Article Text

Abstract
Study objective: The quality of mortality statistics is important for epidemiological research. Considerable discrepancies have been reported between death certificates and corresponding hospital discharge records. This study examines whether differences between the death certificate's underlying cause of death and the main condition from the final hospital discharge record can be explained by differences in ICD selection procedures. The authors also discuss the implications of unexplained differences for mortality data quality.
Design: Using ACME, a standard software for the selection of underlying cause of death, the compatibility between the underlying cause of death and the final main condition was examined. The study also investigates whether data available in the hospital discharge record, but not reported on the death certificate, influence the selection of the underlying cause of death.
Setting: Swedish death certificates for 1995 were linked to the national hospital discharge register. The resulting database comprised 69 818 people who had been hospitalised during their final year of life.
Main results: The underlying cause of death and the main condition differed at Basic Tabulation List level in 54% of the deaths. One third of the differences could not be explained by ICD selection procedures. Adding hospital discharge data changed the underlying cause in 11% of deaths. For some causes of death, including medical misadventures and accidental falls, the effect was substantial.
Conclusion: Most differences between underlying cause of death and final main condition can be explained by differences in ICD selection procedures. Further research is needed to investigate whether unexplained differences indicate lower data quality.
- cause of death
- quality control
- medical record linkage
Statistics from Altmetric.com
Mortality data are a cornerstone of epidemiological research and health monitoring. A number of quality problems associated with these data have been identified, ranging from diagnostic difficulties to national bias in data processing.1–8 Inaccuracy in death certification is a major concern.1 In many countries, there are records concerning decedents in other computerised registers, and several studies have made general comparisons between death certificates and hospital discharge data. Goldacre linked cause of death data for the Oxford region to hospital discharge records, and showed that mortality statistics do not necessarily reflect the actual disease pattern among people who die.9 Gittelsohn and Senning, working on Vermont data, also reported considerable discrepancies between hospital discharge diagnoses and the corresponding death certificates, and suggested that the sources of discrepancy be investigated.10
In a previous study,11 we compared Swedish death certificates for 1995 with national hospital discharge records at the “Basic Tabulation List” level (an aggregated list with about 230 groups). We found that the main condition from the patient's final hospital discharge record (referred to as “the final main condition” below) and the underlying cause of death selected by Statistics Sweden on the basis of the original death certificate (“the original underlying cause of death” below) matched in only about 46% of the cases. We argued, however, that many of these differences could be explained by differences in the ICD definitions of “main condition” and “underlying cause of death”, and in the procedures for reporting and classifying them.
The main condition, as defined in Ninth Revision of the International Classification of Diseases (ICD-9),12 is “the main condition treated or investigated during the relevant episode”, while the underlying cause of death is “(a) the disease or injury which initiated the train of morbid events leading directly to death, or (b) the circumstances of the accident or violence which produced the fatal injury”. This difference in definitions is manifested in the fact that the ICD instructions for the selection of the underlying cause of death differ from those for the selection of the main condition. Accordingly, there are many cases in which one would expect the original underlying cause of death to differ from the final main condition (table 1). For example, if the final main condition is a complication of the original underlying cause of death, then the two conditions are legitimately different while at the same time medically compatible.
Relations between differing final main conditions and original underlying causes of death
However, there are cases that are not as easily explained. If, for example, the original underlying cause of death seems to be a complication of the final main condition rather than vice versa, then the difference between the conditions cannot be explained by the ICD definitions and selection procedures.
In this study, we aim first at quantifying the compatibility between the original underlying cause of death and the final main condition. In other words, we seek to determine how often differences between the original underlying cause of death and the final main condition can be explained by differences in the relevant ICD definitions and selection procedures.
However, we also wish to explore the importance of hospital discharge data that are not reported on the death certificate. Here, we measure how often information that is present in the hospital record but omitted from the death certificate would have influenced the selection of the underlying cause of death.
