Article Text

Abstract
Background It has been shown that the high cost of housing can be detrimental to individual health. However, it is unknown (1) whether high housing costs pose a threat to population health and (2) whether and how social policies moderate the link between housing cost burden and mortality. This study aims to reduce these knowledge gaps.
Methods Country-level panel data from Organisation for Economic Co-operation and Development (OECD) countries are used. Housing cost to income ratio and age-standardised mortality were obtained from the OECD database. Fixed effects models were conducted to estimate the extent to which the housing cost to income ratio was associated with preventable mortality, treatable mortality, and suicides. In order to assess the moderating effects of social and housing policies, different types of social spending per capita as well as housing policies were taken into account.
Results Housing cost to income ratio was significantly associated with preventable mortality, treatable mortality, and suicide during the post-global financial crisis (2009–2017) but not during the pre-global financial crisis (2000–2008). Social spending on pensions and unemployment benefits decreased the levels of mortality rate associated with housing cost burden. In countries with higher levels of social housing stock, the link between housing cost burden and mortality was attenuated. Similar patterns were examined for countries with rent control.
Conclusion Our findings suggest that housing cost burden can be related to population health. Future studies should examine the role of protective measures that alleviate health problems caused by housing cost burden.
- DEATH
- EPIDEMIOLOGY
- Health inequalities
- PUBLIC HEALTH
Data availability statement
Data are available in a public, open access repository. We used secondary data from the OECD databases. Research ethics approval was therefore carried out by the OECD. The information for data source are as follows: - OECD. Health Status. 2022. Data from: https://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_MORTALITY-OECD. Household spending (indicator). 2021. Data from: 10.1787/b5f46047-en - OECD. Social Expenditure: Aggregated data. 2022. Data from: https://stats.oecd.org/Index.aspx?datasetcode=SOCX_AGG-OECD. OECD Affordable Housing Database. 2022. Data from: https://www.oecd.org/housing/data/affordable-housing-database/
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Housing cost burden is associated with health outcomes.
It still remains unclear (1) whether high housing costs pose a threat to population health and (2) whether and how social and housing policies moderate the link between housing cost burden and mortality.
WHAT THIS STUDY ADDS
An increased level of housing cost to income was associated with preventable mortality, treatable mortality, and suicide rate in high-income countries during the post-global financial crisis.
Social spending on pension and unemployment benefits moderated the link between housing cost to income and mortality rate.
Housing policy measures, such as social housing stocks and rent control, helped to prevent people from experiencing mortality risks caused by housing cost burden.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Housing cost burden is a risk factor for population health.
Premature death, such as suicide, could be avoided through effective social spending as well as housing policy measures.
Introduction
Housing cost burden is a growing concern in many countries. Wage increases have not been able to completely catch up with an increase in housing costs.1 This negatively influences households’ ability to make ends meet as a result of a decrease in post-shelter income. Also, unpredictable and depreciated housing markets have not helped homeowners to cash out against their housing property in a timely manner.2 Rather, an increasing number of households give up becoming homeowners because a threatening housing market and strict mortgage practices may lead to economic insecurity of households.3 This in turn substantially increases the demand for rental housing than expected.4 Indeed, such a trend is pronounced in the aftermath of the global financial crisis (GFC), when many household members have been forced to quit jobs and face material hardship.5 6 Although wealthy countries have promoted the ownership of housing through policy measures, such as tax relief and interest-free down-payment assistance loans, they have not paid attention to affordable housing policies aimed at providing benefits for renters (eg, social and public housing).4 7 As such, these circumstances may endanger the living standards of socioeconomically disadvantaged households, such as lower-income households, who are at higher risks of housing insecurity.1
Housing cost burden may be related to health through three major pathways that are not necessarily mutually exclusive. First, housing cost burdened households may experience a decline in physical health, such as nutrient deficiency and (diet-related) chronic conditions,8 since housing cost burden discounts consumption of essential goods, such as healthcare and food. By delaying necessary healthcare services due to a lack of post-shelter income, households may be forced to be hospitalised in the long run.9 10 Second, housing cost burden can provoke psychological concerns. Given that housing cost burden may cause threatening situations (eg, eviction and arrears), people may feel they are not able to control their life independently. Prior studies have documented a well-established link between housing cost burden and mental health, such as depression and anxiety.11 12 Third, such stressors may influence households to attempt unhealthy behaviours, such as smoking and problematic drinking.10 These can manifest in those who tend to rely on maladaptive coping strategies for stress relief.
