Article Text

Abstract
Background The high suicide rate among older adults is an important public health issue. Financial insecurity has been linked to suicidal behaviour. Despite this, as yet, there has been little research on suicide-related behaviours among older recipients of public welfare. This study will examine if suicidal ideation and suicide attempts are more prevalent in older recipients of public welfare assistance in Japan.
Methods This cross-sectional study analysed data from 16 135 adults aged ≥65 years who participated in the 2019 wave of the Japan Gerontological Evaluation Study. Information was obtained on receiving public welfare assistance, lifetime suicidal ideation and attempts, and a variety of covariates. Poisson regression analysis with robust variance estimates was used to examine associations.
Results Suicidal ideation was reported by 4.8% of the participants, while the corresponding figure for attempted suicide was 2.2%. In fully adjusted analyses public welfare recipients had an almost 1.5 times higher prevalence of lifetime suicidal ideation (prevalence ratio, PR 1.47, 95% CI 1.02 to 2.13), and an almost two times higher prevalence of attempted suicide (PR 1.91, 95% CI 1.20 to 3.04) when compared with their counterparts not receiving public welfare assistance.
Conclusion Older recipients of public welfare have a higher prevalence of suicidal behaviour in Japan. An urgent focus is now warranted on this vulnerable population to determine the specific factors underlying this association.
- SUICIDE
- AGING
- PUBLIC HEALTH
Data availability statement
Data may be obtained from a third party and are not publicly available. Data can be requested in the following website. https://www.jages.net/
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The high suicide rate among older adults is an important public health issue.
Financial insecurity has been linked to suicidal behaviour.
There has been little research on suicide-related behaviours among older recipients of public welfare.
WHAT THIS STUDY ADDS
Recipients of public welfare in Japan reported a significantly higher prevalence of lifetime suicidal ideation and suicide attempts.
An urgent focus is warranted on older recipients of public welfare assistance to determine the specific factors underlying suicidal behaviour.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
It may be beneficial to make caseworkers aware that the risk of suicidal behaviour might be elevated in welfare recipients.
Introduction
Recent research has shown that older adults not only have the highest suicide rates in many countries,1 but that suicide mortality may also be growing among older age groups in some settings. In particular, there is some evidence that suicide rates have been rapidly increasing among older adults in Asian countries, including Japan, since the middle of the 20h century.2 This is worrying as a recent government report has indicated that as many as one-third of all suicides occur in adults aged 60 years or older in Japan.3
Government-related research has shown that two of the major reasons for suicide among older people in Japan are health issues and poverty.3 This latter finding accords with previous research in other settings that has linked both financial insecurity4 and poverty5 to an increased risk of suicidal behaviour in older adults. Although the mechanisms underlying this association are uncertain, it is possible that mental health might be important in this context. Specifically, financial insecurity can affect mental health, while research from Japan has shown that individuals with moderate and severe psychological distress have a higher risk of dying from suicide.6
Determining the exact nature of the association between financial hardship and suicide among older adults in different settings is an important public health task—especially as older people are less likely to increase their income as many have already retired. In Japan, people who do not have a minimum financial level, which is determined by the government while considering age, living area and the number of household members (detailed information is provided on the government’s website7), are entitled to public welfare assistance, which aims to guarantee a ‘minimum level of healthy and cultural life’.8 In the process of evaluating an applicant’s eligibility for public assistance, a rigorous means test is conducted of their household by the local municipal welfare office to assess its assets, the applicant’s ability to work, the financial support received from relatives and the use of any other welfare services. Every individual who does not reach a minimum financial level has the right to receive public welfare assistance, although it is not automatically provided but must be applied for by those who are eligible, which means that in practice, there are some people who are eligible but do not receive public welfare assistance. Once recipients obtain a minimum financial level, they must leave the assistance programme. In 2020, in terms of the total number of households receiving public welfare assistance, 55.5% were households with older people aged 65 and above.9 Thus, currently, more than half of all Japanese households that receive public welfare assistance consist of older adults.
