Article Text

Abstract
STUDY OBJECTIVES (1) To identify and to categorise the various city indicators that are related to health levels; (2) to demonstrate the extent of the influence on health of these categorised health determinants; and (3) to demonstrate both the interactive associations among the health determinants and the magnitude of influence of each health determinant on the people's health.
DESIGN By using city statistics of study areas, the health index and health determinant indices were formulated. The extent of influence of health determinants on the health index was examined by regression analysis; the interrelations between the health determinants and the health index were examined by correlation analysis.
SETTING All the administrative units in Japan with populations more than 100 000 were selected as study areas to analyse the relation of health and health determinants.
MAIN RESULTS The nine health determinant indices used—healthcare resources, preventive health activities, environmental quality, housing, urban clutter, local economy, employment, income, and education—explained 51.6% of the variances of the health index as a whole in the cities studies. The health determinant indices showed interrelations with each other, in addition to individual health determinant indices having a high correlation with the health level index of the population.
CONCLUSIONS Both individually and collectively the health determinants are closely related to the health status of a population and individual determinants interact with each other. Simultaneous analysis of the interrelations among health determinants and health status would contribute to widen integration oriented perspective in policy interventions based on collaboration between different sectors of society.
- indicators
- health determinants
- Healthy Cities
Statistics from Altmetric.com
Cities provide living conditions for their residents in complex ways. Health levels, which are largely dependent upon residents' living conditions and lifestyles, must be dealt with in terms of a complicated interaction of a variety of health determinants—physical, economic, and social—in residential environments.
The determinants of health are defined by the World Health Organisation (WHO) as “the range of personal, social, economic and environmental factors which determine the health status of individuals or populations.” WHO has also noted that “the factors which influence health are multiple and interactive.” Health determinants are considered to include such factors as income and social status, education, employment and working conditions, access to appropriate health services, and physical environments.1-4
In order to adopt and implement effective city health policies that will improve the health status of residents, it is necessary to deal collectively with a variety of health determinants from an integration oriented viewpoint. The Healthy Cities Project is one of the most popular frameworks being used to realise comprehensive health policies from this viewpoint.5-7
To implement Healthy Cities projects in actual situations, it is helpful if collaboration among various sectors of society, which is considered a key element of urban health management, can use common databases and if information can be shared among the various government departments and other sectors of society that are concerned with health issues.8 The availability of common databases also provides a platform for evidence-based decision making.9
To show the relations between various health determinants and the health status of cities is regarded as necessary in order to provide a common database for use in understanding and explaining the current diversity of health statuses within a given population. Thus, we have analysed diverse health determinants and their interrelations by using a number of indicators of residential environments and living conditions in all the cities in Japan having a population of more than 100 000. The objectives of this study were: (1) to identify and to categorise, in accordance with the concept of health determinants, the various city indicators that are related to health levels; (2) to demonstrate the extent of the influence on health of these categorised health determinants; and (3) to demonstrate both the interactive associations among the health determinants and the magnitude of influence of each health determinant on the people's health.
Methods
STUDY AREAS
In Japan, local governmental units are defined by the Local Autonomy Law (1947) to be one of the following: Tokyo special ward cities, cities designated by ordinance, cities, towns, and villages. The cities designated by ordinance are further divided into wards for purposes of their administrative services. Many statistics are collected on the basis of these local authority administrative units. In 1990, there were 311 local administrative units with populations more than 100 000. These consisted of 21 of the Tokyo special ward cities, 93 wards of the 11 cities designated by ordinance, and 197 cities.
In this study, we dealt with each of these 311 local administrative units as a “city unit,” in accordance with how they are commonly regarded, and we used statistics relating to them throughout the study. The population of the individual units of this study ranged from 100 811 to 829 455; the median and average were 178 484 and 225 943, respectively. The sum of the units' populations was 70 268 396, which amounted to 73.5% of the total population of all of the cities in Japan.
FORMULATION OF THE HEALTH INDEX
Thirty five health indicators (see table 1) were used to formulate a health index representing the health status of the population. The indicators were computed by applying age adjustment and other standardisation techniques to statistics of the 1990 Population Census of Japan10 and of the Vital Statistics Japan for each year from 1988 through 1992.11 Vital statistics were used by summing up five consecutive years of statistics of individual city units. Then, factor analysis of the 35 health indicators was performed using a varimax operation. The factor score of a factor that explained the greatest variance among the health indicators was taken as the health index. In addition, Pearson correlation coefficients between the health index and individual health indicators were calculated.