These potential mechanisms can be explicable at the population level. People are likely to become frustrated and threatened by a rapid increase in living expenses, and they might even perceive unaffordable housing to be unfair. As a result, this leads to hypertension and stress-related disorders,13 and violent behaviours.14 More importantly, this phenomenon revisits the notion of ‘disease (or deaths) of despair’, which displays the association between hopelessness, depression, and despair-related illness or death (eg, suicide/suicidal thoughts and alcohol-related diseases).15 Scholarship argues that disease of despair has soared remarkably during the economic transition, such as income inequality, unemployment, and poverty, since negative circumstances cause cognitive (eg, thought connected to defeat), emotional (eg, feelings of sadness), and behavioural despair (eg, self-destructive acts). Given that housing cost burden signals the cost of living crisis, disease of despair can be caused by housing cost burden.16 Consistent with this explanation, the GFC can lead to economic recession, which results in job loss, material hardship, and housing cost burden,5 6 and this can also contribute to eviction and foreclosure-related suicides.17
The relationship between housing cost burden and health can vary according to social and housing policies. First, social policies ensure all households get equal access to services that are essential to health maintenance. For example, healthcare policies, such as preventive care (e.g, immunisation, health promotion programmes, and regular health check-ups), help to promote health universally, since they directly provide necessary services and encourage people to manage their health, regardless of their socioeconomic status.18 Second, social policies, such as pensions and housing, can indirectly affect health outcomes in a way that addresses the causes of poor health. They can mitigate unequal exposure to socioeconomic and environmental risk factors by, for example, supplementing income and preventing material hardship.19 In particular, disadvantaged people, such as lower-income households and the unemployed, tend to largely benefit from these policies, since such social programmes can protect them from financial strain. This can alleviate their risks of disease and mortality. Empirical studies are congruent with these explanations, showing that social spending decreased mortality risks,20 suicide rates,21 and food insecurity.22
Using a series of the dataset for the Organisation for Economic Co-operation and Development (OECD) countries, this study examines the association between housing cost relative to income and mortality rates in wealthy countries. This study estimates fixed-effects models to gauge within-country changes in mortality rate explained by housing cost-to-income ratio. This study also investigates whether the housing mortality association varies by social spending as well as housing policies. In doing so, we assess the role of protective policies that can mitigate mortality rates in countries with housing cost burden.
Data and methods
Data were collected for OECD member countries between 2000 and 2017 to test the hypothesis that rising trends of unaffordable housing—housing cost relative to disposable income at the national level—are associated with mortality rates in wealthy countries. Our study includes subjects from 27 countries—Australia, Austria, Belgium, Canada, Czech Republic, Estonia, France, Finland, Germany, Greece, Hungary, Japan, Latvia, Luxembourg, Lithuania, the Netherlands, Norway, New Zealand, Poland, Portugal, Slovak Republic, Slovenia, Spain, Sweden, Switzerland, the UK and the USA—from 2000 to 2017 (or the latest available year). We assumed that mortality rates tend to increase as the crisis goes on, rather than at the beginning of the recession.23 Thus, we also examined whether housing cost burden is associated with mortality during pre-GFC (2000–2008) and post-GFC (2009–2017). We then evaluated whether and how different types of social spending and housing policies moderate the impact of housing on mortality rates. All data are online and freely available from the OECD.
Dependent variables: avoidable mortality and deaths of despair
This study uses two mortality outcomes available from the OECD Health Statistics24: avoidable mortality, and suicide. First, avoidable mortality rates can be divided into preventable mortality and treatable (or amenable) mortality: (1) preventable mortality can be mainly avoided through public health policy, such as prevention, from the viewpoint of social determinants of health (eg, intentional self-harm); and (2) treatable mortality can be timely prevented through healthcare intervention, including secondary treatment (eg, diabetes and appendicitis). Second, we also tested whether suicides are related to housing cost burden. Case and Deaton15 argued that behavior-related mortality (eg, mainly drug overdose and suicide) are on the rise in the USA (among the less educated whites, aged 50 to 65), since many people experience despair and hopelessness caused by economic downturn.15 Here, we use suicide rates as a proxy for deaths of despair. Note that suicides belong to the category of avoidable mortality. Mortality rate is age-standardised, number of deaths per 100 000 population, using the OECD standard population.
Independent variable of interest: housing cost-to-income ratio
To obtain country-level data on unaffordable housing, we used housing cost-to-income ratio available from the OECD database.25 Housing spending in households, which includes actual rentals (for tenants), imputed rentals (for owner-occupiers), maintenance, and others, is presented as a percentage of household disposable income (ratio of averages). The data are taken from the OECD Annual National Accounts Database on financial consumption expenditure of households. We assume that this indicator enables us to assess the degree to which households can afford housing relative to their income as socioeconomic position.
