Relation between parasuicide, suicide, psychiatric admissions, and socioeconomic deprivation
BMJ 1995; 311 doi: https://doi.org/10.1136/bmj.311.6999.226 (Published 22 July 1995) Cite this as: BMJ 1995;311:226
- David J Gunnell, lecturer in public health medicine and epidemiologya,
- Tim J Peters, senior lecturer in medical statisticsa,
- Robert M Kammerling, consultant in public health medicineb,
- Jane Brooks, NHS data analysta
- Department of Social Medicine, University of Bristol, Canynge Hall, Bristol BS8 2PR,
- Avon Health, Bristol BS2 8EE
- Correspondence to: Dr Gunnell.
- Accepted 24 May 1995
Abstract
Objective: To examine the relations between parasuicide, suicide, psychiatric inpatient admissions, and socioeconomic deprivation.
Design: Ecological analysis with data from routine information systems and the 1991 census.
Setting: 24 localities in the area covered by the Bristol and District Health Authority (population 817000), consisting of aggregations of neighbouring wards, with an average population of 34000.
Subjects: 6089 subjects aged over 10 years admitted to hospital after parasuicide between April1990 and March 1994; 997 suicides occurring 1982-91; 4763 subjects aged 10-64 years admitted withacute psychiatric illness between April 1990 and March 1994.
Results: Localities varied significantly in standardised admission ratios for parasuicide and standardised mortality ratios for suicide (P<0.001). Spearman's rank correlation coefficient between the standardised mortality ratio for suicide and standardised admission ratio for parasuicide was 0.73 (95% confidence interval 0.46 to 0.88). Correlation between parasuicide and Townsend score was 0.86 (0.70 to 0.94) and between suicide and Townsend score 0.73 (0.46 to 0.88). The partial correlation coefficient between suicide and parasuicide after the Townsend score was adjusted for was 0.29 (−0.13 to 0.62). The correlation between standardised admission ratio for parasuicide and standardised admission ratio for psychiatric illness was 0.76 (0.51 to 0.89) and between standardised mortality ratio for suicide and standardised admission ratio for psychiatric illness was 0.72 (0.45 to 0.87).
Conclusion: A strong ecological association exists between suicide and parasuicide, with socioeconomic deprivation accounting for much of this relation. This strong association provides supporting evidence for the importance of social policy measures in attaining Health of the Nation targets on mental health.
Key messages
Key messages
This study found that a strong ecological association exists between suicide and parasuicide and that both these factors are related to socioeconomic deprivation
Social policy changes aimed at reducing socioeconomic deprivation may be more effective than health service activities in reducing suicide
The relation between standardised mortality ratios for suicide and standardised admission ratios for psychiatric admission suggests that the government's targets for reducing suicide may act as reasonable proxy measures for the mental health of the population, as measured by the need for psychiatric admission
Introduction
The relation between parasuicide and suicide has been the subject of much debate.1 There are distinct demographic differences between those committing these two acts: parasuicide occurs more commonly in women and in younger age groups; suicide occurs more commonly in men, with the highest rates occurring among those aged over 75.2 The incidence of parasuicide is 10-20 times higher than that of suicide. Recently, however, suicide rates have increased in young men, and this rise has been accompanied by increases in the number of male parasuicide admissions.3 4 In addition, in 30-47% of cases of suicide the individual has a history of parasuicide, and 3-10% of individuals who commit parasuicide commit suicide within 10 years of their attempted suicide.5 6 7 8
The government's document Health of the Nation set targets for the reduction of suicide,9 although the choice of suicide as an outcome indicator for mental illness services has been questioned.10 11 Suicide is a rare event, and suicide rates may be a poor indicator of the overall burden of mental illness in a community. In addition, as effective interventions against suicide have not been identified, health service strategies to achieve the government's targets are difficult to formulate.12 Other measures, such as admission rates for depressive illness, would be more useful if they were not influenced by variations in access to and patterns of service delivery. A recent population based survey found a positive correlation between depression (measured with the hospital anxiety and depression scale) and admission rates for depressive illness.13 In Bristol recent work has shown a strong correlation between unemployment rates and psychiatric admission rates.14 Using similar techniques but with updated information from the 1991 census, we explored the relation between two well accepted indicators of mental distress--suicide and parasuicide--and psychiatric admission rates. We also explored the ecological relation between parasuicide and suicide and between both these acts and an index of socioeconomic deprivation.