Pearson correlation coefficients of health indicators and health index
FORMULATION OF THE HEALTH DETERMINANT INDICES
Seventy one indicators (see table 2) from a variety of fields were used to formulate health determinant indices. Indicators were selected and calculated by using statistics from the following sources: 1990 Population Census of Japan,10 1993 Housing Survey of Japan,12 1991 Establishment Census of Japan,13 1991 Indicators of Citizens' Income,14 1989–1991 Annual Reports concerning Fires,15 1990 Statistics of National Health Insurance,16 1990 National Consumption Survey Japan,17 1993 Yearbook of Cities in Japan,181990 Meteorological Data by Satellite Observation,19 1990 Forestry Census,20 1990 Report on Atmospheric Monitoring Stations,21 1993 Basic Statistics for Community Medical Care,22 and 1990 Indices of Municipalities.23
Pearson correlation coefficients of healthcare, urban residential, and socioeconomic indicators and health determinants indices
Excluded from this analysis were indicators of the urban basic infrastructure—such as water supply and electric power supply—that are already sufficiently provided in the study areas and that differ little among cities, and that thus are marginal variables for explaining health inequalities among the study areas.
The selected 71 indicators were divided into nine categories of health determinants in accordance with the general concept of health determinants.1 2 4 24
Principal factor analysis was then performed to obtain one factor from each individual category of health determinants. The factors were selected by considering that the eigenvalue of the correlation matrix should be more than 2, and that the selected factor should explain at least 30% of the variance within its individual set of indicators. Calculations showed that one factor in each individual category satisfied the above mathematical criteria, and that the factors represented individual aspects of health determinants. Also, Pearson correlation coefficients between health determinant indices and indicators of the concerned categories were calculated.
ANALYSIS OF THE EXTENT OF HEALTH DETERMINANTS' INFLUENCE ON HEALTH
To determine the health determinants' extent of influence on the health index, we performed regression analysis using a forward procedure. The health index was used as a dependent variable. Nine health determinant indices were categorised into three groups: (1) healthcare, (2) residential environment, and (3) socioeconomic status. Then the indices of the three groups were included as independent variables one after another. The three individual groups consisted of the following indices: (a) healthcare related (HC) indices: healthcare resources and preventive health activities; (b) urban residential environment (ENV) indices: environmental quality, urban clutter, and housing; and (c) socioeconomic status (SES) indices: local economy, employment, income, and education. Also, because the demographic characteristics of aging influence health indicators in various ways, five demographic indicators were analysed by factor analysis and one factor that was derived as an aging index was included as an independent variable of a fourth group (AG: aging) used to estimate the health index. The first three groups were put into the model in six different orders. The orders were (1) HC, ENV, SES; (2) HC, SES, ENV; (3) ENV, HC, SES; (4) ENV, SES, HC; (5) SES, HC, ENV; (6) SES, ENV, HC. The adjusted coefficient of determination (r 2) was calculated for each step (each step adding one new group) of each individual model. Finally, the aging index (AG) was added to the model, and the adjusted coefficient of determination (r 2) was calculated. The final adjusted coefficient of determination by health determinants indices and the aging index was calculated so as to show the variations in the health index as explained by the set of health determinants defined in this study. This series of calculations of the adjustedr 2 of regression analysis also was performed by setting male and female age adjusted mortalities as dependent variables.
ANALYSIS OF THE INTERRELATIONS BETWEEN THE HEALTH DETERMINANTS AND THE HEALTH INDEX
Correlation analysis was performed to show the interrelations among health determinants and the relation between the health determinants and health. Pearson correlation coefficients were calculated using associated probability. In addition, Pearson correlation coefficients were calculated between the health index and each of the nine health determinant indices—health resources, preventive health activities, environmental quality, urban clutter, housing, local economy, employment, income, and education—and among the nine health determinant indices. The results have been presented in a chart to show the interrelations among these indices.
Results
key points
-
Nine health determinant indices—healthcare, preventive health, environment, housing, urban clutter, local economy, employment, income, and education—were formulated.
-
Individual health determinants had a high correlation with the health level of the population.
-
Health determinant indices showed interrelations with each other.
-
Simultaneous analysis of taking various health determinants at once visualised dynamics of health and health determinant indices.
-
An integration oriented perspective based on an understanding of the relations between health and health determinants is useful.
THE HEALTH INDEX
The first factor that had an eigenvalue of 10.9 and that explained 31.2% of the variance among 35 health indicators was taken as the health index. Health indicators with a statistically significant (p < 0.01) correlation with the health index are listed in table 1, along with their Pearson correlation coefficients; 26 indicators had a significant correlation with the health index.