Despite being able to receive financial assistance through monthly income benefits and an exemption from medical care costs, it is still possible that Japanese welfare recipients may be at increased risk for a variety of detrimental outcomes.10 Research from other settings has indicated that the physical and mental health status of welfare recipients is often comparatively poor.11 For example, several cross-sectional studies in high-income countries reported that social assistance recipients had higher rates of psychological symptoms, mental disorders and physiological symptoms.12 13 In addition, longitudinal studies have reported that the transition to social assistance might also be associated with higher rates of psychological symptoms.14 15 Indeed, it is possible that the recipients of public welfare assistance might be a group with an increased risk of not only worse mental health, but also suicide, given that some research has also indicated that receiving public welfare/assistance may be linked to suicidal behaviour.
Specifically, an earlier US study reported a negative association between suicide rates and states’ spending on public welfare in the period between 1960 and 1995.16 Similarly, another study using data from 26 European countries in the period from 1980 to 2005 also found a negative correlation between social expenditure and the suicide trends in most countries.17 However, as these studies were ecological studies, the possibility of ecological fallacy cannot be discounted. In fact, individual-level studies have reported converse associations. A US individual-level study reported that recipients of the Supplemental Nutrition Assistance Programme were at increased risk of reporting serious suicidal thoughts, having a suicide plan and attempting suicide.18 In addition, a South Korean study that used data from the 2009 National Health and Nutrition Examination Survey reported that the receipt of public welfare assistance (ie, National Basic Livelihood Security assistance) was significantly associated with past-year suicidal ideation among older men, but not women.19
In Japan, the few studies to date that have examined the association between welfare and suicide have produced conflicting results. An earlier ecological study showed that the public welfare assistance rate was negatively associated with the standardised suicide mortality rate.20 In contrast, an ecological study that used data from Osaka in the 1980–1999 period reported a positive association between public welfare assistance and suicide rates among older adults.21 Relatedly, a recent empirical study also found that living on public welfare assistance was a risk factor for repeated past 12-month self-harm among Japanese adults.22 Previous studies have reported that Japan often has different trends in socioeconomic inequalities in suicide from other high-income countries. For example, in age-specific subgroup analyses in one study, in fully adjusted models none of the educational levels were statistically related to suicide in either sex except for among women aged 40–49 with the second lowest educational level, who had an even lower suicide risk compared with those women with the second highest educational level.23 In addition, another Japanese study showed that Japan and South Korea have different trends in mortality by occupational class when compared with European countries, where the authors discussed whether the results might be attributable to increasing suicide mortality rates among upper-nonmanual workers in Japan and South Korea.24 Hence, it is possible that different mechanisms might underlie the association between being a recipient of public welfare assistance and suicide in older Japanese adults. For example, recipients of public welfare assistance are more likely to be in poor health,11 which has been previously linked to suicide in older adults.25 There is also some evidence that recipients of public welfare assistance in Japan might have an increased risk of being exposed to stigma and experience discrimination,26 27 which might also increase the risk of suicidal behaviours.
However, as yet, there is a paucity of research at the individual-level that has examined suicide-related behaviours among older people in public welfare programmes including Japan’s public welfare assistance service. In response to this deficit, in this study, we aim to examine whether suicidal ideation and suicide attempts are more prevalent among older recipients of public welfare than among their non-recipient counterparts using information from the latest nationwide dataset of older Japanese adults. Based on earlier research we hypothesise that recipients of public welfare assistance may be more likely to report suicidal ideation and suicide attempts.