Methods
HOSPITAL ADMISSION DATA AND POPULATION DATA
We obtained details of patients aged over 10 and resident in the area covered by the Bristol and District Health Authority admitted after parasuicide between April 1990 and March 1994 from the South and West region's patient administration system (a routine health information system). We used the same system to identify patients aged 10-64 admitted under the specialty of mental illness over the same four year period. The patient administration system records patients' details, including date of birth, sex, and postcode, for all admissions to hospitals in the South and West region (formerly the South Western region). Each of the four main health care providers in the Bristol and District Health Authority is linked to the patient administration system, thus ensuring 100% coverage of all the authority's inpatient episodes. Patients resident in the area covered by the district health authority who are treated elsewhere in the region are similarly recorded and identifiable on the region-wide system. In all, 96.6% (5882/6089) of parasuicide admissions had a postcode for area of residence entered on the system. The number of district residents treated following parasuicide outside the region was small (94/6089 (1.5%)). All medical coders in the district are centrally trained and frequently audited. Senior coders meet every three months to discuss coding issues, which increases consistency between hospitals.
In the South and West region parasuicide admissions are identified by the codes E950-E959 (suicide and self inflicted injury) and E980-E989 (injuries undetermined whether accidentally or purposely inflicted) from the International Classification of Disease, ninth revision. We used this extended definition for parasuicide to ensure complete case ascertainment. Similarities in the age distributions for parasuicide coded as deliberate and for parasuicide coded as accidental overdose (E850-E859), except in elderly people, suggest that deliberate self poisoning is often coded as accidental. To overcome any variation in coding practices and to gain the most complete picture of parasuicide in the district we combined both these categories. Our figures may therefore slightly overestimate (by less than 5%) the true picture, particularly for older people, in whom accidental self poisoning is more likely. We did not include accidental injuries in this way. Wrist laceration coded as accidental is more likely to be truly accidental than is overdose coded as accidental, and inclusion of the former episodes may therefore distort the estimate of incidence. We omitted individuals aged 10 years or under from the analysis as intentional self harm in children is rare; self harm is most likely to be accidental.
To assess variations in event rates by small area we divided the district into 24 localities defined by postcode (mean population 34000) that were made up of aggregations of electoral wards to reflect natural communities. These had been previously identified and used for locality profiling by the district health authority (Bristol and District Health Authority's locality profiling notes, 1992). The population structure of these areas has changed little in the 13 years examined. Before considering correlations with deprivation, we investigated whether the observed differences between localities could have arisen by chance. Assuming a Poisson distribution, an approximateχ2 test statistic is available15 since the standard used here is the district itself.
To assess person based admission rates, we linked separate episodes of care using district number, date of birth, and sex. Age and sex standardised parasuicide and psychiatric admission ratios for the district's residents, admitted to both psychiatric and general hospitals under the specialty of mental illness, were calculated by the indirect method of standardisation with 1991 census data from the Office of Population Censuses and Surveys for the Bristol and District Health Authority. Townsend scores were calculated for each of the localities from information collected in the 1991 census.16
SUICIDE DATA
Mortality data for 1982-91 were obtained from the Office of Population Censuses and Surveys' mortality files for Bristol and District Health Authority. These data covered a longer period of time to ensure there were sufficient events to produce standardised mortality ratios for each of the 24 localities of the district. There were on average 90-100 suicides a year in the district (ICD codes E950-E959, E980-E989). We included suicide and undetermined deaths as for parasuicide. Although there have been some changes in the population of Bristol over the 13 years covered by the morbidity and mortality data, comparison of 1986 mid-year population estimates with those of the 1991 census showed that there had been no significant changes between localities. Therefore the district population given by the 1991 census was again used as the standard population for calculating standardised mortality ratios.
STATISTICAL METHODS
Spearman's rank correlation coefficient was calculated to examine the relations between parasuicide, suicide, psychiatric admission, and deprivation. Nonparametric procedures were used to account for the effect of outlying values, which may exert a disproportionate influence on the strength of the relation observed with parametric statistics. We checked the age specific rates for parasuicide, psychiatric admissions, and deaths from suicide to ensure that the patterns are consistent with the summary standardised admission ratios and standardised mortality ratios. For all outcomes, for the age groups with adequate numbers of events, the age specific rank orders of the areas were practically identical to the rank order for the summary, though age groups for deaths from suicide had to be aggregated.