METHOD
Material
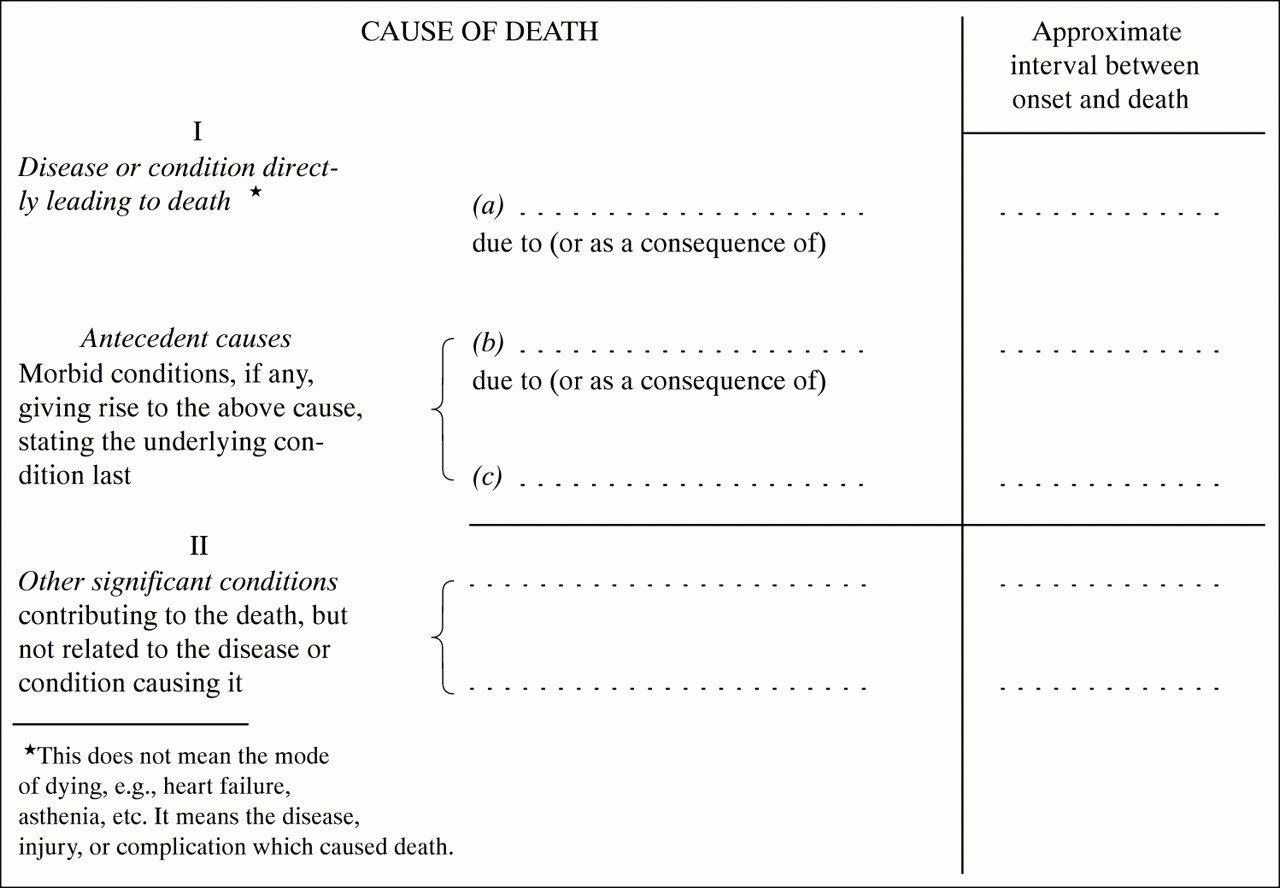
We obtained cause of death data for 1995 from the Swedish National Cause of Death Register, which covers all deaths of Swedish residents, whether they occur in Sweden or abroad. The medical part of the Swedish death certificate was based on the international form specified in the international (English) version of ICD-9 (fig 1), and the causes of death were coded centrally at Statistics Sweden according to the ICD instructions.12 Since 1987, Statistics Sweden has used ACME, a software developed by the National Center for Health Statistics, USA, to select the underlying cause of death.13 The 1995 record format permitted a complete registration of all reported conditions. The total number of deaths in 1995 was 93 910.