THE HEALTH DETERMINANTS
The following nine factors were selected as health determinant indices: healthcare resources, preventive health activities, environmental quality, housing, urban clutter, local economy, employment, income, and education. Table 2 shows the statistically significant Pearson correlation coefficients of the healthcare, urban residential, and socioeconomic indices that we used for this study. The individual health determinant indices represented the following aspects: (1) healthcare resources: adequate healthcare resources exist; (2) preventive health activities: preventive health activities are conducted; (3) environmental quality: good quality physical environment; (4) housing: new, good quality housing with exists; (5) urban clutter: urban area that is densely crowded and congested; (6) education: the population is highly educated in terms of both level and quality; (7) employment: good employment opportunities are available; (8) income: the population has a high income; (9) local economy: local business is growing and local financial conditions are good.
RANGE OF INFLUENCE OF HEALTH DETERMINANT INDICES
Table 3 shows the adjusted coefficient of determination (r 2) as calculated for each step, adding the HC, ENV, and SES indices into the regression model so as to predict the health index. The adjustedr 2 represents the explained variances among individual dependent variables in terms of the defined set of independent variables. Adding one of the three sets of health determinants—that is, either HC, ENV, or SES, according to the order of adding dependent variables—resulted in an absolute increase in the adjusted r 2. However, the range of the increase of the adjustedr 2 that resulted by adding one particular set shows the extent of the contribution of the individual areas of health determinants. Additional health index variances that were explained by the healthcare related indices ranged from 3.7% to 14.2%; the urban residential indices ranged from 13.4% to 23.8%; and the socioeconomic indices ranged from 24.0% to 34.5%.
Explained variances of the health index by sets of health determinants
The adjusted r 2 of the model with nine health determinant indices was 0.516, and that of the model with nine health determinant indices and the aging index was 0.548.
The results with the male and female age adjusted mortalities and with the adjusted r 2 of the model with the nine health determinant indices as independent variables were 0.590 and 0.483, respectively. The results with the model of the nine health determinant indices and the aging index and with the adjustedr 2 were 0.669 and 0.553, respectively. For male age adjusted mortality, the contribution of SES was 0.348; for female age adjusted mortality the contribution of SES was 0.182. The latter was smaller than the contribution of ENV to female age adjusted mortality.
THE INTERRELATION BETWEEN HEALTH DETERMINANTS AND THE HEALTH INDEX
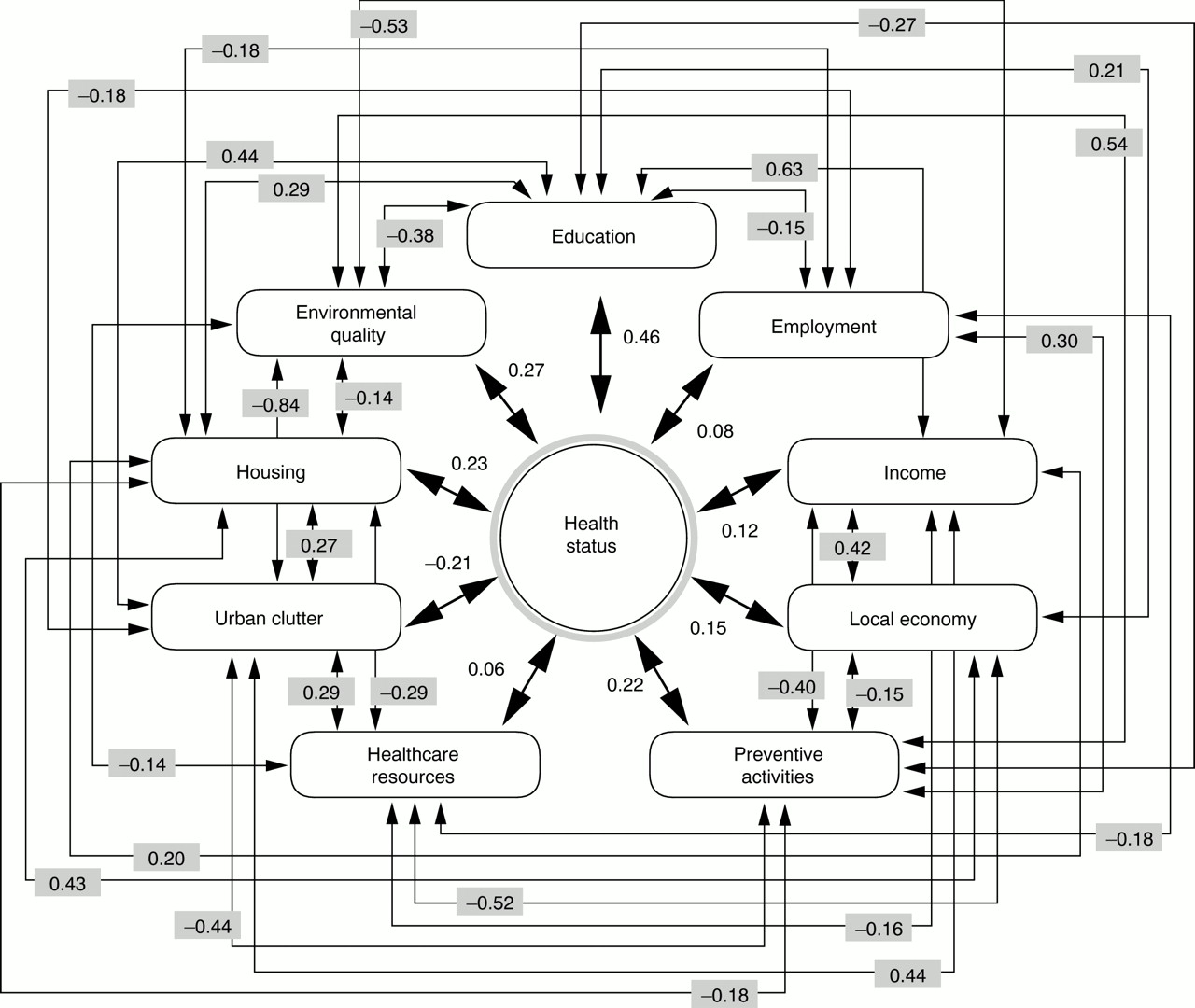
Figure 1 shows the interrelation between the health determinants and the health index.

{kind=link}
Interrelation between the health determinants and the health status. “Health Status” is represented by the health index. “Healthcare resources”, “Preventive activities”, “Environmental quality”, “Housing”, “Urban clutter”, “Education”, “Employment”, “Income”, “Local economy” individually represent health-determinant factors. Fine thread arrows indicate pairs of health determinant indices with statistically significant correlation with Pearson correlation coefficients. Thick thread arrows show relation between health determinant indices and the index of health with Pearson correlation coefficients.
Pearson correlation coefficients between health determinant indices each other showed that 29 pairs of the 36 pairs of indices had a significant correlation (p < 0.05). Pearson correlation coefficients between the health index and the health determinant indices showed a significant correlation between the health index and preventive health activities, environmental quality, housing, urban clutter, education, income, and local economy.