Results
Between April 1990 and March 1994, 6089 residents in the Bristol and District Health Authority were admitted after parasuicide, and 4763 were admitted to psychiatric hospitals for psychiatric illness; 9% (144/1615) of those admitted in the 12 months April 1992 to March 1993 to general hospitals after parasuicide were transferred to psychiatric hospitals after psychiatric assessment. Between 1981 and 1992 there were 997 deaths from suicide. There were significant variations between localities in standardised admission ratios for parasuicide χ 2=1246, df=23; P<0.001) and psychiatric illness χ 2=1415 df=23; P<0.001) and the standardised mortality ratio for suicide χ 2=163, df=23; P<0.001) (table).
Standardised admission ratios (95% confidence intervals) for parasuicide (April 1990 to March 1994) and standardised mortality ratios for suicide (1982-91) for 24 localities covered by Bristol and District Health Authority
RELATIONS BETWEEN PARASUICIDE AND SUICIDE AND SOCIOECONOMIC DEPRIVATION
We examined the relation between parasuicide and suicide as two markers of psychiatric illness and the Townsend index, a composite measure of socioeconomic deprivation. A strong relation was found for parasuicide (Spearman's rank correlation coefficient 0.86 (95% confidence interval 0.70 to 0.94)) and suicide (0.73 (0.46 to 0.88)) (fig 1). No clear pattern was seen in the distribution of the standardised admission ratios for parasuicide across the district's four acute hospitals, suggesting that systematic differences in admission policies did not confound the observed relation.

Relation between (a) standardised admission ratio for parasuicide (1990-4) and Townsend score (1991 census) and between (b) standardised mortality ratio for suicide (1982-91) and Townsend score (1991 census), for 24 localities covered by Bristol District Health Authority
{kind=link}

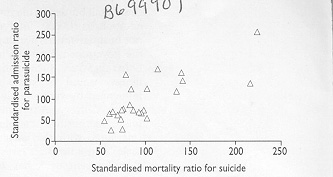
Relation between standardised admission ratio for parasuicide (1990-4) and standardised mortality ratio for suicide (1982-91) for 24 localities covered by Bristol District Health Authority
{kind=link}

Relation between standardised admission ratios for parasuicide (1990-4) and psychiatric admission (1990-4; ages 10-64) for 24 localities covered by Bristol District Health Authority
{kind=link}

Relation between standardised mortality ratio for suicide (1982-91) and standardised admission ratio for psychiatric admission (1990-4; ages 10-64) for 24 localities covered by Bristol District Health Authority
{kind=link}
RELATION BETWEEN PARASUICIDE AND SUICIDE
Figure 2 shows the relation between standardised admission ratios for parasuicide and the standardised mortality ratio for suicide for each of the 24 localities of Bristol. The Spearman's rank correlation coefficient for these two measures was 0.73 (0.46 to 0.88). The partial correlation coefficient for standardised mortality ratio for suicide and the standardised admission ratios for parasuicide, adjusted for the effect of socioeconomic deprivation as measured by the Townsend score, was 0.29 (−0.13 to 0.62).
RELATIONS BETWEEN STANDARDISED ADMISSION RATIOS FOR PARASUICIDE, STANDARDISED MORTALITY RATIOS FOR SUICIDE, AND PSYCHIATRIC ADMISSION
Figures 3 and 4 show the relations between standardised admission ratios for parasuicide and standardised mortality ratio for suicide with standardised admission ratios for psychiatric admission. The correlation coefficient for standardised admission ratios for parasuicide with psychiatric admission rate was 0.76 (0.51 to 0.89). A similar relation between suicide and standardised admission ratios for psychiatric admission was found (0.72 (0.45 to 0.87)).
Discussion
SUICIDE AND PARASUICIDE
A strong ecological relation exists between suicide and parasuicide; areas with high standardised mortality ratios for suicide also have high standardised admission ratios for parasuicide. This relation is present despite differences in the age-sex profile of the individuals committing the two acts and is partially explained by socioeconomic deprivation. The increased risk of suicide after parasuicide is recognised5; this phenomenon is unlikely to account, however, for the observed relation as less than 10% of individuals committing parasuicide go on to commit suicide.
