Article Text

Abstract
Objective: Parenting may be an important protective factor against teen driving risk; however, parents do not limit teen driving as much as might be expected. The Checkpoint Program was designed to promote parental management of teen driving through the use of staged persuasive communications.
Methods: Parent-teen dyads (n = 452) were recruited when teens received learner’s permits and interviewed over the telephone at baseline, licensure, and three months post-licensure. After baseline, families were randomized to either the intervention group that received persuasive communications or to the comparison group that received general information about driving safety.
Results: Both parents and teens in the intervention group reported significantly greater limits on teen driving at licensure and three months post-licensure. In multivariate analyses, intervention and baseline driving expectations had significant effects on driving limits at licensure. Intervention and driving limits established at licensure were associated with three month driving limits.
Conclusion: The findings indicate that exposure to the Checkpoints Program increased parental limits on teen driving.
- driving risk
- young drivers
- parenting
- parental management
- DMV, Department of Motor Vehicles
- GDL, graduated driver licensing
- PCs, persuasive communications
- driving risk
- young drivers
- parenting
- parental management
- DMV, Department of Motor Vehicles
- GDL, graduated driver licensing
- PCs, persuasive communications
Statistics from Altmetric.com
- driving risk
- young drivers
- parenting
- parental management
- DMV, Department of Motor Vehicles
- GDL, graduated driver licensing
- PCs, persuasive communications
- driving risk
- young drivers
- parenting
- parental management
- DMV, Department of Motor Vehicles
- GDL, graduated driver licensing
- PCs, persuasive communications
Motor vehicle crashes are the leading cause of death and injury among teenagers between the ages of 16 and 19. Teen crash rates are higher than those of any other age group,1–5 and disproportionately high at weekends, with teen passengers, and at nighttime.2,4–9 High crash rates among teens are attributed to their young age, lack of driving experience, and relative propensity for risky driving.3,10,11
Recognition of the increased risk of driving among teens, particularly in high risk conditions such as at night and with teen passengers, has stimulated many states to adopt graduated driver licensing (GDL) programs. Research indicates that certain components of GDL programs, including delayed ages at permit and provisional license, increased supervised driving, and nighttime driving curfews, have resulted in reduced rates of teen risky driving behaviors, crashes, violations, and overall amount of driving.12–19 However, the characteristics of GDL programs vary from state to state and few jurisdictions have all the elements of an optimal program as identified by the Insurance Institute for Highway Safety.20 Presumably, states with more of the specified provisions would be most effective in reducing teen crashes. As an added benefit, GDL programs may enhance and support parents’ efforts to moderate teen driving.
With or without GDL programs, parents would seem to be in a prime position to impose and enforce driving restrictions on young drivers. Parents are involved in their teenagers’ driving from the beginning, teaching them to drive, governing their access to vehicles, and setting rules. However, parenting as related to teen driving risk is surprisingly understudied. In this paper we review literature linking parenting and teen driving, and present the Checkpoints Program and process and impact data supporting it.
PARENTING AND TEEN DRIVING
Parents have a substantial opportunity to affect safe teen driving because they are involved in their teenagers’ driving from the beginning, teaching them to drive and governing their access to vehicles. Teenagers also report that parents set driving rules such as “don’t drink and drive”, “tell parents where you are going and with whom”, and “be home at a certain time”.21,22 A growing body of literature in the area shows relations between parenting and teen driving.23 For example, Beck and others24 found that more frequent parental supervision and restricted teen access to a car were associated with less likelihood of teens speeding and more likelihood of their using seat belts when driving. With data from 300 adolescents licensed two years or less, Hartos and colleagues25 found that low parental monitoring and control were related to risky driving behaviors, traffic violations, and motor vehicle crashes among the teens. In fact, violations were about four times more likely and crashes were almost seven times more likely with lenient restrictions related to frequency of friends as passengers. Of these adolescents, 261 completed follow up interviews about risky driving behaviors three months later. The results showed that risky driving at follow up was predicted by risky driving at baseline, parental restrictions on driving, and sensation seeking. In addition, 80% of teens consistently reported either high or low levels of risky driving at both time points. When compared to adolescents with low risky driving at both time points (n = 129), adolescents with high risky driving at both time points (n = 79) were three times more likely to report low parental monitoring and two times more likely to report low parental restrictions.26
Our next study27 looked at whether parent imposed delayed licensure and restricted driving are related to fewer teen risky driving behaviors. At baseline, 275 teenagers who received a learner’s permit and one of their parents were interviewed, and one year later, 161 of the teenagers had since obtained a provisional license and were reinterviewed. The results indicated that parents reported delaying teen licensure until teens were “ready”, and they limited teen driving in terms of trip conditions (for example, getting permission, reporting return time) more so than driving in high risk conditions (for example, at night, with teen passengers). In addition, higher levels of teen risky driving behaviors were predicted by younger ages at licensure and fewer reported limits on driving in the first month. Risky driving was also related to male gender, higher conflict over driving, lower perceptions of dangers related to driving, more problem behaviors at baseline, and more high risk driving (for example, at night, teen passengers).
Although parents are in a prime position to influence their teens’ driving behaviors, research indicates that many parents are less involved with their teens driving than they could be. Beck and colleagues24,28 found that for the majority of incidents, parents were not aware that their teens drove under the influence, rode with other drinking drivers, were distracted by friends/passengers while driving, did not wear seat belts, drove aggressively, or ran stop signs/traffic lights. Other studies29,30 also document a tendency of parents to under-personalize risks related to teen driving and to attribute impaired driving to their teens’ friends rather than to their own teens.