Moderating variables: social spending and housing policy measures
First, data on social spending per capita was collected from the OECD Social Expenditure Database (SOCX), which includes a range of programmes, including pension and unemployment benefits, health, and housing.26 Second, this paper examines the effect of two housing policy measures on mortality outcomes: the size of a country’s social housing stock, and the presence of rent control. We define higher social housing stock when social housing accounts for more than 10% of total housing stock (five out of 27 countries). Rent control includes (a) controls on initial rent levels or/and (b) regulated and/or negotiated rents applied across rental sectors (13 out of 27 countries). These measures capture whether a country supports socioeconomically disadvantaged people to afford rental housing. Data on housing policy measures are available from the OECD Affordable Housing Database.27
Statistical models
For analysis, we used fixed effects linear regression, which can control for unobservable time-invariant country-level confounding factors, such as social, cultural, and other conditions that are constant. That is, we can solely estimate within-country changes in mortality predicted by within-country changes in housing cost burden. Our first fixed-effects, or within-country, regression model is as follows:

Here, i is country and t is year. Mortality is mortality rate. Housing cost burden is the aforementioned measure of house cost to income.  is a vector of time-varying control variables. Control variables are composed of gross domestic product (GDP) (adjusted for purchasing power parity). They are related to both independent and dependent variables in our study, and also capture the direct effects of the recession on mortality rates.28 Year is a set of variables that control for year-specific effects on mortality. µ controls for country-specific, time-invariant error terms.
ε
is the error term that varies with country and time. Next, moving to the second step of the analysis, we: (a) tested whether (time varying) social spending moderates the relationship between housing cost burden and mortality rate using a series of interaction terms with indicators of social spending; and (b) conducted a stratified analysis to estimate the association between housing cost burden and mortality according to (time invariant) housing policies (social housing stock and rent control). For all analyses, we used the
‘xtreg
’ command in Stata/SE 15.0, and 95% confidence intervals (95% CI) were calculated based on robust standard errors.
is a vector of time-varying control variables. Control variables are composed of gross domestic product (GDP) (adjusted for purchasing power parity). They are related to both independent and dependent variables in our study, and also capture the direct effects of the recession on mortality rates.28 Year is a set of variables that control for year-specific effects on mortality. µ controls for country-specific, time-invariant error terms.
ε
is the error term that varies with country and time. Next, moving to the second step of the analysis, we: (a) tested whether (time varying) social spending moderates the relationship between housing cost burden and mortality rate using a series of interaction terms with indicators of social spending; and (b) conducted a stratified analysis to estimate the association between housing cost burden and mortality according to (time invariant) housing policies (social housing stock and rent control). For all analyses, we used the
‘xtreg
’ command in Stata/SE 15.0, and 95% confidence intervals (95% CI) were calculated based on robust standard errors.
Results
Housing cost burden and mortality
Table 1 shows the association between housing cost burden and mortality, taking into account control variables. In panel A, we saw no association between housing cost burden and mortality rates during the pre-GFC period, for preventable and treatable morality rates, respectively (β=−0.311, 95% CI −6.235 to 5.611, and β=0.815, 95% CI −3.172 to 4.801). However, in panel B, we saw a statistically significant association between housing cost burden and preventable mortality rate (β=2.808, 95% CI 0.086 to 5.530) and treatable mortality rate (β=1.554, 95% CI 0.424 to 2.683) during the post-GFC period between 2009–2017. An increase in housing cost burden is also associated with 0.552 increase in suicide rates during the post-GFC period (95% CI 0.015 to 1.090).
Association between housing cost to income, avoidable mortality, and suicide rates
Moderating roles of social spending
Table 2 presents the protective role of social spending in the link between housing cost burden and treatable mortality rate. We found that the significant interaction term between social spending on pension and unemployment benefits and housing cost burden was statistically significant for preventable mortality as an outcome (β=−0.174, 95% CI −0.344 to –0.004, and β=−0.902, 95% CI −1.700 to –0.104). In contrast, when social spending on healthcare as well as housing is above $100 per capita, the association between housing cost burden and preventable mortality rate was not mitigated. Social spending on pension has significant modifying effects on the link between housing cost burden and treatable mortality (β=−0.075, 95% CI −0.143 to –0.007), suggesting that the association between housing cost burden and preventable mortality is attenuated when social spending on pensions is higher. We repeated this analysis for social spending on unemployment benefits, healthcare, and housing but they did not significantly change the levels of treatable mortality rates associated with housing cost burden.
Association between housing cost to income and preventable and treatable mortality rate, by social spending during the post-global financial crisis (2009–2017)
Table 3 illustrates the moderating role of different types of social spending per capita on the relationship between housing cost burden and suicide rates. While social spending on pensions, healthcare, and housing was not found to be a significant moderator that mitigates risks of suicide, an additional $100 spent on unemployment benefits per capita reduces the link between housing cost burden and suicide rate (β=−0.129, 95% CI −0.256 to –0.001).