The international form of medical certificate of cause of death. After The Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death, ninth revision.
Hospital discharge data were obtained from the Swedish Hospital Discharge Register. This register is a compilation of all individuals' hospital discharge records, collected electronically first at the regional level by the local health administrative authorities, and then forwarded to the National Board of Health and Welfare. According to the Board's estimates, about 99% of all hospitalisations are reflected in this register.14 Discharges from nursing homes are not reported. In contrast with the causes of death in the national mortality register, the hospital discharge diagnoses are coded locally at each hospital, generally by the physician responsible for the discharge. The Board of Health and Welfare, however, performs extensive checks on the data. In 1995, Swedish hospitals used the KS87 adaptation of ICD-9.15 The Hospital Discharge Register contains one entry for each episode of hospital care, with each entry indicating the personal identification number (that follow all Swedish residents throughout their lives), and including particulars of the hospital department and the hospitalisation, as well as a main condition, a maximum of five additional conditions, the external cause in cases of injury, and codes for any surgery performed.
By matching the personal identification numbers, we extracted individual data for all hospital discharges within one year prior to death. The resulting database comprised 224 794 hospital discharges (69 818 people), corresponding to almost 75% of all deaths in 1995. Of these, 39 872 persons (43% of all deaths) died in the hospital.
Software
We used ACME both to analyse the compatibility between the original underlying cause of death and the final main diagnosis, and to estimate the importance of hospital discharge data not reported on the death certificate. ACME has been used in routine production of US mortality statistics since 1968, and is often regarded as the de facto international standard for the selection of underlying cause of death.13,16 Starting from a set of ICD codes that corresponds to the conditions reported on the death certificate, ACME selects an underlying cause of death according to the rules and guidelines in the ICD.12 The selection procedure contains two steps. Firstly, ACME identifies the starting point in the physician's description of the train of events leading to death, entered in Part I of the death certificate. This entails testing whether a condition A can be due to a condition B. Secondly, ACME checks whether this starting point is itself an obvious consequence of some other condition, and searches for such underlying causes in both Part I and Part II. While Part II is intended for conditions that contributed to the death but are not related to the events described in Part I, the underlying cause is still sometimes entered here.
Basic Tabulation List (BTL) used in analyses
As we wished to avoid minor differences of little practical importance, we made all analyses at the BTL level. The three digit BTL is a cause of death shortlist consisting of about 230 categories, published in volume 1 of ICD-9. It corresponds fairly well with the level of detail at which mortality statistics are generally analysed. The BTL groups do not, however, cover all causes of death and thus cannot be used for calculating totals. For this reason, we used Statistics Sweden's extended version of the BTL, in which residual groups have been added throughout the list.17
Compatibility between final main condition and original underlying cause of death
To assess the compatibility between the final main condition and the original underlying cause of death, we constructed “test certificates” with only two diagnoses each. On the top line (as immediate cause of death), we placed the final main condition, and on the line below we entered the original underlying cause of death. This is the equivalent of stating that the final main condition is caused by the original underlying cause of death. We then ran the “test certificates” through ACME and checked whether ACME would accept the stated relation. When accepted, we deemed the final main condition and the original underlying cause of death to be medically compatible. When not accepted, we considered them incompatible.
Similar analyses could, of course, be made for the additional conditions reported to the hospital discharge register. However, we decided to restrict our analysis to the final main condition, as this was presumably dominant throughout the patient's final hospitalisation.