In addition, an alarming number of teens do not report having driving rules or restrictions for high risk driving conditions, including driving at night and with teen passengers.24,25 Despite research linking teen passengers with crashes,5–7 Hartos and colleagues25 found that adolescents reported that they were allowed to have “many” teens as passengers “most of the time”. Likewise, Beck and others24 found that only a little more than half (55%) of the teen drivers in their survey reported any restrictions on the total number of passengers allowed in the car when they were driving, and only 25% reported being restricted to no teenage passengers.
Thus, the research addressing parenting and teenagers’ driving suggests that: (1) teen driving risk is related to parenting, especially parental monitoring and restrictions on driving; and (2) many newly licensed teens report few driving restrictions, especially under the most dangerous conditions, such as at night and with teen passengers.
CHECKPOINTS PROGRAM
Parental management of teen driving is an important target for intervention research for a number of reasons: (1) teen driving is dangerous; (2) most teens are highly motivated to drive; (3) many parents are somewhat ambivalent about their teens starting to drive; and (4) clear guidelines for parents on why and how to manage teen driving are not generally available. Many programs and instructional materials have been developed to help parents teach adolescents to drive, but few educational materials have been developed to encourage and teach parents how to manage teen driving risk. The Checkpoints Program is a conceptually based educational intervention that aims to reduce teen driving risk by increasing parental management of teens’ early driving through the use of persuasive parent education materials.
Persuasive communications (PCs) are educational messages intended to alter salient beliefs or attitudes that motivate behavior. A key to the effectiveness of PCs is directing them toward dispositions of the target population that are operationally related to the target behavior. Social learning theory posits that perceived norms, attitudes, and expectations influence behavior. Therefore, PCs may enhance people’s capacity and motivation to perform a specific target behavior when it is presented as important, widely accepted, relatively easy to carry out, and effective if carried out.31,32 In addition, messages are thought to be most effective when they are clearly defined, credible, adapted to the needs and characteristics of the audience, and conveniently delivered to them.33
Thus, PCs adapted to the specific needs and perceptions of the target population and delivered frequently in an attractive and easily understandable form may influence parents to adopt driving restrictions to lower their teens’ risk for crash. Accordingly, attitudes towards the risks of teen driving, perceptions about how common it is for parents to restrict teen driving, and expectations about having driving restrictions may be related to the establishment of driving limits for newly licensed teens. The Checkpoints Program includes PCs that target these areas in the form of a video, newsletters, and a parent-teen driving agreement.
METHODS
Parents and teens are recruited at offices of the Connecticut Department of Motor Vehicles (DMV) when teens receive a learner’s permit, are randomly assigned to the Checkpoints Program or a general traffic safety education group, and are followed for two years. The goal of the intervention is to increase teen driving restrictions, especially under higher risk conditions such as at night and with teen passengers, by having families negotiate a parent-teen driving agreement. Parents and teens complete telephone interviews at recruitment, when teens become licensed, and at three months, six months, and 12 months post-licensure.
Soon after recruitment, families in the intervention group receive a video that introduces the risks of teen driving and sets expectations about restricting teen driving privileges and completing/adhering to a parent-teen driving agreement. During the time teens have a learner’s permit, families are mailed frequent, brief, persuasive communications in the form of newsletters. These newsletters are designed to increase family perceptions about the extent and nature of certain risks posed by teenage driving (for example, not wearing a seat belt, driving with multiple teen passengers, driving late at night), normative expectations that most parents restrict their teen’s driving, and the value of parents managing teen driving.
Just prior to teens obtaining a driver’s license, families receive a parent-teen driving agreement in the mail. Behavioral contracts have been employed successfully in a wide range of contexts and behaviors because they establish clear expectations, performance standards, consequences for noncompliance, and the period of successful compliance required to earn additional privileges.34,35 Therefore, driving agreements are potentially important tools to facilitate parental management of teen driving and reduce adolescent driving risk. Although a variety of driving agreements are available through insurance companies and local advocacy groups, none have been evaluated in terms of their content, adoption, and effectiveness.
The Checkpoints Driving Agreement was designed to encourage parents to strictly limit teen driving under high risk conditions (for example, on high speed roads, in bad weather, with teen passengers, and at night) during the first few months of licensure and gradually allow more driving privileges as teens gain driving experience and show responsible behavior over the next year or two. In addition to specifically outlining driving privileges under high risk conditions, the agreement helps parents establish teen driving rules, consequences for violating the rules, and markers of experience and success that will enable teens to earn greater driving autonomy. Then, over the first six months that teens have licenses, families receive additional newsletters that support and encourage parents to continue limiting and monitoring teen driving.
