.
The distribution of socioeconomic position in early life, birth weight, and results of the cognitive function tests at age 12 years for the cohort, is shown in table 1. The unadjusted relative death intensity ratios, according to these characteristics, are also shown. We found a higher risk of death from age 15–49 years in sons of unmarried mothers, and sons of fathers in the working class or of unknown social class. Sons of unmarried mothers and sons of fathers in the two lower social classes also had a higher prevalence of low birth weight, compared with those with married mothers, and of low cognitive performance, compared with those with fathers from high/middle class. Birth weight and the two cognitive tests were inversely associated with mortality later in life, and the proportion of a low cognitive test score decreased with an increase in birth weight category.
Characteristics of 7319 male singletons in the cohort. Percentage with birth weight below 2500 g, percentage in the lowest quartile of cognitive tests, and crude risk of all cause mortality between age 15–49 years (95% confidence intervals) according to characteristics
The effect of mother’s single status on mortality attenuated considerably in all models when father’s social class was entered, and, therefore, marital status was not included in the multivariable analyses. The association between father’s social class and mortality was slightly reduced after controlling for birth weight, while the inclusion of IQ in the model caused a larger reduction of the social class estimate (table 2, model 1 and 2). The IQ and creativity tests were correlated (r=0.53); and when both variables were present in the model, the effect of the creativity test became insignificant (model 4). This was also seen in all other models, and, consequently, we excluded the creativity test from the final models. The inclusion of birth weight in the model with IQ did not affect the estimates for father’s social class or IQ, while the effect of birth weight was attenuated. However, social class, birth weight, and IQ remained significantly associated with mortality in the final model (table 2, model 5).
Hazard ratios for all cause mortality between ages 15 and 49 (95% confidence intervals) in relation to paternal social position, adjusted for birth weight and cognitive function for 7308 male singletons born in 1953
The hazard ratio for birth weight below 2500 g seemed to be higher for the low social class (HR 1.69 (1.07 to 2.64)) than for the high social class (HR 1.07 (0.46 to 2.45)). The second estimate, however, was only based on 15 deaths, and the risk estimates for the intermediate birth weight category showed the opposite tendency. Thus, the test for statistical interaction between father’s social class and birth weight was not significant (p=0.15). Visual inspection of mortality rates for each category of birth weight and IQ in the different social strata did not indicate any additive modifications of effects.
Although log-log plots and tests of zero slope gave no indication of violation of the proportional hazard assumption, the relations seemed to differ slightly, when the analyses were subdivided into early (age 15–34 years) and later (age 35–49 years) deaths (table 3). Father’s social class was associated with mortality before and after age 35 years, while the inverse relations with birth weight and IQ remained persuasive for the later deaths. The adjusted associations between covariates and mortality from specific causes are given in table 4. Father’s social class was significantly associated with deaths from CVD, violent, and other causes, before and after adjustment. When birth weight or IQ were controlled for, however, the effects were attenuated.
Hazard ratios for all cause mortality in young adulthood and early middle age (95% confidence intervals) in relation to paternal social class, adjusted for birth weight and childhood IQ, for 7308 male singletons born in 1953
Hazard ratios for death between ages 15 and 45* (95% confidence intervals) from cardiovascular diseases, accidents/suicide, and other causes, in relation to father’s social class, adjusted for birth weight and childhood IQ, for 7308 male singletons born in 1953
As a sensitivity analysis, all the reported analyses were repeated for all 7493 men, with cognitive test scores, in tertiles and including an additional category for those with missing data. This approach gave essentially the same results as those based on the subjects with complete information on all variables reported above.
DISCUSSION
In this cohort of Danish men born in 1953, we found a clear relation between adverse socioeconomic position in early life and increased mortality in young adulthood. Low birth weight and low childhood IQ were both associated with social disadvantage and increased adult mortality. Adjustment for birth weight and IQ somewhat decreased the hazard ratios for the indicator of childhood socioeconomic position (father’s social class at time of birth), but the estimates for all three variables remained significant. Analyses of cause specific mortality revealed consistent, positive associations with father’s social class.