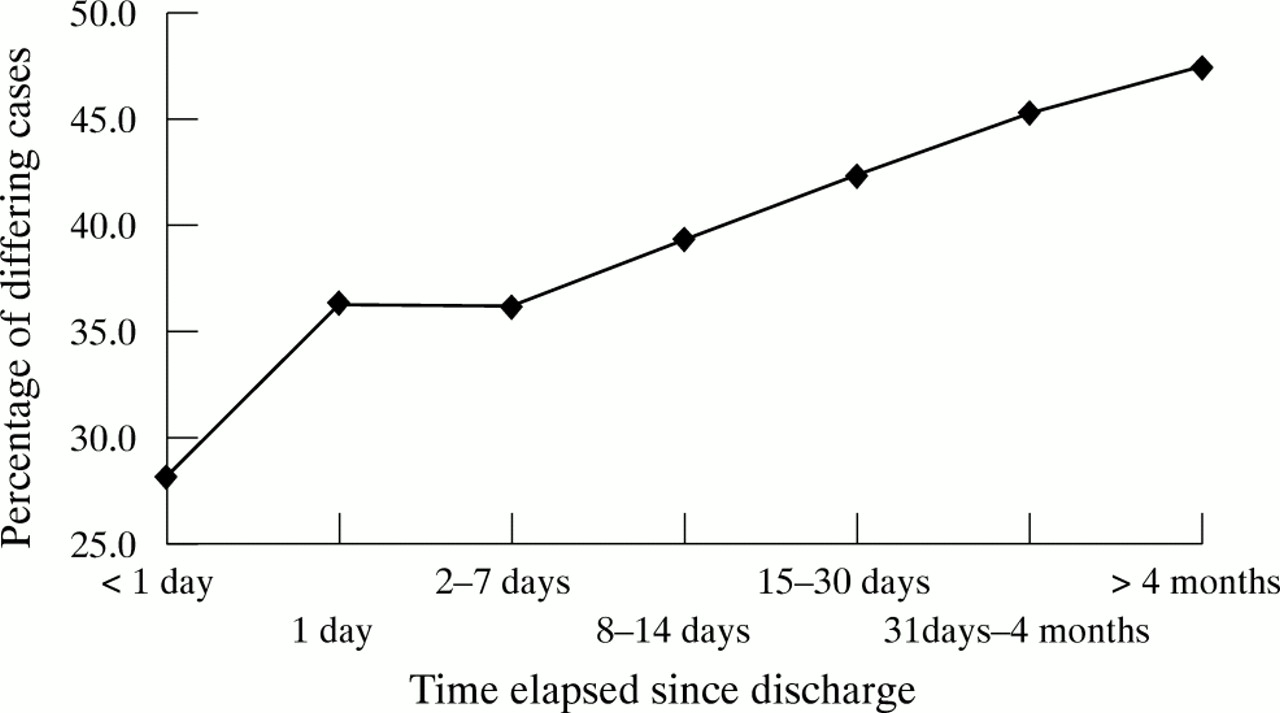
To obtain a general overview, we first calculated the number of incompatible cases per ICD chapter. Next, we analysed the percentage of incompatible cases by the time elapsed since discharge, as differences between original underlying cause of death and final main condition are more likely to be legitimate the longer the interval between discharge and death. For example, new conditions might develop after discharge, and previously innocuous conditions might begin to have serious consequences.
We decided to conduct the more specific analyses for hospital deaths only, as our data are less complete for deaths occurring after discharge. Previous studies9–11 have shown that some final main conditions are less likely than others to appear on the death certificate. Analogously, we identified the particular original underlying causes of death that most often were incompatible with the final main conditions.
Importance of hospital discharge data not reported on the death certificate
We constructed a second set of “test certificates” to check whether data present in the hospital discharge register, but not reported on the death certificate, would influence ACME's selection of the underlying cause of death. For this analysis, which aimed at identifying the initial step in the course of events that ultimately lead to death, it seemed plausible to take into consideration not only the final main condition, but also the additional hospital discharge conditions. The main condition is, per definition, predominant during the hospitalisation, but it might very well be caused by something reported as an additional condition.