Intervention
There are limited opportunities to intervene with parents and teens regarding driving. Most driver education courses are devoted to teaching teens exclusively and do not include parents in the process. Although parents commonly accompany teens to a DMV office when they test for their permit and license, offices are generally crowded, noisy, and busy, so they may not be good places at which to deliver educational materials on parental management of teen driving. In the Checkpoints Program, families receive educational materials in the form of newsletters by mail. In a pilot study, parents of 98 adolescents in drivers’ education classes were mailed two sample newsletters that significantly altered their attitudes towards the risks of teen driving and the benefits of restricting teen driving. In other preliminary research, the acceptability, format, and content of the Checkpoints Driving Agreement was tested with a convenience sample of 47 families recruited as teens tested for their licenses at five private driving schools in Connecticut. Family members were interviewed at the schools about intended limits on teen driving, asked to use the driving agreement, and reinterviewed within three months about acceptability of the driving agreement and initial driving limits placed on teens. Most families (38 of 47) reported using and liking the agreement and adopting the Checkpoints recommendations for strict initial limits on teen driving related to driving unsupervised at night, with teen passengers, and on high speed roads. Ultimately, parents reporting placing more strict limits on their teens’ driving than they originally intended.36
Design
A full scale pilot is currently underway to test the impact of exposure to the Checkpoints Program on parental restriction of teen driving. A total of 486 eligible families were approached for recruitment at eight offices of the Connecticut Department of Motor Vehicles, and 452 parent-teen dyads (93%) agreed to participate in the program. (Connecticut licensing laws allow permits beginning at age 16 and full privilege licenses after the permits have been held for at least four months.) Recruited families were randomized to either the group that receives the Checkpoints Program materials or the group that receives a general set of materials related to driving and cars. Parents and teens are being assessed at baseline (immediately after recruitment), when teens become licensed, and three months, six months, and 12 months post-licensure. At this time, we have complete interview data for baseline, licensure, and three months post-licensure.
Measures
Driving limits were assessed shortly after teen licensure and then three months after licensure by asking parents and teens if they had driving limits on types of roads, number of passengers, and curfew on weekends. Each was scored on a scale from 0, no limits, to 4, strict limits (see fig 1). In addition, independent variables assessed at baseline and included in the analyses reported here include gender of teen and parent, driving expectations, teens’ impulse control, and parent monitoring. Expectations about future driving were assessed by asking both parents and teens how often teens would be allowed to drive under 13 high risk conditions, including on high speed roads, with two teen passengers, and at night. Internal consistency was alpha = 0.82 for parents and alpha = 0.86 for teens. Teens were asked eight items about impulse control (alpha = 0.78) from Weinberger,37 with items such as, “when I’m doing something fun I tend to get carried away and go too far”. Teens also reported parental monitoring by responding to 11 items (alpha = 0.84) about how often their parents know about their activities (for example, “where you are when you are not at home or school” and “your behavior at school”).

Treatment group differences for each driving limit.
Analyses
The analyses examine treatment group differences in driving limits reported at licensure and three months post-licensure by teens and parents in the intervention and comparison groups. Multiple linear regression and path analyses were conducted to predict driving limits at licensure and three months post-licensure from several baseline variables, demographic characteristics, and treatment group assignment.
RESULTS
A total of 420 parent-teen dyads (93%) dyads completed baseline surveys. Of the family members, 45% of teens and 62% of parents were female. Interestingly, only about three quarters of the teens obtained driver’s licenses within 12 months of recruitment. Thus, only 73% of parent-teens dyads (307) completed surveys for time of licensure; 146 families were in the intervention group and 161 were in the comparison group. A total of 264 parent-teen dyads completed three month interviews; 125 in the intervention group and 139 in the comparison group. No demographic variables differed by group.
Table 1 shows the reactions to the Checkpoints Program materials by teens and parents in the intervention group at time of licensure. Most parents and teens reported receiving, watching, and discussing the video and receiving, reading, and discussing the newsletters. Just under half of parents and teens reported completing the parent-teen driving agreement; these families were satisfied with it and would recommend it to other families.
Parent and teen reactions to the Checkpoints Program
Figures 1 and 2 present driving limits reported by parents and teens at licensure and at three months post-licensure. Figure 1 shows driving limits for each of three risk conditions at each time point. These three limits were combined into a composite score for overall driving limits, reported in fig 2, for parents and teens. Teens and parents in the intervention group reported significantly higher levels of restrictions for the risk conditions at both time points (all p values <0.05). In addition, composite scores for teens and parents in the intervention group were higher than those for teens and parents in the comparison group at both licensure (teens: t = 4.99, p < 0.0001; parents: t = 4.31, p < 0.0001) and three months post-licensure (teens: t = 3.64, p < 0.0003; parents: t = 3.70, p < 0.0003). Interestingly, parents within both groups reported significantly greater teen driving limits than did their teens at both licensure (intervention: t = 6.51, p < 0.0001; comparison: t = 9.62, p< 0.0001) and three months (intervention: t = 8.06, p < 0.0001; comparison: t = 9.41, p < 0.0001).