Methods
Study population
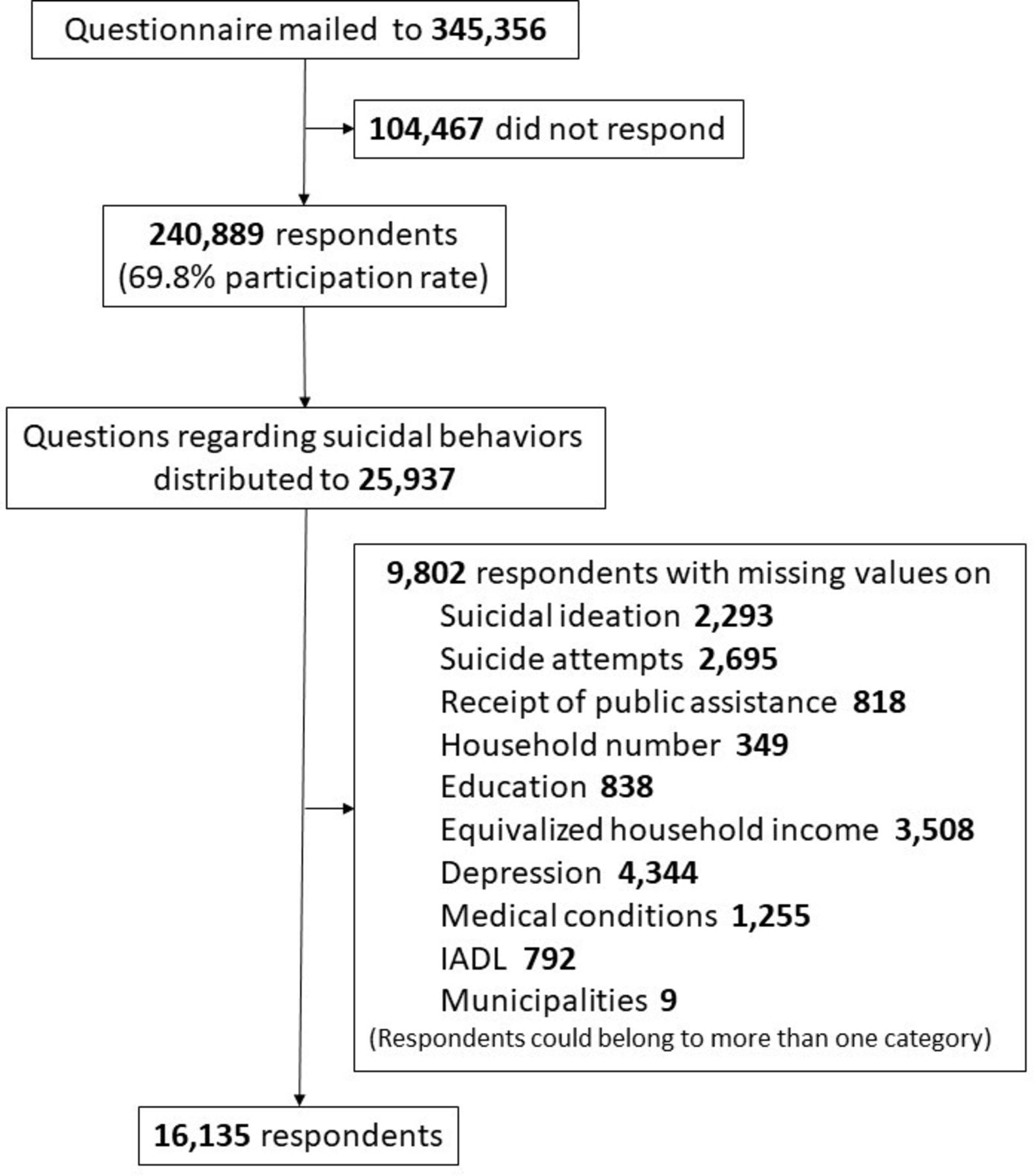
Data were used from the 2019 wave of the Japan Gerontological Evaluation Study (JAGES), which is a nationwide community-based cohort study. The JAGES cohort was established to investigate the social determinants of healthy ageing among people aged ≥65 years in Japan. In the 2019 wave, which ran from December 2019 to January 2022, self-report questionnaires were mailed to 345 356 community-dwelling individuals in 60 selected municipalities that included metropolitan, urban, semiurban and rural communities across 24 Japanese prefectures. The participants comprised a random sample of residents officially registered as living in 43 large municipalities as well as all older residents living in 17 smaller municipalities. In total, 240 889 people responded (response rate: 69.8%; range from 54.5% to 89.8%). There were eight versions of the JAGES questionnaire with each having a different subset of questions accompanying a common set of core questions, with one-eighth of the participants being randomly allocated, each subset of questions. One of the eight versions in the 2019 wave, which was distributed to 25 937 participants, had questions on suicidal behaviour. In the current study, data were used from participants without missing answers for any variables (N=16 135) (figure 1).

{kind=link}
Study flow chart. IADL, Instrumental Activities of Daily Living.
Suicidal ideation and attempted suicide
Information on lifetime suicidal ideation was obtained with the question; ‘Have you ever seriously wanted to kill yourself in your life?’, while information on lifetime attempted suicide was obtained by asking the question; ‘Have you ever tried to kill yourself?’. Individuals who responded that they ‘do not want to answer’ these questions (6.30% (n=1100) for suicidal ideation and 4.93% (n=861) for attempted suicide) were excluded from the analysis.