Discussion
This study showed, firstly, that the nine health determinants used here explained more than one half of the variances of the health index as a whole in the cities studied; secondly, that the health determinants showed interrelations with each other, in addition to individual health determinants having a high correlation with the health level of the population.
The health index that we used in this study represented a greater proportion of variances of the selected populations' health indicators. Results with male and female age adjusted mortalities as dependent variables also showed that one half of the variances of the health indices were explained by selected health determinant indices.
It was considered that for the obtained statistical result to have ar 2 greater than half was because of the adoption of variables from various fields including healthcare, urban residential, and socioeconomic conditions, in accordance with the concept of health determinants taken with wide perspective that are found in living conditions. The contribution of wide range health determinants to the health status of the population supported the importance of the integrative approach of wide range various administrative fields in the development of health policies and in collaboration among various sectors of society.
Each individual health determinant had a statistically significant correlation with from six to eight other health determinants. These interrelations were not confined to determinants within only one of the three categories of health determinants—healthcare, urban residential, or socioeconomic—but extended to determinants in the other two categories as well. We concluded that the interrelations among the indices formed both a complicated interaction of varied health determinants and a causal web-like relation between environmental factors and the health status in the cities studied. We also concluded that the obtained interrelation representing the dynamics of health determining mechanism reinforced the importance of comprehensive intervention in the implementation of Healthy Cities projects.
Socioeconomic conditions defined a certain proportion of the variances in health status. The analysis showed high correlations between the individual health determinants of the socioeconomic category—education, employment, income, and local economy—and the health of the population. It has been reported that socioeconomic status is closely related to health levels, including relations between income inequalities and differences in mortality,2 24-27and between variations in educational levels and differences in mortality.28 29 Thus, the adoption of programmes to improve socioeconomic conditions and to reduce socioeconomic inequalities is necessary in order for Healthy Cities projects to achieve tangible results.
Variables concerning residential environments also explain a certain proportion of the variances in health levels. Our analysis showed high correlations among the individual health determinants of the urban residential environment category—environmental quality, housing, and urban clutter—and the health of the population. With regard to the residential environment, the adjustedr 2 for explaining variances of female age adjusted mortality was larger than that of men, with the difference being 0.107. It has been reported that a greater proportion of women than men expresses demands to improve the residential environment.30 It is likely that the gender differences in our study results reflect the fact that women spend more time in their living places than men do, and that therefore they might be greatly influenced by their residential environment.31 It might therefore be appropriate to suggest that Healthy Cities projects should largely respond to the needs and demands of the female population in efforts to improve residential environments.