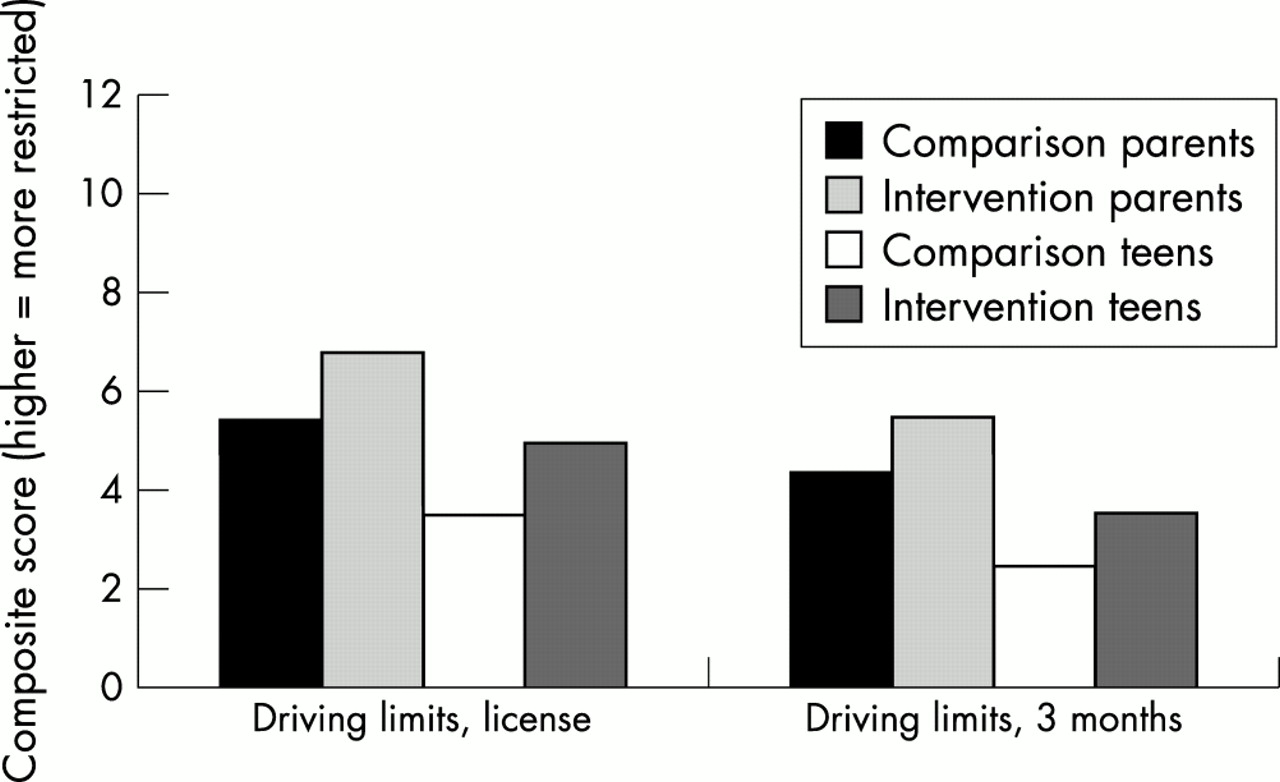
Treatment group differences for overall driving limits.
To test for intervention effects, multiple linear regression analyses were conducted separately for parent and teen reports at licensure and three months, with composite scores for driving limits as the outcome, as shown in table 2. In the licensure models, baseline measures of teen gender, parent gender, parent monitoring, teen impulse control, and teen and parent restriction expectations were included along with treatment group. In the parent licensure model, treatment group, parent gender (mothers were more restrictive than fathers), teen baseline driving expectations, and parent baseline driving expectations were significantly associated with driving limits. Similarly, in the model for teen reports of driving limits at licensure, treatment group, teen and parent baseline driving expectations, and parent gender (mothers were more restrictive than fathers) were significantly associated with higher driving limits. In the three month parent model, driving limits established at licensure and treatment group were significant. However, in the three month teen model, only restrictions at licensure were associated.
Regression results for predicting teen driving limits
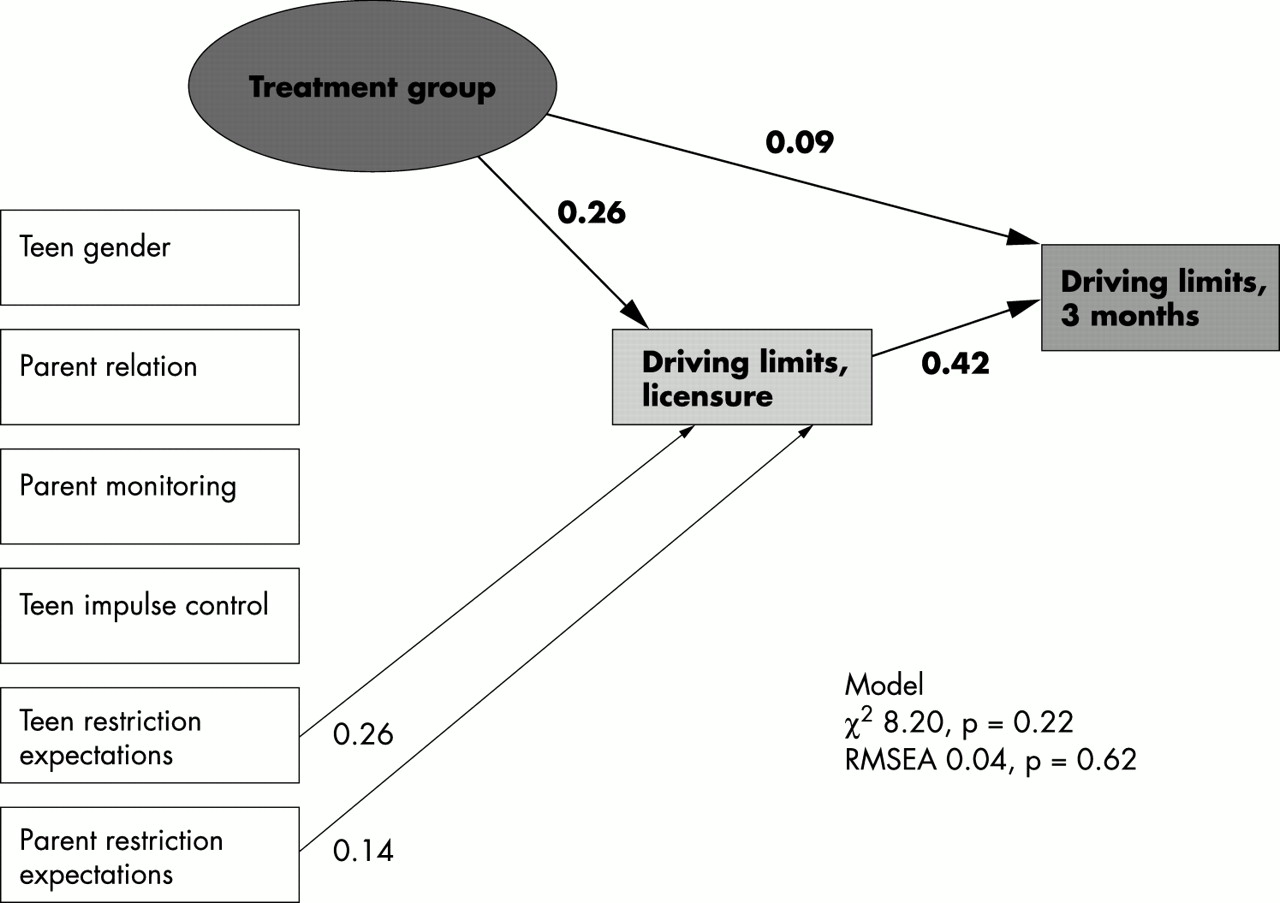