Here, we retained all conditions as reported on the original death certificate, but added main and additional conditions retrieved from the final hospital discharge record. To avoid making any unsubstantiated assumptions as to the importance of these conditions, we placed them last in Part II of the “test certificate”, that is, under “conditions contributing to the death, but not related to the disease or condition causing it”.12
These additions would thus influence the selection of the underlying cause of death in two circumstances only. The first is when one of the added conditions is “more specific” than the original underlying cause of death. For example, if the original underlying cause of death is “cerebrovascular disease” and the hospital discharge register has “cerebral haemorrhage”, ACME will consider the latter condition as the more specific, and will assign it as the new underlying cause of death. The second case concerns “obvious consequence”, that is, did the train of events leading to death obviously start with one of the added conditions? An example is the case where the original underlying cause of death is peritonitis but a diagnosis of ruptured appendicitis is mentioned in the hospital discharge register. Here appendicitis will be ACME's newly assigned underlying cause of death, as the peritonitis was in all probability attributable to the appendicitis.
Furthermore, we scanned the hospital discharge register for information on recent surgery or recent injuries. The ICD rules lay great emphasis on surgery or injuries during the last four weeks of a patient's life, and many common secondary conditions such as pneumonia and heart failure are considered to be complications of surgery or injuries that occurred within those four weeks.12 When we found a recent operation or injury that was not mentioned on the original death certificate, we reclassified the multiple conditions, taking the surgery and injury into account.
The second set of “test certificates” was then processed by ACME. When analysing the results, we followed the same basic steps as was done when comparing original underlying cause of death and final main condition. Thus, we first computed the number of changes to the original underlying causes of death by ICD chapter. To test our assumption that both main and additional conditions should be considered, we also specified the origin of the newly assigned underlying causes of death. We then listed the particular original underlying causes of death that ACME would most often replace with another condition. We distinguished between the two types of such replacements: where ACME had found a “more specific” description of the original underlying cause of death, and where ACME considered the original underlying cause of death an “obvious consequence” of another condition.
RESULTS
Compatibility between final main condition and original underlying cause of death
In over one third of cases in which the original underlying cause of death differed from the final main condition, the conditions were also medically incompatible (table 2). We found the highest proportions of incompatibilities for deaths originally certified as attributable to symptoms (men 84% of deaths within one year from discharge, women 83%), and the lowest for conditions originating in the perinatal period (men 14%, women 31%), which, however, is a very small group. Most large diagnostic groups displayed only small differences between the sexes.
Differences and incompatibilities between original underlying cause of death and final main condition, Basic Tabulation List level, by ICD Chapter of original underlying cause of death and sex. All deaths within one year from discharge, Sweden, 1995 (n=69 818)
The overall results were not worse for the older age groups (data not shown). Incompatibilities between original underlying cause of death and final main condition were most common among people 15–44 years (51% of deaths within one year following discharge), and lowest in the 65–74 age group (34%).
The frequency of incompatible conditions increases with time elapsed since discharge (fig 2). For hospital deaths, ACME considered the original underlying cause of death incompatible with the final main condition in 28% of cases in which the two conditions differed from each other. For deaths occurring at least four months after discharge, 47% of the cases were regarded as incompatible.
{kind=link}
{kind=link}
Original underlying causes of death medically incompatible with the final main condition, in percentage of all cases in which the two conditions differ at BTL level, by time elapsed since discharge. Deaths within one year after discharge from hospital, Sweden, 1995 (n=38 023).
We found higher figures for some specific groups of the BTL (table 3). For those BTL groups that contain at least 30 reported hospital deaths, the highest proportions of incompatible statements were those for signs, symptoms and ill defined conditions (100% of all differing cases), malignant neoplasms of other and unspecified sites (79%), and other and unspecified neoplasms (76%).