SOCIOECONOMIC DEPRIVATION AND MENTAL ILLNESS
A strong ecological relation was also found between suicide and parasuicide (both well accepted indicators of psychiatric morbidity) and psychiatric admission rates in individuals aged 10-64. Hence psychiatric admission rates may reflect levels of psychiatric morbidity as indicated by parasuicide and suicide rates. The relation between parasuicide and one indicator of socioeconomic deprivation (unemployment) was documented in the early 1980s17 with both individual and ecological analyses. In Bristol a similar relation was found between unemployment and psychiatric admission rates in the 1990s14 and between parasuicide and deprivation in the 1970s.18 Rises in unemployment do not necessarily lead to rises in suicide,19 though we confirm a strong relation between suicide, parasuicide, and socioeconomic deprivation in the 1990s. Although raised standardised mortality ratios for suicide are found in social class I as well as class V and unemployed individuals, the relatively small number of cases of suicide in social class I leads to little impact on the standardised mortality ratio for suicide for locality.20
LIMITATIONS OF ADMISSION DATA FOR PARASUICIDE
Only individuals admitted after attending hospital for parasuicide are included here. In the Bristol District Health Authority about 63% of patients attending accident and emergency departments are admitted after parasuicide (Gunnell et al, unpublished data). The incidence of parasuicide after which the individual does not attend accident and emergency departments in the Bristol district is unknown. In addition, systematic differences may exist between hospital admission policies for parasuicide and the sociodemographic characteristics of catchment areas. This is unlikely, however, since the four hospitals in the Bristol district cover the observed range in Townsend scores and parasuicide admission ratios (fig 1). Systematic differences in the way general practitioners treat parasuicide in better off areas may also account for some of the observed differences, though this probably does not greatly confound the observed correlations.
THE ECOLOGICAL FALLACY
Ecological relations do not imply causation and have three main limitations. Firstly, we did not obtain indices of socioeconomic deprivation for individuals admitted to hospital or committing suicide. Individuals may not share the socioeconomic characteristics of the area population (the ecological fallacy). Secondly, those with mental illness may be differentially attracted to areas of deprivation by the availability of hostels and local authority housing as well as by the anonymity of life there.21 22 This is less likely to be the case with parasuicide than with severe mental illnesses such as schizophrenia. Lastly, underenumeration at the census--that is, disproportionately high underestimation of the population denominator in the more deprived areas--is a possible explanation.23 No information was available by locality to allow for this, and average underenumeration for districts is thought to be small (less than 1%). Moreover, this should have particular influence on young people, and, as stated, the relations between standardised mortality ratio and standardised admission ratio and deprivation are similar in all age groups.
Despite these reservations the relations between socioeconomic deprivation and health are well documented.24 For example, if the whole population experienced the same death rates as the non-manual classes an estimated 17000 fewer deaths would occur among 20-64 year old men.25 The close link between suicide and parasuicide shown here may be more noticeable now because of the increases in suicide among young men. For young men the factors associated with the rise in suicide may also be associated with rises in parasuicide. In the absence of effective interventions to prevent suicide and parasuicide, social policy changes aimed at decreasing socioeconomic deprivation may be more effective in reducing the incidence of acts. The Health of the Nation, however, did not include such targets.
CONCLUSIONS
These data and previous research support two conclusions. Firstly, the importance of socioeconomic deprivation as an indicator and possible determinant of psychiatric morbidity and suicide is clearly demonstrated. From these and other data, social policy and government measures to reduce socioeconomic deprivation may be as important in realising the Health of the Nation targets for suicide as health service activities. Such measures may also affect other indices of psychiatric ill health. Secondly, although suicide and parasuicide differ in several respects, the ecological relation between these acts suggests that they share to some extent a common cause and that this cause is largely related to socioeconomic deprivation.
Acknowledgments
We thank Mariallena Trivella and Simeon Barron for data preparation; Mike Shepherd for advice on the localities of Bristol; Mr R White (regional coding officer) for advice; Dr A Round for comments; accident and emergency consultants in Bristol and District Health Authority and Professor H G Morgan and Dr J Evans for information on admission to hospital after parasuicide.
Footnotes
-
Funding No specific funding.
-
Conflict of interest None