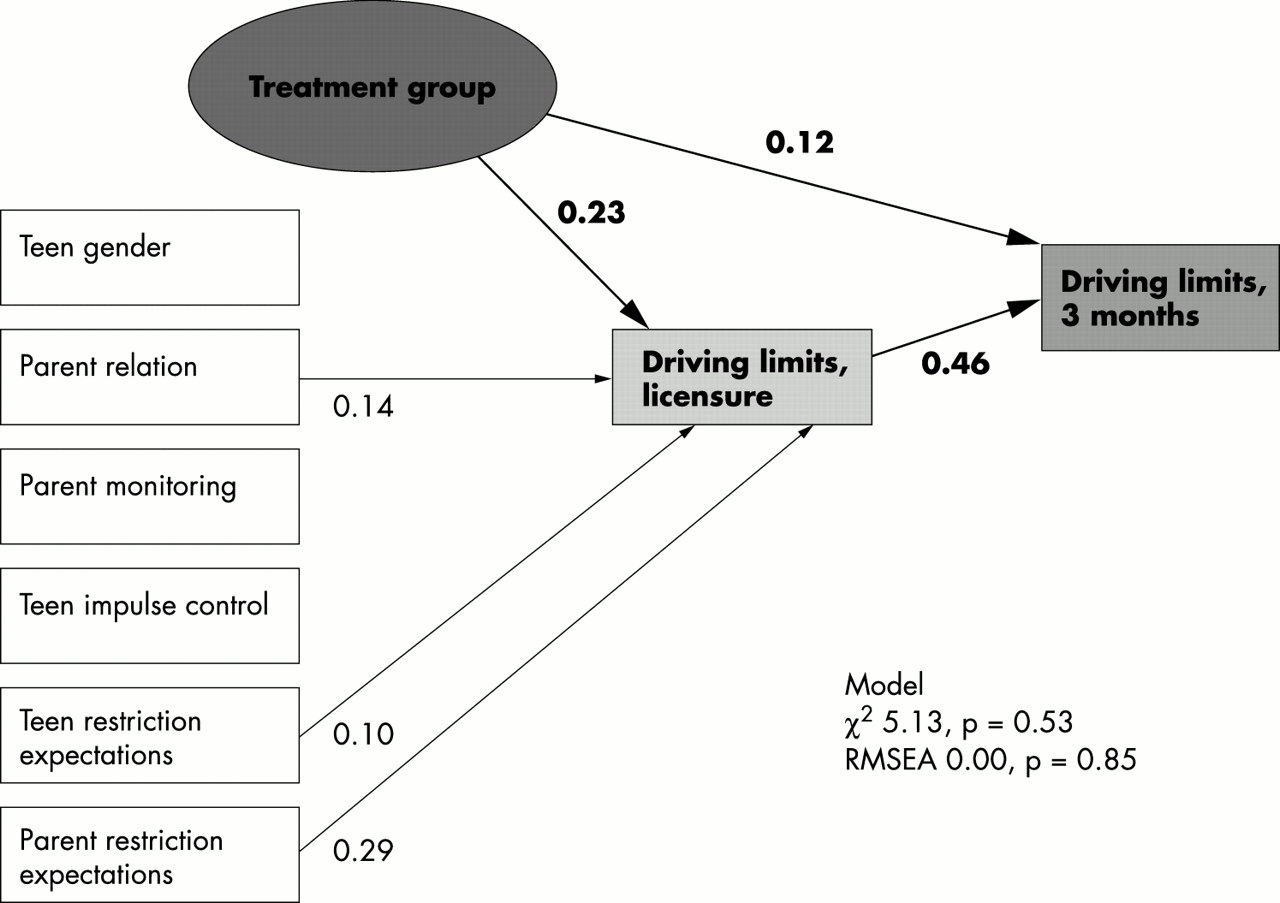
To illustrate the patterns of relations among the variables related to teen driving limits, separate path analyses using Mplus (version 2)38 were conducted for parents and teens which included the same variables as in the multiple linear regressions. Tests of model fit for parent data indicated good model fit: χ2 = 5.13, p < 0.53 (good model is indicated by a p value >0.05) and RMSEA (root mean square error of approximation) = 0.00, p < 0.85 (RMSEA is a combined measure of goodness of fit and parsimony and good models have a value of 0.05 or less and a p value approaching 1.00). For parent reports, shown in fig 3, exposure to Checkpoints was significantly associated with driving limits at three months, but driving limits at licensure was the best predictor. Figure 3 also shows positive effects on driving limits at licensure of exposure to Checkpoints along with female parent, teen baseline expectations, and parent baseline expectations. In addition, the results also indicated adequate model fit for teen reports: χ2 = 8.20, p < 0.22; RMSEA = 0.04, p < 0.62. For teen reports, shown in fig 4, exposure to treatment predicted driving limits at licensure; however, only licensure limits were related significantly to driving limits at three months.