Association between housing cost to income and suicide rate, by social spending during the post-global financial crisis (2009–2017)
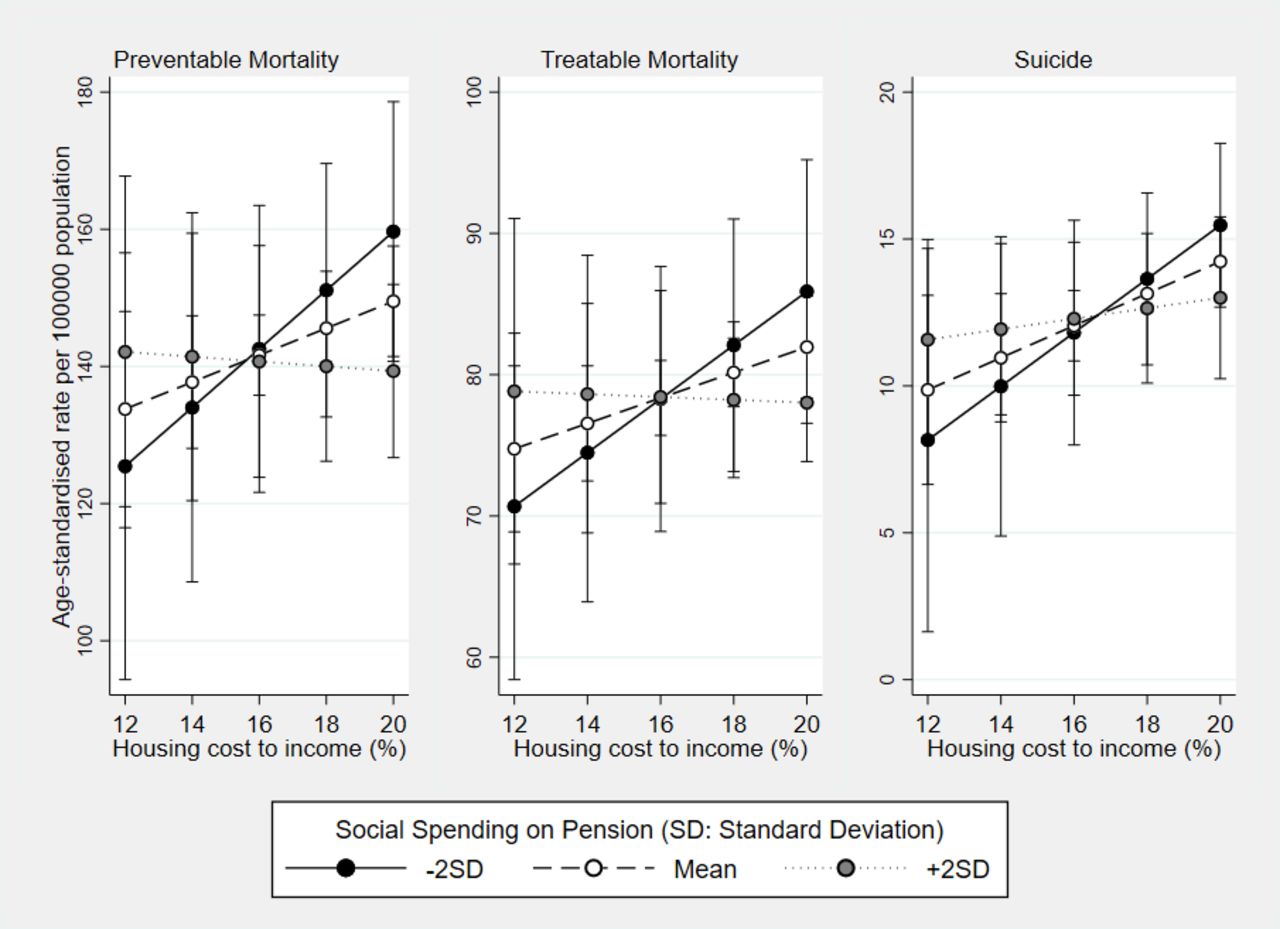
Figure 1 and figure 2 show the relationship between housing cost burden and mortality according to social spending on pensions and unemployment benefits. As social spending on pensions or unemployment benefits increases, the predicted value of mortality rates relative to housing cost to income ratio remains constant or decreases.