Public welfare assistance
Participants were asked ‘do you receive public welfare assistance now?’ There were three response options: ‘not receiving public welfare assistance,’ ‘receiving public welfare assistance’ and ‘applying for public welfare assistance’. Those who responded ‘applying for public welfare assistance’ were excluded from the analyses given their small number (0.02%, n=3).
Covariates
Previous literature was used as a guide when choosing covariates.28 Information was obtained on age (65–69, 70–74, 75–79, 80–84, 85+), sex (male vs female), the number of household members (one (ie, living alone), two and three or more), education (≤9 years vs >9 years—ie, in Japan, 9-year education is mandatory), and equivalised household income (including subsidies based on public welfare assistance and pensions; divided by ¥10 000: < ¥100, ≥ ¥100 to < ¥200, ≥ ¥200 to < ¥300, ≥ ¥300 to < ¥400 and ≥ ¥400). Depressive symptoms were measured with the Japanese short version of the Geriatric Depression Scale with 15 binary questions.29 30 The overall summed score (range: 0–15) was dichotomised, and individuals with a score of ≥5 were considered to have depressive symptoms. This measure had a good level of internal consistency (Cronbach’s alpha was 0.81). Information on Instrumental Activities of Daily Living (IADL) was obtained with five questions that inquired about: (1) using public transportation, (2) shopping for daily necessities, (3) boiling water, (4) paying bills and (5) handling banking deposits (where higher scores indicate greater functional ability). The score was dichotomised into ≤4 (lower functional ability) and 5 (maximum functional ability). Medical conditions were measured by summing the number of 16 diagnosed diseases/health conditions (range: 0–16): hypertension, stroke (eg, brain haemorrhage), heart disease, diabetes, hyperlipidaemia, respiratory disease (eg, pneumonia, bronchitis), gastrointestinal, liver or gallbladder disease, kidney or prostate gland disease, musculoskeletal disease (eg, osteoporosis, arthrosis), traumatic injury (eg, fall, fracture), cancer, blood or immune system disease, dementia (eg, Alzheimer’s disease), Parkinson’s disease, eye disease and ear disease. Participants were categorised as having either 0 conditions, 1 or 2 conditions and 3 or more conditions.
Statistical analysis
Poisson regression analysis with robust variance estimates was used to examine the association between receiving public welfare assistance and suicidal behaviour (suicidal ideation and attempts) while controlling for a range of covariates (age, sex, the number of household members, education, equivalent household income, depressive symptoms, IADL and medical conditions) to minimise bias. Five models were constructed to analyse the data in order to determine how demographic variables and other factors affect the associations. Model 1 was a model that included only the receipt of public welfare assistance. Model 2 additionally included demographic variables for age and sex. Model 3 included the same variables as in model 2 and also socioeconomic variables relating to the number of household members, education and equivalent household income. Model 4 included the same variables as in model 3 and additionally adjusted for depressive symptoms. The fully adjusted model 5 had the same variables as in model 4 and further included the IADL and medical conditions variables. To adjust for possible geographical variation, the individual municipalities were included in the analysis as dummy variables. This allowed us to control for unobserved municipal heterogeneity, such as variations in geographical, cultural, historical and social conditions at the time of the data collection. All the analyses were conducted with STATA V.16.1 MP (StataCorp). Results are presented as prevalence ratios (PR) with 95% CIs. The level of statistical significance was p<0.05 (two tailed). In order to assess the fit of the models, χ2 goodness-of-fit tests were conducted, which showed that the models fit reasonably well.
In the main analyses, we excluded people with missing values and who did not want to answer the suicidal ideation and attempted suicide questions. To check the potential effect of doing this we undertook sensitivity analyses, where we used multinomial logistic regression and included categories that comprised those individuals who did not want to answer the suicidal ideation and attempted suicide questions (reference category: Never having had suicidal ideation or attempted suicide) as well as missing categories for each variable with missing values.
Results
The analytical sample consisted of 16 135 individuals (202 welfare recipients and 15 933 non-recipients of public welfare), of whom, 4.8% (n=772) experienced lifetime suicidal ideation and 2.2% (n=355) reported attempted suicide. Among non-recipients of public welfare assistance, approximately 4.6% (n=742) experienced suicidal ideation and 2.1% (n=335) reported attempted suicide, while among recipients of public welfare assistance the corresponding figures were 14.9% (n=30) for suicidal ideation and 9.9% (n=20) for attempted suicide (table 1). Recipients of public welfare assistance were more likely to be male, live with fewer household members, have a lower level of education and lower equivalised household income. These individuals were also more likely to report depressive symptoms and medical conditions.