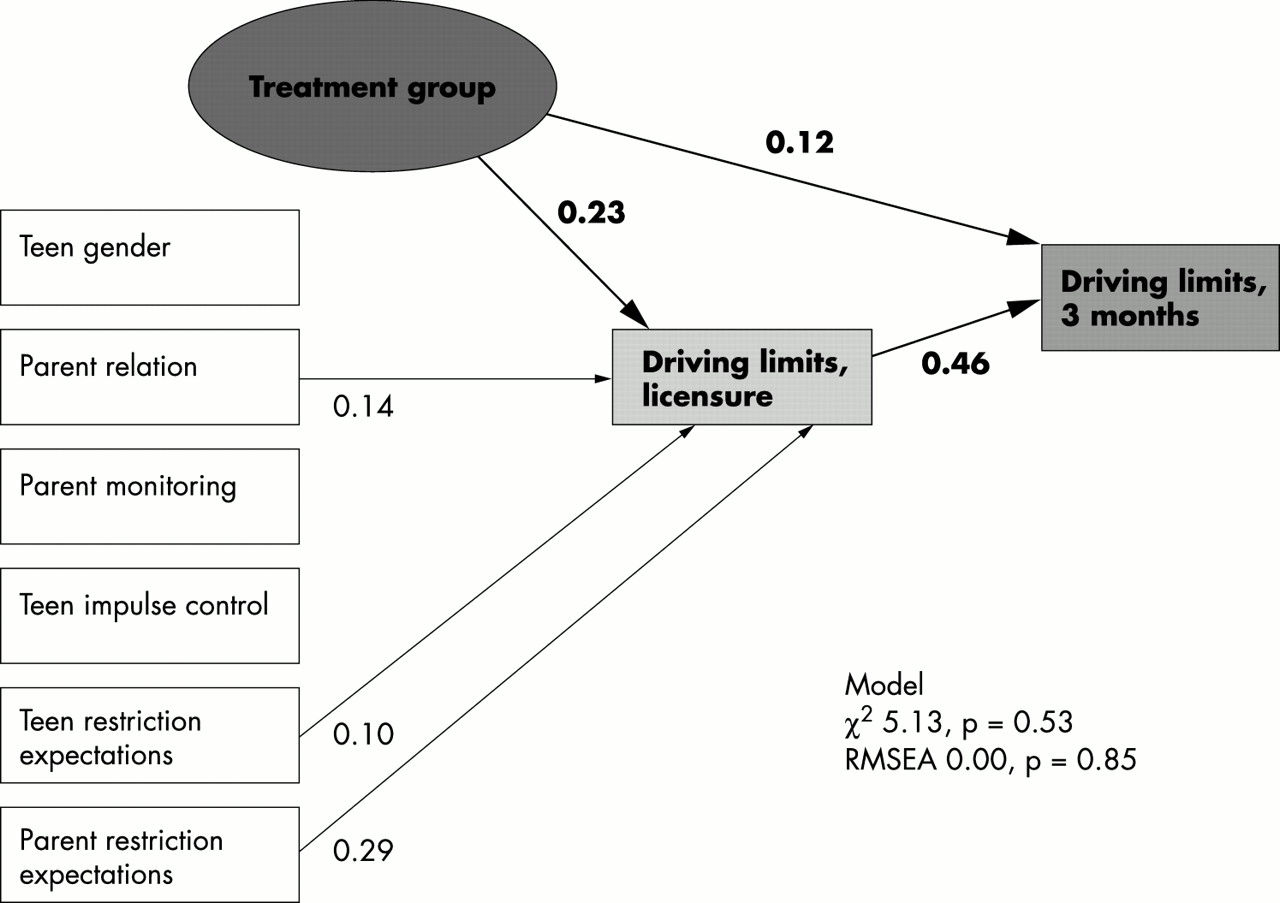
Path analysis for parent reports predicting teen driving limits at three months post-licensure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Path analysis for teen reports predicting teen driving limits at three months post-licensure.
The multivariate models produced R squares of 0.41 for teen reports and 0.38 for parent reports, indicating that a substantial portion of the variance in driving limits could be explained by the variables included. Both sets of model fit statistics (χ2 and RMSEA) indicated that the data were an adequate fit for the models. For the parent data, restriction expectations contributed greatly, and treatment group and attitudes toward risk contributed about equally, to the variance. For the teen data, restriction expectations provided the greatest contribution to the explanation of the variation in driving limits, followed by treatment group.
DISCUSSION
A growing body of research indicates that parenting is related to teen driving risk. Thus, increasing parental management, which is the focus of the Checkpoints Program, may be an important influence on the reduction of teen driving risk. The strengths of the Checkpoints Program include the delivery of multiple messages that are tailored and timed to correspond to the teen’s driving experience and the focus on a single tool (Checkpoints Driving Agreement) to organize parental management of teen driving. In addition, this is the first controlled evaluation of the facilitated use of a parent-teen driving agreement. The results should provide valuable information about the extent to which parent imposed limits on teen driving can be influenced and whether parent limits result in reduced adolescent crash risk.