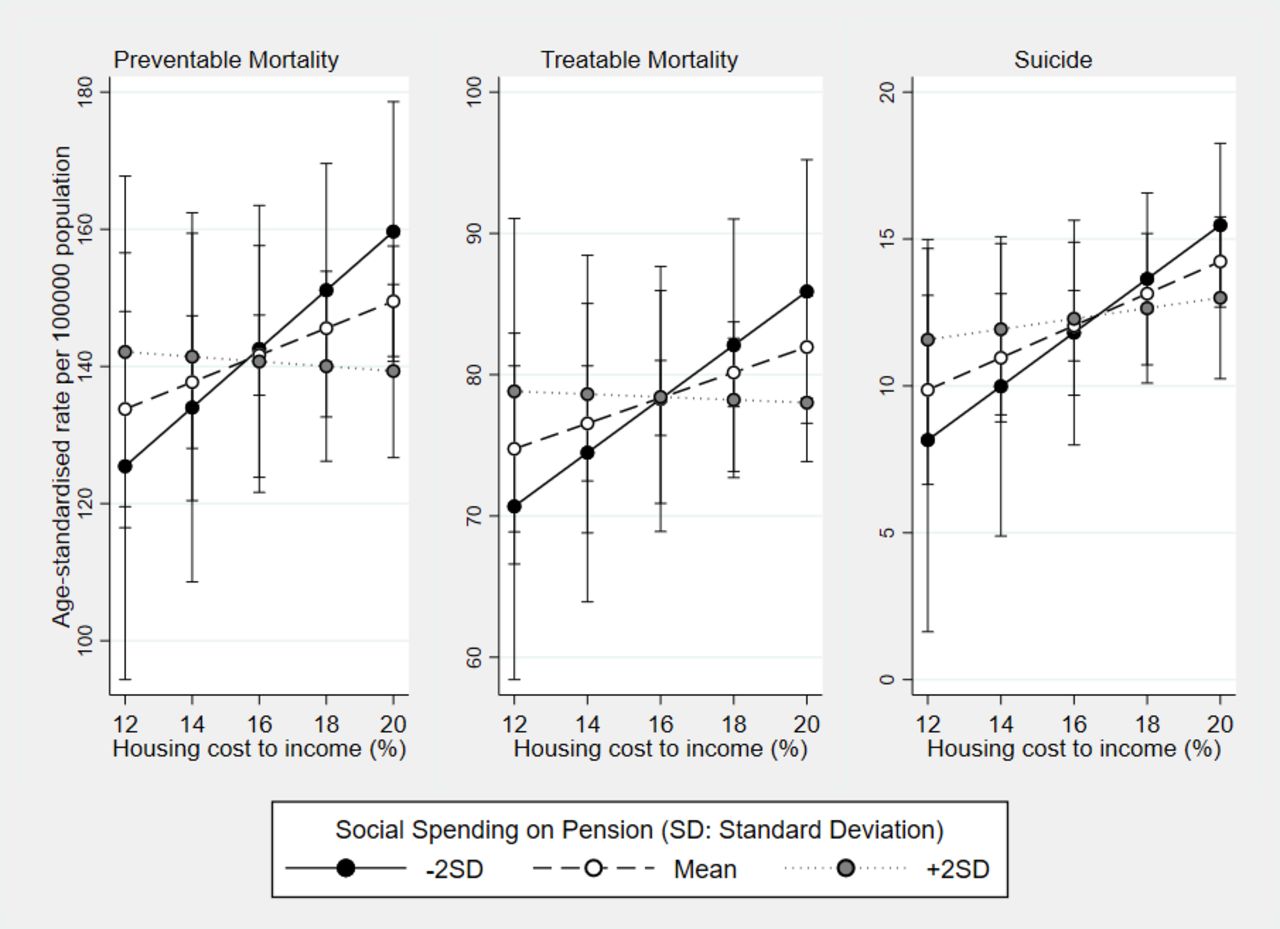
Predicted probability of mortality rate by housing cost to income and social spending on pension.