Demographic characteristics of the analytic sample by receipt of public welfare assistance
Receipt of public welfare assistance was associated with lifetime suicidal ideation in all of the models (table 2). In model 1 receiving welfare was associated with a 2.97 times (95% CI 2.12 to 4.17) higher prevalence of suicidal ideation, while the corresponding figures were 2.99 times (95% CI 2.14 to 4.20) in model 2 and 2.03 times (95% CI 1.44 to 2.87) in model 3. Including depressive symptoms in the analysis in model 4 led to the PR falling to 1.52 (95% CI 1.06 to 2.19). The inclusion of medical conditions and IADL in model 5 had only a small effect with the PR reducing to 1.47 (95% CI 1.02 to 2.13). In addition, older age, living with other people and having a higher education were all associated with a significantly reduced prevalence of suicidal ideation. In contrast, depressive symptoms and a high number of medical conditions were both associated with a higher prevalence of lifetime suicidal ideation.
Association between receiving public welfare assistance and suicidal ideation among older adults in Japan (N=16 135)
Receipt of public welfare assistance was associated with over a four times higher prevalence for lifetime attempted suicide in model 1 (PR: 4.30, 95% CI 2.78 to 6.66) (table 3). Adjusting for demographic variables in model 2 had little effect on the association (PR 4.38, 95% CI 2.83 to 6.79); Further adjusting the analysis for socioeconomic variables (model 3), depressive symptoms (model 4) and medical conditions and IADL (model 5) considerably attenuated this association. Nonetheless, in the fully adjusted model 5 receipt of public welfare assistance continued to be associated with almost a two times higher prevalence of lifetime attempted suicide (PR 1.91, 95% CI 1.20 to 3.04). In addition, older age, having a higher education and higher income were associated with a lower prevalence of lifetime suicidal ideation, while individuals with depressive symptoms had over a three times higher prevalence of attempted suicide (PR 3.26, 95% CI 2.62 to 4.07).
Association between receiving public welfare assistance and attempted suicide among older adults in Japan (N=16 135)
Further calculations showed that for suicidal ideation and attempted suicide the population attributable fractions were 2.7% and 4.4%, respectively, indicating that this was the prevalence of suicidal ideation/behaviour associated with receiving public welfare assistance.
In sensitivity analyses that included those individuals who did not want to answer the suicide questions and missing categories for each covariate with missing values, the results were consistent with those obtained in the main analyses. In addition, the results also showed that public assistance recipients were more likely to report suicidal ideation and suicide attempts compared with non-recipients of public assistance among those people who did not want to answer the suicide questions. (The results are available on request).
Discussion
This study analysed data from a sample of 16 135 community-dwelling older adults aged ≥65 years in Japan to examine whether suicidal ideation and suicide attempts are more common among older recipients of public welfare assistance than among their non-recipient counterparts. Results from Poisson regression analyses with robust variance estimates showed that older recipients of public welfare had a significantly higher prevalence of reporting lifetime suicidal ideation and suicide attempts. This association was robust even after adjusting for a range of covariates that included depressive symptoms, a well-known risk factor for suicidal behaviour.28 The results of this study are in line with a previous individual-level study from the USA, which reported a relationship between the receipt of public welfare and suicidal behaviour18 and an earlier ecological study in Japan which showed a positive association between public welfare assistance and suicide rates among older people.21 This study builds on and extends earlier Japanese research by using individual-level data to show that the receipt of public welfare is linked to a higher prevalence of both suicidal ideation and attempts among older adults in Japan.