The 10 original underlying causes of death most often incompatible with the final main condition, Swedish extended Basic Tabulation List, hospital deaths, Sweden 1995 (n=39 872)
Importance of hospital discharge data not reported on the death certificate
When we added all additional information from the hospital discharge register to the original certificate (main condition, additional conditions, information on recent surgery and injury), ACME assigned a new underlying cause of death in 4225 out of the 39 872 cases of hospital deaths (table 4). The newly assigned underlying cause of death was “upgraded” from contributory cause of death to underlying cause in 23% of the 4225 cases. In 77%, the newly assigned underlying cause of death had not been mentioned on the original death certificate but was taken from the hospital discharge register. It was derived almost as often from the additional discharge conditions as from the main condition.
Changes in original underlying cause of death when all hospital discharge data* are added to the original death certificate: Origin of the newly assigned underlying cause of death. Hospital deaths, Sweden 1995 (n=39 872)
About 11% of deaths originally classified to a BTL group for “unspecified” (less informative) diagnostic statements were changed when main and additional conditions were added to Part II, and replaced by a “more specific” diagnosis in the same broad diagnostic group (table 5). For example, in 56% of hospital deaths reported as attributable to unspecified cerebrovascular disease, the hospital discharge register provided a more precise description of the cerebrovascular condition. However, for most diagnostic groups, the number of such improvements in specificity was small.
Original underlying causes of death often replaced by more specific underlying causes in the same broad diagnostic group when all hospital discharge data* are added to the original death certificate, the ten groups most often affected and total. Swedish extended Basic Tabulation List, hospital deaths, Sweden 1995 (n=39 872)
ACME considered the original underlying cause of death an obvious consequence of another condition in 7% of all hospital deaths (data not shown). This sometimes meant a sharp increase in the death rates (table 6). For example, misadventures during medical care showed an almost 10-fold increase (+962%), alcoholism increased by 467%, bronchitis, emphysema and asthma by 66%, and accidental falls by 58%. It should be noted, though, that with the exception of accidental falls, these percentile increases are based on fairly small numbers.
The 15 largest changes in original underlying cause of death rates when all hospital discharge data* are added to the death certificate, examples. Changes from unspecified to more specific subcategories of the same broad diagnostic group excluded. Swedish extended Basic Tabulation List, hospital deaths, Sweden 1995 (n=37 640)
DISCUSSION
Compatibility between final main condition and original underlying cause of death
In our previous study,11 we found that the final main condition differed from the original underlying cause of death in 54% of the cases. According to ACME, over one third of these are incompatible diagnostic statements, as the final main condition cannot be seen as a complication or consequence of the original underlying cause of death (table 2). The original underlying cause of these incompatible cases was often symptoms and other ill-defined conditions, unspecified malignant neoplasms, an injury of undetermined intent, unspecified cerebrovascular and other circulatory diseases, unspecified accidents, and unspecified psychoses (table 3). Few epidemiologists would dispute the statement that deaths assigned to these groups, with the possible exception of cerebrovascular deaths,18 are highly problematic. Injuries of “undetermined intent” may contain suicides and accidents, as well as homicides, and unspecified circulatory conditions occur as the final complication of almost all other serious conditions. Also, psychoses seldom cause death on their own but rather in interaction with other conditions, and obviously very little is known about the mechanisms underlying deaths classified under ICD categories for “symptoms and other ill-defined conditions”. This lends some support to the suggestion that incompatible diagnostic statements might indicate a quality problem.
Key points
-
Quite often the underlying cause of death and the main condition from the last hospital discharge record do not coincide.
-
In a Swedish material, over one third of the differences could not be explained by ICD definitions and selection procedures.
-
Can unexplained differences serve as a data quality measure of mortality statistics? This should be investigated.
Importance of hospital discharge data not reported on the death certificate
Adding hospital discharge conditions to Part II of the original death certificate will result in ACME assigning a new underlying cause of death only if there has been an indisputable mistake in certification, and we saw fairly few such changes (11% of deaths within a year of discharge). For some causes of death, though, the effect of this was dramatic (table 6). The great increase in deaths attributable to misadventures during medical care is noteworthy, not least of all because other recent studies show that medical mishaps are grossly underreported.19,20 Another interesting finding is that even recent accidental falls and fractures had often been omitted from the original death certificate, which concurs well with the findings of several quality studies.21,22
One quarter of the changes made implied the substitution of a more specific condition within the same broad BTL group (table 5). This indicates that the diagnostic information is often less precise on death certificates than in the hospital discharge register. One explanation for this may be that physicians often consult the ICD manuals when reporting a patient to the hospital discharge register, thus making use of all the details allowed by the ICD. When writing death certificates, on the other hand, physicians usually do not consult the ICD and thus tend to fall back on less precise everyday clinical language.