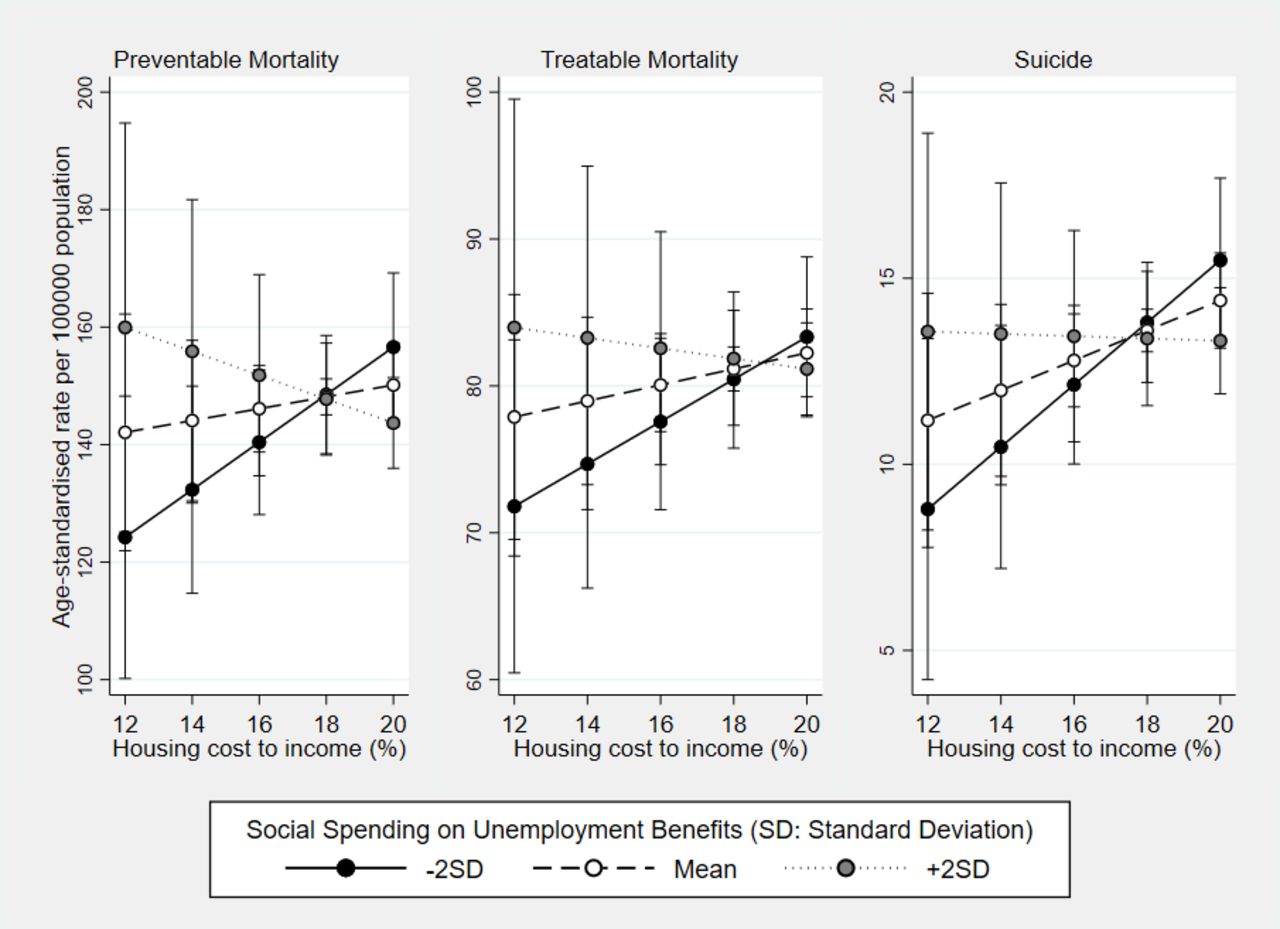
Predicted probability of mortality rate by housing cost to income and social spending on unemployment benefits.
Moderating roles of housing policy measures
We further tested whether housing policy measures change the levels of mortality rate associated with housing costs (table 4). Panel A-1 and panel A-2 indicate results for the association between housing cost burden and mortality rate by social housing stock. As shown in panel A-1, in countries with lower stocks of social housing, housing cost burden was significantly associated with preventable mortality (β=3.014, 95% CI 0.133 to 5.894), treatable mortality (β=1.484, 95% CI 0.197 to 2.772), and suicide rate (β=0.647, 95% CI 0.100 to 1.194). However, panel A-2 shows that the observed association was attenuated in countries with larger social housing stocks for preventable mortality (β=−4.891, 95% CI −7.344 to –2.437), treatable mortality (β=0.066, 95% CI −1.642 to 1.775), and suicide rates (β=−0.963, 95% CI −2.633 to 0.707).
Association between housing cost to income and mortality rate, by housing policy measures during the post-global financial crisis (2009–2017)
We found a similar pattern for rent control (panel B-1 and panel B-2). Countries that do not have rent controls still had a significant association between housing cost burden and preventable mortality (β=4.119, 95% CI 0.014 to 8.225) and suicide (β=0.877, 95% CI 0.050 to 1.704), whereas countries that do control rent levels did not show any significant association between housing cost burden and mortality, including preventable mortality (β=0.236, 95% CI −4.103 to 4.575), treatable mortality (β=0.692, 95% CI −1.336 to 2.720), and suicide (β=0.165, 95% CI −0.546 to 0.875), respectively.