The findings of our research indicated that most parents and teens attend to mailed persuasive communications and that exposure to these materials appears to influence attitudes toward teen driving restriction and increase initial parental restrictions on teen driving at licensure. Most parents and teens in our pilot study reported receiving, reading or viewing, and liking the educational materials, and those exposed to the Checkpoints Program reported more strict driving limits than did those in the comparison group. Interestingly, parents in both groups reported stricter limits than did their teens. This difference may result from parents and teens not clarifying rules, or the bias of self report data toward social desirability, and possibly more so in the intervention group, where parents in particular might report greater limits than they actually impose to “look good”. Teen reports are probably less biased in this direction, but the “true” limits are most likely somewhere between parent and teen reports. Ways to validate parent and teen reported limits are needed.
The treatment group effects were statistically significant, but modest. Families exposed to the Checkpoints Program reported stricter teen driving limits under high risk conditions at licensure and three months post-licensure. Treatment group was associated with restrictions at three months post-licensure, but driving restrictions imposed at licensure was the best predictor, suggesting the importance of intervention addressing initial restriction practices. Clearly, it is easier to maintain restrictions over time than it is to establish new restrictions. Also associated with licensure restrictions were parents’ and teens’ baseline (pre-intervention) expectations about driving restrictions, suggesting the importance of addressing early expectations about driving limits and privileges.
While these results are promising, it remains to be seen whether these differences translate into increased teen driver safety and reduced crashes. For example, would an average difference of one hour in a weekend driving curfew (for example, 11 30 pm versus 12 30 am) reduce teenage driving risk, crashes, and injuries if adopted by a wide percentage of families? Also, the extent of maintenance of parental restrictions and the long term effect of the Checkpoints Program on teen driving, citations, and crashes remain to be assessed in ongoing follow up assessments. Based on the findings presented here, the Checkpoints Program materials have been modified and their effect is being assessed in a much larger randomized trial in Connecticut.
A great deal remains to be learned about the most effective timing, dose, intensity, and content of mediated persuasive communications and their effect of exposure on the maintenance of parental limits on teen driving over time. In addition, key parenting behaviors may differ, depending on any state sanctioned restrictions on teen driving. Connecticut is one of the few remaining states without any provisional driving restrictions, such as limiting teen passengers and nighttime driving. It may be that in states where such limits are sanctioned, parents may not need as much “persuading” to limit teen driving. However, it may be that in such states, parents are less willing to place additional restrictions on teen driving because the state sets restrictions. More research is needed to assess appropriate targeted parenting behaviors in states with no, some, and strict limits on teen driving. Currently, a trial is underway in Maryland, a state with graduated licensing, to assess the effects on parental management of teen driving of an abbreviated version of the Checkpoints Program implemented at the time teens obtain their provisional licenses.
REFERENCES
Discussion paper
The paper by Simons-Morton, Hartos, and Leaf represents an important step in advancing our understanding of how parental management of teen driving can be influenced. Their investigation has several notable strengths, including use of a randomized, controlled design, basis in a well reasoned theory of social influence (social learning theory), and delivery at multiple time points corresponding to the teen driving experience. Their focus on parents was well placed, as they are the immediate gatekeepers who allow teen access to cars and can determine when, where, why, and how often teens drive. In short, parents are in a prime position to influence the conditions under which teens acquire driving experience and to judge when their teens have developed sufficient levels of skills, experience, and maturity to expand their driving opportunities.
The findings from this investigation are intriguing and indicate directions for future research. There appear to be at least six different issues to be explored.
REACH AND FIDELITY OF INTERVENTIONS
There was evidence that the reach and fidelity of the parent based intervention materials may have been problematic. Whereas almost 95% of parents and 90% of teens said they read at least some of the newsletters, only 76% of parents and 63% of teens watched the video, and less than half of the parents (45%) and teens (47%) reported that they completed the driving agreement. Reasons for such low utilization rate of the main parental management tool, the driving agreement, of this intervention are unclear. Pilot data suggested that the driving agreement was well liked and seen as useful by parents.1 Yet, the present findings indicate that this was less likely to be so under real world conditions. This raises questions about the usability of the parent-teen driving agreement and whether parents are more likely to respond to materials that only provide information (for example, video and newsletters) as opposed to materials that promote action (driving agreement).
Research2,3 shows that in abstract or hypothetical cases, parents are more likely to favor stronger restrictions and even support a punitive response to teen risk. However, in the actual case (when the teen has actually engaged in some form of risky behavior), parents appear to be more lenient and apt to employ less restrictive and punitive measures. In other words, talk is cheap, before a parent actually confronts a teen whose privileges have to be restricted. Future research should focus on ways of increasing parental commitments to action by actually imposing teen driving restrictions. Investigations are also needed which examine the processes that parents use to set and enforce teen restrictions. It seems likely that in some circumstances, parents operate instinctively and are more likely to set restrictions, guidelines, and expectations on teen behavior as the need arises (that is, after some incident has occurred). The implicit assumption in this investigation is that parents can be made to follow a rational-proactive model, rather than an instinctive-reactive approach. We need to identify the fashion in which parents actually operate (rational-proactive versus instinctive-reactive) and develop interventions accordingly.