When ACME assigned a new underlying cause of death obtained from the hospital records, it was derived from the additional discharge conditions almost as often as from the main condition (table 4), which implies that both main and additional conditions should be considered.
Sometimes a condition originally reported as a contributory cause of death was upgraded to underlying cause of death. This was often due to the effect of additional information about recent surgery. ACME considered the original underlying cause of death a complication of surgery, and the condition necessitating the surgery was assigned as the new underlying cause of death. This testifies to the importance of reliable information on recent surgery.
Limitations of the study
An incompatibility between the final main conditions and the original underlying cause of death naturally does not necessarily mean that the death certificate is erroneous. There are obviously more factors than ICD selection rules that may explain apparent incompatibilities. Firstly, the hospital discharge register has quality problems of its own. It should be noted, though, that according to a Swedish study, hospital discharge data are fairly reliable on the aggregated level.23,24 Secondly, by testing whether the final main condition is a plausible consequence of the original underlying cause of death, we might reject some perfectly correct certificates for persons suffering from multiple, but aetiologically unrelated conditions. Thirdly, the ACME “decision tables” that specify acceptable relations between medical conditions are not perfect.25 Fourthly, the time elapsed since discharge from the hospital may account for many of the incompatibilities. After discharge, the patient is perhaps treated by another physician who sees the case in a different light from the attending physician at the hospital, and new conditions might develop after the last hospital stay. Inversely, comparing registers will miss a number of defective death certificates. For example, register comparisons will not identify cases in which the original underlying cause of death and the final main condition are the same, but unfortunately both wrong.
Further research
Our findings indicate a possible error in certification for one out of five deaths in the study population. If confirmed by future research, this reflects a substantial quality problem. Even so, our figures are comparatively low compared with the error rates reported in many previous quality studies.26–32 Our lower error rates may indeed indicate limited possibilities for detecting defective death certificates by comparing the original underlying cause of death with routinely collected hospital discharge data. However, they may also illustrate the lack of international standards for cause of death quality research. Possibly, a quality measure based on a widely recognised software like ACME could contribute to standardisation and comparability.
However, to design such a quality measure and to judge its merits and drawbacks will require further research. For example, linking death certificates to hospital discharge data will hardly help if the deceased was not hospitalised within a reasonable period of time prior to death. Therefore, we need more understanding about the influence of the time factor. The possibility of using other sources of medical information, for example non-institutional care data, should also be explored.
The priority, however, should be to check the outcome of the comparisons made in this study with the corresponding hospital records, including necropsy reports. By doing so, an estimation could be made of both the likelihood that incompatible diagnoses do in fact conceal a quality problem, and of the risk of missing seriously defective death certificates. We would also be able to assess how often the hospital discharge record rather than the death certificate is wrong, and how often an apparent incompatibility is in fact attributable to an error in the ACME decision tables. In all this, special attention should be paid to the core data of mortality statistics, namely, avoidable and otherwise premature deaths.33,34
Using the medical records to check findings would also provide us with a better understanding of the circumstances in which physicians tend either to report an incorrect cause of death diagnosis or to omit important steps in the series of events that eventually lead to death. Such knowledge would also be helpful for training physicians in filling out death certificates, as well as for designing quality assurance programmes for official mortality statistics.
Acknowledgments
Funding: this study was made possible by a grant from the Vårdal foundation (project number V97 393), and by the support from the National Board of Health and Welfare and from Statistics Sweden.
Conflicts of interest: none.