We formulated an index of environmental quality to reflect less air pollution, relatively good access to greenery, and the availability of longer hours of sunlight at individual residences. In this regard, the levels of nitrogen oxide in the air reflect existing levels of air pollution.32 In the areas that we studied, automobiles were the main source of nitrogen oxide air pollution.33Access to greenery in city areas reflected high quality living environments that included enough open space and parks, as well as land use zones limited exclusively to housing. Longer hours of sunlight also characterised high quality residential areas. Good urban planning schemes designed to promote good residential areas have enabled individual locations to have high quality residential space. In Japan, land use zoning is specified by the City Planning Law for the following specific categories: exclusive residential building districts, residential districts, neighbourhood commercial districts, commercial districts, quasi-industrial districts, industrial districts, exclusive industrial districts. Within exclusive residential districts, construction of better equipped housing has been encouraged, and in such areas the housing environments are generally more supportive of health.34 35 It has been reported that the health of people in localities having a larger proportion of well prepared exclusive housing areas tends to be generally higher than in localities with a smaller proportion of such housing areas.36 A study of a community in the United States also revealed that neighbourhood social environments impact health independent of the socioeconomic conditions of individuals and communities.37 We concluded that it is essential to develop health planning and urban planning in concert in order for Healthy Cities projects to be effective.
The index of preventive health activities reflected the positive preventive health activities, including participation in health check ups, in communities. Participation in health check ups, which constituted one element of the index, represented not only the proportion of the population that completed screening programmes, but also showed participation in health education programmes, because health check up programmes conducted at public health centres basically aim to provide participants with information about primary means of preventing detrimental health factors. Lifestyle related indicators such as the percentage of smokers were not used in this analysis. Changes in the lifestyles of people are considered as an appropriate intermediate health outcome.38 Systematic collection and comparison at the municipal level of standardised data relating to people's lifestyles and to changes thereof are necessary both to analyse lifestyles as health determinants and to evaluate the intermediate health outcomes of health promotion activities. We have concluded that more indicators representing the process of health promotion activities should be developed and made possible for standardised comparison in order to increase the explanatory value of such analyses.
This analysis is based on the data relating to cities in Japan in 1990. During this studied period, per capita GDP was compatible with 23 734 US dollars39; percentage of workers of primary, secondary, and tertiary industries were 7.2, 34.1, and 58.7.39Enrolment to primary education was 100% and enrolment to tertiary education among the corresponding age group was 32%.40Life expectancy at birth was 76.04 years for male and 82.07 years for female41 and infant mortality was 4.6 per 1000 live births in 1990.11
The presented figures of association between health and health determinants might vary from country to country. Also, those figures might show different features according to their developmental stages during several decades of time. In addition, a set of indicators could be devised and adapted to fit the particular situations of various countries if it were desired to apply the analysis to cities in countries other than Japan. However, we concluded that it is universally important to select wider range determinants of health and to recognise the existence of causal web-like interrelations between health determinants and health status. We have also concluded that these kinds of analyses have been shown to be necessary as tools for evidence-based decision making in the formation of comprehensive health programmes such as Healthy Cities projects.
Appropriate indicators to be analysed should be selected for the individual set of cities analysed. For example, statistics concerning water supplies and power stations were not used in this study, because at present such resources are uniformly available in virtually every municipality in Japan. However, these indicators were in fact significant health determinants in Japan only several decades ago. Thus, the indicators selected might need to differ among different countries and regions because the variances of indicators can differ among the population units of different countries and regions. Related to this, the relation between GDP and health by country has changed over time in accordance with the overall increases in health status and economic conditions.40
In conclusion, the nine wide ranged health determinants that we studied—healthcare resources, preventive health activities, environmental quality, housing, urban clutter, local economy, employment, income, and education—as a whole explained more than 50% of the variances in the index of people's health. Both individually and collectively the health determinants are closely related to the health status of a population. In addition, the individual determinants interact with each other. Simultaneous analysis of the interrelations among health determinants would help evidence-based decision making in formulating urban health policies. In addition, an integration oriented perspective based on an understanding of the relations between health and health determinants would widen policy interventions that are based on collaboration between different sectors of society.
References
Footnotes
-
Funding: this research is partly supported by a Grant in Aid of Scientific Research by the Japan Society of Promotion of Science.
-
Conflicts of interest: none.