One of the strengths of our study is follow up for mortality, which covered all cohort members. Losses to follow up, therefore, did not seem to result in a serious bias. Non-participants, however, included more boys from lower social classes, and, as special schools were not included in the school survey, it is most likely that this group also represents more boys with impaired mental skills. Thus, our conclusions might not apply to these disadvantaged groups. It should also be noted, in this context, that women were not present in the dataset. The information on social circumstances in early life was collected from birth registers of high quality, rather than relying on recall from the offspring in childhood or middle age. This might minimise subjective and biased classification of exposure status. Furthermore, cognitive function was assessed using two different measures in late childhood, at an age when test scores are assumed to be stable.18 On the other hand, we must admit that it could also be a study limitation to rely on data collected in another era; the current usefulness of measures of IQ and socioeconomic position in 1953 may fairly be questioned. In addition, we only had information on a few of the many other factors, such as adult socioeconomic position and behaviour, which might also confound and/or mediate the relation between socioeconomic position in early life and later mortality. However, looking at health in the long term by use of existing cohorts, while increasing the understanding of early life origins of adult chronic disease, will always have this problem. A few other study limitations should be considered. We showed that creative potential had no independent effect besides what was obtained by the IQ test, which measured three different cognitive skills. A possible explanation is that the tests were correlated, and, given the sample size of our study, the independent effects of both variables could not be supported. It should also be noted questions have been raised as to what IQ tests actually measure.19 Furthermore, the small number of cause specific deaths reduce statistical power and allow no firm conclusions to be drawn from these data.
These analyses only included a single measure of socioeconomic position in early life. We had information on participants’ occupation at age 20 years, but these data were incomplete and consequently not used in this study. On the other hand, the association between social position in early life and adult mortality has been shown in a variety of studies, even after taking account of socioeconomic circumstances in adulthood.1–3,20 A recent study from a cohort born in 1946, in the UK, demonstrated that mortality between ages 26 and 54 was strongly influenced by social circumstances in childhood as well as in early adulthood. A trivial effect of entering adult social indicators into models of childhood social position upon mortality indicated that these influences operate through different pathways, and that childhood social position is not simply a proxy for adult living conditions.3 We have no reasons to believe that the findings from the 1946 cohort should not apply for the Danish cohort, which in many respects is comparable with the UK cohort.
In this study, inclusion of birth weight and childhood IQ in the model reduced the risk estimates for father’s social class, indicating that these two variables mediate some of the effect. We also found the expected positive association between birth weight and IQ, and, in addition, our study showed that the effect of birth weight on mortality was attenuated when IQ was entered into the model. The latter finding suggests that cognitive function might be one of the pathways through which birth weight exerts its effect on mortality in adulthood. Thus, our study seems to support the postulated model (fig 1). We compared a Cox model that contained the intermediate variables to one that did not. This approach could be used to assess how much of the association between socioeconomic position and mortality could be accounted for by birth weight and IQ. We must admit, however, that such a measure depends on the chosen cut off points and reference category used, and there is no way to judge its precision.21 It is also advisable to use more complex models, such as structural equation models, to quantify the direct and indirect causal pathways postulated in a given lifecourse model.4,21 In the follow up study of children born in Aberdeen, Scotland,8 structural equation modelling was used to test direct effects of IQ at age 11, and of father’s occupation at age at death. The most fitting model interpreted IQ as a mediating factor between father’s occupation and age at death, while the models that assumed a direct effect of the social factor on age at death were not acceptable. It should be noted, however, that the Scottish analysis was restricted to those who died during follow up. The reason may be that the empirical model that treats social position in early life as a direct and mediating variable (through IQ) cannot easily be implemented in the Cox model.
Similar to the findings from a Finnish cohort study of 4630 men,7 our data suggested that the relation between birth weight and adult health is particularly strong in the lower social classes. This result indicates that social influences that alter growth also may change the risk of disease in adult life, and this supports a critical period model with modification of later effects.