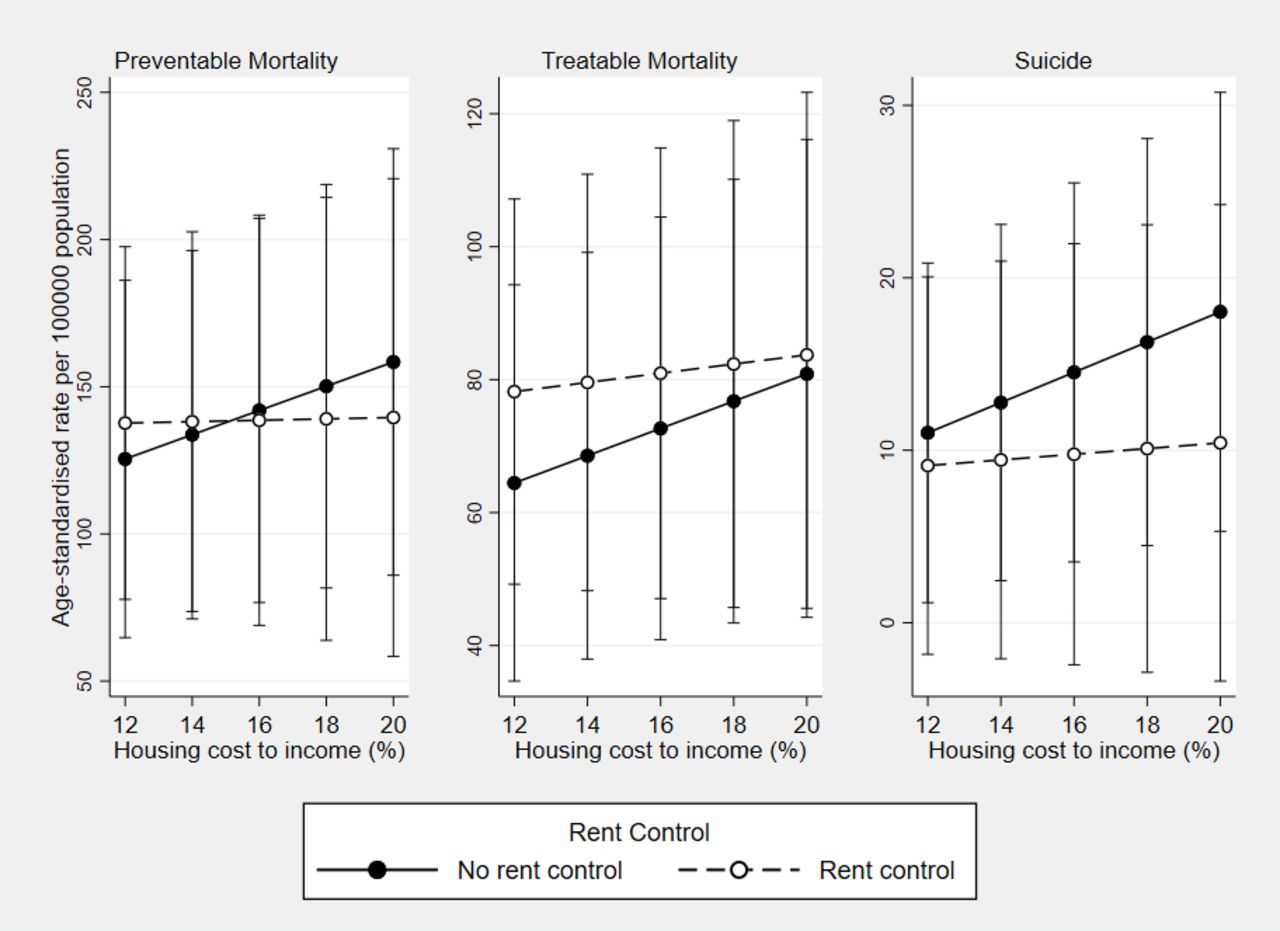
Figure 3 and figure 4 plot results of the relationship between housing cost burden and mortality according to housing measures. As shown in figure 3, the predicted value of mortality is higher when housing cost burden increases in countries with lower social housing stock, whereas the predicted value decreases or remains constant in countries with higher social housing stock. Similar patterns were found for rent control (figure 4). The association between housing cost burden and mortality is more pronounced in countries without rent control, whereas the link between housing cost burden and mortality is attenuated in countries with rent control.

Predicted probability of mortality rate by housing cost to income and social housing.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted probability of mortality rate by housing cost to income and rent control.
Discussion
Despite a well-documented link between housing cost burden and health at the individual level, whether and how housing cost burden relates to population health at the societal level is understudied. Also, few studies have examined the distinctive roles of social policies and housing policies in mitigating the link between housing cost burden and population health. The present study aims to examine whether unaffordable housing at the societal level is associated with a greater risk of avoidable mortality and deaths of despair (particularly suicide). Also, we further assessed the moderating effects of social spending and housing policy measures on the link between housing cost burden and mortality rate. There are several important findings in the foregoing analysis.