PARENT-TEEN (DIS)CONCORDANCE
There is considerable evidence of discordance between parents and their teens. Over 89% of the teens said they discussed the newsletters with their parents; and 82% of the parents said they discussed the newsletters with their teens. Figures 2 and 3 also indicate evidence of parent-teen discordance in terms of driving restrictions. This raises questions about which reporter is more believable in parent-teen dyad studies of reported driving restrictions. Is parenting best measured from the perspective of the provider (that is, the parent) or recipient (teen)?
For various reasons, parents are likely to report (perhaps even over report) that they communicate with their teens, engage their attention in traffic safety issues, and instill in them a common understanding about driving expectations. Yet, teens have a tendency to filter out some of this information (they fail to hear it, process it, remember it, accept it, or believe it). This can result in a significant loss of parental influence in certain areas. Much like the old philosophical question, “if a tree falls in the woods and nobody is there to hear it, does it really make a sound?”, one may ask “if a parent talks to a teen about traffic safety, but the teen isn’t listening, processing or remembering, does parenting really take place?” This suggests that parenting might best be measured from the teen’s perspective. Future research should address how parent information is received and filtered by teens, and whether parent-teen discordance is related to driving risk. If so, then parent based interventions might be developed to reduce this discordance.
DELIVERY OF INTERVENTIONS
Another issue concerns the delivery mode and whether these kinds of materials can be offered through other channels. This intervention was delivered by mail to parents at home, after being recruited at the motor vehicle agency. Would such materials have a higher utilization rate if they were delivered to parents while they are at the licensing agency, waiting for their son or daughter to be processed? An ongoing investigation in Maryland may provide the answer to this question. Regardless of how parents are reached with driving management materials, can this information be supplemented in other ways?
As we journey through the information age, it begs the question about whether the internet might be a useful medium through which parents (and teens) could be reached. Such a delivery strategy has certain advantages. It allows information to be delivered at home, on demand by the user. It can be tailored to the particular needs of the family and even updated or renewed on a regular basis as new information becomes available. Finally, it would allow linkage to other auxiliary sources of information (for example, parenting skills in general, social services, etc) that could be accessed by a wider array of parents. The extent to which teens and their parents would use such a system needs to be explored, along with other information delivery channels that will reach parents.
CONTENT OF INTERVENTIONS
Should interventions provide information to make parents better driving instructors, thus making them more adept at teaching their teens specific driving skills (that is, vehicle manipulation) and risk perception (danger recognition techniques)? Or should interventions focus on making parents effective at setting driving restrictions, including monitoring teens and modifying their driving privileges? The focus of this investigation is clearly on the latter.
For teens, it appears that outside of formal or informal driving instruction from parents or professionals, real benefits are derived from the experience they acquire while driving on their own. The assumption in this investigation is that teens need to have this opportunity to gain driving experience under relatively reduced risk circumstances (without teen passengers, on lower speed roads, not late at night, etc) and that as their driving experience, skills, and overall maturity increase, so, too, may their driving privileges. This suggests that there is no substitute for personal experience as a way of making teens safer drivers, and that parents may be largely irrelevant as driving skill instructors after teens begin driving on their own. At the provisional stage of licensure, such an approach might inadvertently remove parents from the business of providing any instruction and relegate them to the business of just establishing and regulating driving privileges. Research should address the extent to which parents might also benefit from information which enables them to teach advanced driving skills to their children and whether this results in any benefit to the teen driver.
TIMING OF INTERVENTIONS
When should intervention materials be delivered to parents to be most effective? Would it be appropriate to deliver these materials somewhat before teens are learning to drive (for example, age 14), when teens are learning to drive (as was the case in this investigation), or just after they have just become licensed? Would parents use such materials after the teen has been driving independently for some time (for example, during the first 6–12 months of licensure)?
Given that the nature of certain driving risks may change as adolescents become emergent adults (see the paper by Arnett in this issue), it is appropriate to examine how parental influence relates to this phenomenon. Many emerging adults 18–22 years of age are still dependent on some form of parental support and may even live at home with their parents. Therefore, parents are not entirely out of the responsibility loop once their child reaches the age of 18 and may still have some degree of leverage when it comes to managing their older teen’s level of driving risk.
EFFECTS OF INTERVENTIONS
Finally, it is not yet known if parent based materials, such as provided in the Checkpoints Program, can produce a significant and meaningful reduction in teen motor vehicle crash involvement. As with any behaviorally based intervention, there are several factors that will limit the likelihood of success.
The intervention must be of sufficient intensity and duration to achieve a change in the cognitive as well as behavioral domains of the parents. The results presented give us some indication as to the magnitude of the effect at this first level. Second, the parent’s behavior must be of sufficient duration and intensity to impact the cognitive and behavioral domains of their teens. Data are not yet available to indicate if teen driving behavior was changed. After this second threshold has been achieved, the ultimate outcome is whether there has been a reduction in motor vehicle crash risk. If this occurs, it would be informative to know if the parent intervention reduced teen traffic exposure (they drove less often), reduced teen risky driving (they drove safer), or both?
CONCLUSION
Parent based interventions in the area of parenting and teen driving present a unique set of challenges and opportunities. Parents have been under utilized as a source of influence in the traffic safety area. Coupling parent focused programs and progressive policy (graduated driver licensing programs) offers promise in reducing teen motor vehicle crash involvement.4 Clearly, the field is in need of careful research into the mechanisms by which parents can be reached and enlisted to restrict teen driving, and whether such strategies hold real promise for reducing teen motor vehicle crash risk. The investigation by Simons-Morton, Hartos, and Leaf offers evidence of the first stage in this process.