
Abstract
Mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) are particularly effective treatment approaches in terms of alleviating depressive symptoms and preventing relapse once remission has been achieved. Although engaging in mindfulness practice is an essential element of both treatments; it is unclear whether informal or formal practices differentially impact on symptom alleviation. The current study utilizes a correlational design to examine data provided by thirty-two previously depressed, remitted outpatients who received either MBCT or MBSR treatment. Outpatients in the MBCT group received treatment as part of a previously published randomized efficacy trial (Segal et al. in Arch Gen Psychiatry 67:1256–1264, 2010), while those in the MBSR group received treatment as part of a separate, unpublished randomized clinical trial. Throughout treatment, clients reported on their use of formal and informal mindfulness practices. Results indicate that engaging in formal (but not informal) mindfulness practice was associated with decreased rumination, which was associated with symptom alleviation.

Similar content being viewed by others


Notes
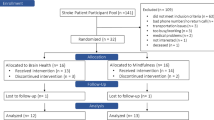
The MBSR group was recruited from one arm of a larger neuroimaging study comparing MBSR against a Progressive Muscle Relaxation active control group. Participants were right-handed adults recruited from a community based sample. Twenty-four participants fully remitted from unipolar depression were randomized into the two active-treatment groups, including the 14 MBSR group participants. Clinical history and remitted status were confirmed through assessment with an experienced clinical psychologist. All remitted patients had a history of one more past episodes of depression at the time of recruitment, with varied levels of ongoing antidepressant medication and psychotherapy. No participants had prior exposure to formal meditation or relaxation training, with the exception of some yoga classes in the past. MBSR participants attended an MBSR course led by experienced MBSR facilitators at the Centre for Addiction and Mental Health.
In the MBCT condition, participants were excluded if they had a current diagnosis of Bipolar Disorder, Substance Abuse Disorder, Schizophrenia or Borderline Personality Disorder or a trial of ECT within the past 6 months, or currently practiced meditation more than once per week or yoga more than twice per week. A full description of inclusion and exclusion criteria, treatment fidelity, and study details can be found in Segal et al. (2010). In the MBSR condition, participants were excluded if they had a current diagnosis of Bipolar Disorder, Substance Abuse Disorder, Schizophrenia, Borderline Personality Disorder, Post Traumatic Stress Disorder, or any Eating Disorder. Further, they were excluded if they had any current meditation practice or if they engaged in yoga. Given that participants completed fMRI scans, they were excluded if they carried a surgically implanted metal device such as a pacemaker.
In order to demonstrate mediation, the RSQ subscales must be measured during treatment, be significantly altered by treatment, and must temporally precede the outcome—although two time points are used, this is the case with the current data since the RSQ is measured on treatment session eight while the HRSD is measured 2 weeks following session eight. Further, the mediator must also then show a main and/or interactive effect with treatment on outcome; (i.e., the mediator and/or interaction term in the regression should be significant) while treatment need not have a significant overall or main effect on outcome. A main effect of mediation is demonstrated when treatment significantly changes the mediator but the effect of the mediator on outcome does not significantly differ across treatment types. In contrast, an interactive mediation effect occurs when treatment not only significantly impacts on the mediator but also changes the relationship between the mediator and outcome such that it differs across treatments. In the current analysis, both the HRSD and the RSQ are measured at two time points; however, the T2 HRSD was typically administered at least 2 weeks after the T2 RSQ, so the T2 RSQ temporally precedes the T2 HRSD administration.
When examining each group separately, path a was significant for both groups; the frequency of formal mindfulness practice predicted changes in rumination although the coefficients differed (MBCT a = −.49, MBSR a = −.44). No significant associations were found between frequency of formal, informal, and total mindfulness practice, as related to distraction. Path b, examining the relationship between rumination and depression symptom change when controlling for the independent variable, was significant for both groups, demonstrating that decreased rumination predicted decreased depressive symptoms (MBCT b = .43, MBSR b = .38). For path c, depressive symptom change was associated with both the frequency of formal mindfulness practice and total mindfulness practice for both groups (MBCT c = −.53; MBSR c = −.49). Finally, for path c’, the relationship between depressive symptom change and formal mindfulness practice remained significant for both groups (MBCT c’ = −.70; MBSR c’ = −.65).
References
Allen, M., Bromley, A., Kuyken, W., & Sonnenberg, S. J. (2009). Participants’ experiences of mindfulness-based cognitive therapy: “It changed me in just about every way possible”. Behavioural and Cognitive Psychotherapy, 37, 413–430.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Association.
Bagby, M. R., Rector, N. A., Bacchiochi, J. R., & McBride, C. (2004a). The Stability of the Response Styles Questionnaire Rumination Scale in a sample of participants with major depression. Cognitive Therapy and Research, 28(4), 527–538.