CVD mortality was inversely related to father’s social class. The same was true of violent deaths, although to a smaller extent. Clear effects of childhood socioeconomic position have also been seen for CVD in a number of previous studies.3,20 This seems to support the postulated mechanisms related to accumulation of socially patterned risk factors for CVD. A number of non-exclusive explanations, however, exist for the association of socioeconomic position in early life with adult mortality. Birth weight and IQ may reflect genetic factors for early mortality, but could also be considered as proxy measures of a number of different environmental and behavioural factors that tend to cluster in families—primarily for social reasons—and this would influence the health of the members of these families.5 The relation between birth weight and childhood IQ could also support the hypothesis of a biological pathway, which suggests that malnutrition in early life affects the development of the brain and later cognitive function. IQ has also been related to final qualifications and adult behaviour, such as smoking, thus supporting the notion that this psychometric characteristic may influence health.8 The potential health effects of socioenvironmental exposures over a lifetime have been described in different lifecourse models.4,5 The sensitive period model states that the environment in early life influences later susceptibility to disease, while the cumulative effect model suggests an added influence of the number and/or duration of health damaging exposures, across the lifecourse, on disease risk. Low birth weight and low IQ were most prevalent in sons of fathers in the lower social classes and each exposure exerted an independent effect on mortality. The risk increased with the number of unhealthy exposures, and, consequently, our study seems to demonstrate a cumulative influence of socially patterned exposures, across the lifecourse, on mortality risk.4,5 Adjustment for the social class difference in birth weight and IQ, however, only explained a part of the observed social variation in mortality. This finding suggests that a sensitive period model also plays a part, although it should be noted that we only addressed a subset of the health related factors linked to socioeconomic position in early life.
Key points
-
Men with adverse socioeconomic position in early life have higher rates of mortality in young adulthood, even after control for birth weight and childhood cognitive function.
-
Low birth weight and low IQ are both related to adverse socioeconomic position in early life, and to increased mortality in young adulthood. This suggests a cumulative influence of socially patterned exposures across childhood, on mortality.
-
The relation between birth weight and adult health seems to be particularly strong in those with adverse socieconomic position in early life.
Policy implications
-
The mechanisms mediating the association between childhood socioeconomic position and health later in life have scarcely been investigated, but this knowledge is important for the prevention of such inequities. Birth weight and childhood cognitive function seem to be modifiable links.
-
This points up the importance of prevention strategies to improve the health of socioeconomically disadvantaged families, even before they have children.
In conclusion, this study provides support for the existence of a relation between socioeconomic position in early life and adult mortality in men, which cannot be fully accounted for by birth weight or childhood cognitive function.
Acknowledgments
We thank all those who initiated and/or continued the study from 1965 to 1983—K Svalastoga, E Høgh, P Wolf, T Rishøj, G Strande-Sørensen, E Manniche, B Holten, I A Weibull, and A Ortmann—for their thorough work on the project. Thanks to Knud Juel for providing data on causes of death.
REFERENCES
Supplementary materials
. Author Correction
Please note that there is an error in the 5th paragraph, next to last line, in the section DATA SOURCES AND VARIABLES
"ICD10-code K70" should read "100-152, 160-199; ICD10".
The correct paragraph is shown here:From the school questionnaire, we used the information on IQ and creative potential. The IQ test consisted of spatial, arithmetic and verbal sub-tests. In the spatial test, students were asked to choose one out of four alternative three dimensional figures, corresponding to a flat, two dimensional template. In the arithmetic test, students were to determine the logical sequences for a series of six numbers. In the verbal test, students were to identify, out of four alternatives, the antonym of a given word. Each sub-test included 40 problems, with a correct answer counting for one point, resulting in a range of 0�40 points. The overall test ranged from 0 to 120 points, with the highest value reflecting the best score. In the creativity test, students were to come up with a word that was associated somehow with three other rather different words. This test included 25 different word series, and each correct answer counted for 1 point, giving a scoring range of 0 to 25 points. Cause of death was based on official death certificates coded using the 7th Revision of the International Classification of Diseases for the years 1968�1969, the 8th Revision for 1970�1993, and the 10th Revision for 1994�1998. Cause of death was classified into the following selected end points: CVD (ICD7-codes 330�468; ICD8-codes 390�458; ICD10-codes I00-I52,I60-I99; 100-152, 160-199; ICD10); injuries and suicide (ICD7-codes 800�999; ICD8-codes 800�999; ICD10-codes V01-Y99); and other causes (all other codes).
Footnotes
-
Funding: Danish Heart Association.
-
Conflicts of interest: none declared.
Linked Articles
- In this issue
- Corrections