First, analyses showed that housing cost burden predicted a higher level of avoidable mortality and suicide rates in wealthy countries during the post-GFC (2009–2017). Given that not only does housing cost burden provoke concerning feelings (eg, despair and hopelessness), but this also increases risks of illness and disease,15 23 and the GFC can cause such risks to deteriorate. For example, people are more likely to be concerned about housing insecurity (eg, eviction, foreclosure, and rent arrears) in responses to housing cost burden as they are at higher risks of unemployment and wage loss in the aftermath of the GFC. It suggests that the GFC includes short- and long-term socioeconomic difficulties that can increase mortality risks.28
Second, we also demonstrated that social spending on old age and unemployment benefits was significantly associated with lower mortality rates. This finding aligns with existing studies that social spending buffers households against economic hardship.18 22 Social spending may have an important role in reducing economic hardship by helping households to earn additional income for their survival.18 19 While plausible, it should be interpreted with caution since social spending on healthcare and housing did not significantly moderate the link between housing cost burden and mortality rates. Usually, spending on healthcare can be positively associated with economic stress, in part because healthcare is a reactive measure, such as characterised by an increasing demand due to life expectancy, rather than a preventive one.
More importantly, the results of this study estimated the protective roles of housing policy measures. First, social housing for broad segments of the population appears to be associated with lower mortality risks. Social housing sectors potentially promote housing security of households because they can find out alternative options rather than being overwhelmed by priced rented housing. Second, rent controls intend to keep the living cost affordable, particularly for lower income residents, by limiting the amount that landlords can demand for leasing a home. Overall, these protective measures protect households against suffering from housing cost-induced stressors (eg, reduced post-shelter income or feeling of despair and hopelessness) by reducing the likelihood of negative events (eg, eviction) or by alleviating psychological stress.29 30 This result can highlight that premature death, such as suicide, could be avoided through effective social spending as well as housing policy measures.
There are several limitations to this study. First, the data do not provide information for housing cost burden or mortality rates by socioeconomic groups. While this study has investigated true ‘population-level’ attributes of countries and their impact on mortality consistent with concepts such as ‘social facts’ and population health,31 future studies would ideally have individual-level and country-level data so that nested analysis of individuals nested in macro contexts could be conducted. Second, although we identified the moderating effects of social spending, we did not separate different programmes within each category. For example, there are policy changes, such as expansion or reduction of social housing stock, in some countries, while others may introduce new housing programmes. More work is needed to understand how changes in particular programmes moderate the association between housing cost burden and health.
Despite its limitations, the study has several strengths. First, this is one of the first studies to assess the association between housing cost burden and mortality rates. We were able to assess within-country variations in avoidable mortality rates associated with housing cost burden. Second, this study demonstrated the extent to which protective policies might mitigate risks of mortality associated with housing cost burden. In particular, the use of unmeasured housing policy measures, such as existing social housing stock and rent control, facilitate our understanding of how indirect housing policies help to alleviate the link between housing cost burden and mortality. Our study provides compelling evidence of (1) how housing cost burden since the GFC causes mortality, and (2) why social policies remain important to improve population health.
Given that many countries have been experiencing increasing housing burden issues for many years, results of the study provide meaningful implications. Housing cost burden can cause economic insecurity, and as a result, increase mortality risks. Furthermore, this study highlights that social policies can protect households from experiencing mortality risks. Unfortunately, since there has been growing pressure to cut back on social spending after the economic crisis, an increasing number of households are faced with housing cost burden. Therefore, more research is needed to illustrate the potential mechanisms of how health inequalities associated with housing cost burden may be alleviated by social policies. In particular, housing policies need to be considered for better understanding of the protective factors for housing-health association.
Data availability statement
Data are available in a public, open access repository. We used secondary data from the OECD databases. Research ethics approval was therefore carried out by the OECD. The information for data source are as follows: - OECD. Health Status. 2022. Data from: https://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_MORTALITY-OECD. Household spending (indicator). 2021. Data from: 10.1787/b5f46047-en - OECD. Social Expenditure: Aggregated data. 2022. Data from: https://stats.oecd.org/Index.aspx?datasetcode=SOCX_AGG-OECD. OECD Affordable Housing Database. 2022. Data from: https://www.oecd.org/housing/data/affordable-housing-database/
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Twitter @marisa_c_young
Contributors G-RP: guarantor of this work, conceptualisation, methodology, formal analysis, writing – original draft, writing – review and editing. MG: supervision, writing – original draft, writing – review and editing. MY: supervision, writing – original draft, writing – review and editing. JRD: supervision, writing – original draft, writing – review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.