Bagby, M. R., Ryder, A. G., Schuller, D. R., & Marshall, M. B. (2004b). The Hamilton Depression Rating Scale: Has the gold standard become a lead weight? The American Journal of Psychiatry, 161, 2163–2177.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182.
Beiling, P. J., Hawley, L. L., Bloch, R. T., Corcoran, K. M., Levitan, R. D., Young, L. T., et al. (2012). Treatment-specific changes in decentering following mindfulness-based cognitive therapy versus antidepressant medication or placebo for Prevention of Depressive Relapse. Journal of Consulting and Clinical Psychology, 80(3), 365–372.
Bondolfi, G., Jermann, F., Van der Linden, M., Gex-Fabry, M., Bizzini, L., Rouget, B. W., et al. (2010). Depression relapse prophylaxis with mindfulness-based cognitive therapy: Replication and extension in the Swiss health care system. Journal of Affective Disorders, 122, 224–231.
Bowen, S., & Kurz, A. S. (2012). Between- session practice and therapeutic alliance as predictors of mindfulness after mindfulness-based relapse prevention. Journal of Clinical Psychology, 68(3), 236–245.
Broderick, P. C. (2005). Mindfulness and coping with dysphoric mood: Contrasts with rumination and distraction. Cognitive Therapy and Research, 29(5), 201–510.
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31, 23–33.
Eisendrath, S. J., Delucchi, K., Bitner, R., Fenimore, P., Smit, M., & McLane, M. (2008). Mindfulness-based cognitive therapy for treatment-resistant depression: A pilot study. Psychotherapy and Psychosomatics, 77(5), 319–320.
Evans, S., Ferrando, S., Findler, M., Stowell, C., Smart, C., & Haglin, D. (2008). Mindfulness-based cognitive therapy for generalized anxiety disorder. Journal of Anxiety Disorders, 22, 716–721.
First, M. B., Spitzer, R. L., Gibbon, M. & Williams, J. B. W. (1995). Structured Clinical Interview for DSM-IV Axis I Disorders (SCIDIP). Washington, DC: American Psychiatric Press.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: A meta-analysis. Journal of Psychosomatic Research, 57, 35–43.
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery and Psychiatry, 23, 56–62.
Hawley, L. L., Moon-Ho, R. H., Zuroff, D. C., & Blatt, S. J. (2006). The relationship of perfectionism, depression and therapeutic Alliance during treatment for depression: Latent difference score analysis. Journal of Consulting and Clinical Psychology, 74(5), 930–942.
Hawley, L. L., Moon-Ho, R. H., Zuroff, D. C., & Blatt, S. J. (2007). Stress reactivity following the brief treatment for depression: Differential relapse in psychotherapy and pharmacotherapy. Journal of Consulting and Clinical Psychology, 75(2), 244–256.
Hayes, A. F. (2009). Beyond Bron and Knny: Statistical mediation analysis in the new millennium. Communication Monographs, 76(4), 408–420.
Hofmann, S. G., Sawyer, A. T., Witt, A. A., et al. (2010). The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. Journal of Consulting and Clinical Psychology, 78, 169–183.
Jain, S., Shapiro, S. L., Swanick, S., Roesch, S. C., Mills, P. J., Bell, I., et al. (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: Effects on distress, positive states of mind, rumination, and distraction. Annals of Behavioral Medicine, 33(1), 11–21.
Kabat-Zinn, J. (1982). An out-patient program in behavioral medicine for chronic pain participants based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. General Hospital Psychiatry, 4, 33–47.
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York: Delacorte.
Kenny, M. A., & Williams, J. M. G. (2007). Treatment resistant depressed participants show a good response to mindfulness-based cognitive therapy. Behaviour Research and Therapy, 45, 617–625.
Kim, Y., Lee, S., Choi, T., Suh, S., Kim, B., Kim, C., et al. (2009). Effectiveness of mindfulness-based cognitive therapy as an adjuvant to pharmacotherapy in participants with panic disorder or generalized anxiety disorder. Depression and Anxiety, 26, 601–606.
Kingston, J., Chadwick, P., Meron, D., & Skinner, T. C. (2007). A pilot randomized control trial investigating the effect of mindfulness practice on pain tolerance, psychological well-being, and physiological activity. Journal of Psychosomatic Research, 62, 297–300.
Kraemer, H. C., Kiernan, M., Essex, M., & Kupfer, D. J. (2008). How and why criteria defining moderators and mediators differ between the Baron & Kenny and MacArthur approaches. Health Psychology, 27(Suppl 2), S101–S108.
Monroe, S. M., & Simons, A. D. (1991). Diathesis-stress theories in the context of life stress research: Implications for the depressive disorders. Psychological Bulletin, 110, 406–425.
Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100, 569–582.
Nolen-Hoeksema, S. (2000). The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. Journal of Abnormal Psychology, 109(3), 504–511.
Piet, J., & Hougaard, E. (2011). The effect of mindfulness-based cognitive therapy for prevention of relapse in recurrent major depressive disorder: A systematic review and meta-analysis. Clinical Psychology Review, 31, 1032–1040.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891.
Ramel, W., Goldin, P. R., Carmona, P. E., & McQuaid, J. R. (2004). The effects of mindfulness meditation on cognitive processes and affect in participants with past depression. Cognitive Therapy and Research, 28(4), 433–455.
Robinson, M. S., & Alloy, L. B. (2003). : Negative cognitive styles and stress-reactive rumination interact to predict depression: A prospective study. Cognitive Therapy and Research, 27, 275–291.
Segal, Z. V., Bieling, P. J., Young, T., MacQueen, G., Cooke, R., Martin, L., et al. (2010). Antidepressant monotherapy versus sequential pharmacotherapy and mindfulness-based cognitive therapy, or placebo, for relapse prophylaxis in recurrent depression. Archives of General Psychiatry, 67, 1256–1264.
Segal, Z. V., Kennedy, S., Gemar, M., Hood, K., Pedersen, R., & Buis, T. (2006). Cognitive reactivity to sad mood provocation and the prediction of depressive relapse. Archives of General Psychiatry, 63, 749–755.
Segal, Z. V., Williams, J. M., & Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse. New York: Guilford Press.
Segal, Z. V., Williams, J. M., Teasdale, J. D., & Gemar, M. (1996). A cognitive science perspective on kindling and episode sensitization in recurrent affective disorder. Psychological Medicine, 26, 371–380.
Sephton, S., Salmon, P., Weissbecker, I., Ulmer, C., Floyd, A., Hoover, K., et al. (2007). Mindfulness meditation alleviates depressive symptoms in women with fibromyalgia: Results of randomized clinical trial. Arthritis and Rheumatism, 57, 77–85.
Shapiro, S., Carlson, L., Astin, J., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 62, 373–386.
Shapiro, S., Schwartz, G., & Bonner, G. (1998). Effects of a mindfulness-based stress reduction on medical and premedical students. Journal of Behavioral Medicine, 21, 581–599.
Sotsky, S., & Glass, D. (1983). The Hamilton Rating Scale: A critical appraisal and modification for psychotherapy research. Sheffield: Paper presented at the annual convention for the Society for Psychotherapy Research.
Teasdale, J. D. (1988). Cognitive vulnerability to persistent depression. Cognition and Emotion, 2, 247–274.
Teasdale, J.D. (2004). Mindfulness-based cognitive therapy. (pp. 270-289). J. Yiend (Ed). Cognition, emotion and psychopathology: Theoretical, empirical and clinical directions. viii, 312 pp. New York, NY, US: Cambridge University Press; US.
Teasdale, J. D., Segal, Z. V., & Williams, J. M. G. (1995). How does cognitive therapy prevent relapse and why should attentional control (mindfulness) training help? Behaviour Research and Therapy, 33, 25–39.
Van Aalderen, J. R., Donders, A. R. T., Giommi, F., Spinhoven, P., Barendregt, H. P., & Speckens, A. E. M. (2012). The efficacy of mindfulness-based cognitive therapy in recurrent depressed participants with and without a current depressive episode: A randomized controlled trial. Psychological Medicine, 42(5), 989–1001.
Vettese, L. C., Toneatto, T., Stea, J. N., Nguyen, L., & Wang, J. J. (2009). Do mindfulness meditation participants do their homework? And does it make a difference? A review of the empirical evidence. Journal of Cognitive Psychotherapy, 23(3), 198–225.
Acknowledgments
This study was funded, in part, by Grant #066992 (R01: Dr. Segal) from the National Institute of Mental Health, Bethesda, MD. We thank the following colleagues for contributing to this research. Robert Cook, Lawrence Martin and Jennifer Brasch served as study psychiatrists. Shelly Ferris, Kate Szacun-Shimizu, and Karyn Hood served as study coordinators. Susan Woods and Theresa Casteels served as MBCT study therapists. Lori Hoar, Joanne Nault, Rebecca Pedersen and Zoe Laksman served as project interviewers, Bao Chau Du and Heidy Morales provided research support. Tom Buis and Andrew Pedersen provided programming and data analytic support. David Streiner provided statistical and study design consultation. Karen Brozina-Hawley assisted with proofreading and editing.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hawley, L.L., Schwartz, D., Bieling, P.J. et al. Mindfulness Practice, Rumination and Clinical Outcome in Mindfulness-Based Treatment. Cogn Ther Res 38, 1–9 (2014). https://doi.org/10.1007/s10608-013-9586-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-013-9586-4