Several mechanisms might underlie the association between receiving welfare and engaging in suicidal behaviour. For example, there is some evidence that Japanese welfare recipients may be more likely to suffer from stigma and discrimination due to receiving public welfare assistance.26 27 This might be important as there is some evidence that discrimination is significantly associated with lifetime suicidal thoughts, plans and attempts.31 Recipients of welfare might also have been more likely to have experienced economic hardship, which is related to suicidal behaviours.5 Furthermore, governmental statistics also show that recipients of public welfare tend to engage in worse health behaviours such as heavy drinking and have lifestyle diseases—both of which might be linked to suicidal behaviour.25 32 33
This study has several limitations. First, as this is a cross-sectional study causal relationships could not be established. Second, we cannot guarantee that there was a temporal concordance between the main variables examined in this study as data were collected on the participants’ lifetime experience of suicidal behaviour but about their current receipt of public welfare. Third, since data were self-reported, there is the possibility that bias may have been an issue, including reporting bias and non-response bias with suicidal behaviours being especially likely to have been under-reported (ie, socially desirable responding),34 while those who have more transient lifestyles and have ongoing health issues tend not to participate in surveys. Indeed, national statistics show that 2.9% of people aged 65 years and older were receiving public welfare as of 2018,35 while only 1.2% of our study sample were public welfare recipients. Thus, this bias might also account for the lower percentage of welfare recipients seen among our study sample. Therefore, it is possible that the study sample might not have been fully representative of all older adults in Japan and the results might not be valid for this population overall. Fourth, this study did not use data from those who responded that they ‘do not want to answer’ the questions on suicidal ideation (6.3%) and attempted suicide (4.9%). This may have been problematic as 13.4% of public welfare assistance recipients were non-responders for suicidal ideation while this figure was only 6.2% for non-recipients, while the corresponding figures for attempted suicide were 11.2% and 4.8%, respectively. Given this we might have underestimated the strength of the relationship between receiving welfare and suicidal behaviour. Fifth, we had no information on the length of the time period recipients had been receiving welfare assistance. This might have also been important for the observed associations. Sixth, we were only able to control for depressive symptoms but not consider other mental illnesses such as anxiety and post-traumatic stress disorders even though they might have been important for the associations. Thus, unmeasured confounders could have potentially biased our findings. Finally, we were not able to consider the life course trajectory in this study, which could have potentially been very different between public assistance recipients and non-recipients, indicating a possible risk of bias. Future studies that consider the life course trajectory when examining these associations will thus be needed.
The finding that being a recipient of public welfare assistance is associated with a higher prevalence of suicidal behaviour may have important policy implications. In particular, the results of our study underline the potential significance and importance of additional support for health maintenance among welfare recipients, as seen recently with the introduction of the ‘health management support programme for welfare recipients’ in Japan in 2021 that was mandated to regional welfare offices.36 In relation to this, the findings of this study suggest that it may be beneficial to make those supporting public welfare recipients aware that the risk of suicidal behaviour might be elevated in some welfare recipients. More specifically, as the recipients of public welfare are visited regularly by caseworkers it is possible that this ‘intervention’ could be more precisely tailored to function as a form of emotional/social support which has been previously linked to better mental health and reduced suicidal behaviour among older adults in Japan.37 Having said this, as the workload of caseworkers is already heavy in terms of the support they provide for recipients, it is essential that concrete systems/policies be established to promote partnerships between healthcare professionals and welfare offices, as is seen in other settings such as in relation to social prescribing and patient navigation.38 39 It is also important to ensure that the actual welfare provided (income) is sufficient enough to guarantee that recipients are not living in poverty or can slip into poverty or experience financial destitution, which may have been a cause of suicidal behaviour4 5 in our study. Finally, in order to prevent the receipt of public welfare assistance being associated with discrimination and stigma, information should be disseminated at a societal level about the importance of the welfare system and public welfare assistance in ensuring that everyone in a society has a basic minimum standard of living.
In conclusion, this study found that recipients of public welfare in Japan had a significantly higher prevalence of reporting lifetime suicidal ideation and suicide attempts. Future research should examine whether the various types of support can play a protective role for older welfare recipients who are at risk for suicide-related behaviour. In addition, it is also important to determine the specific reasons for the increased risk of suicidal behaviours among public welfare assistance recipients using longitudinal data so that evidence-based policies can be implemented to address this situation.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data can be requested in the following website. https://www.jages.net/
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committees on Human Subjects at the National Center for Geriatrics and Gerontology (No. 992), the Faculty of Medicine at Chiba University (No. 2493), the Faculty of Medicine at the University of Tokyo (No. 10555) and the Graduate School and Faculty of Medicine at Kyoto University (No. R3153). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Twitter @DiceNish, @naoki_kondo
Contributors SK, AS and NK conceptualised and designed the study. SK analysed the data and prepared the manuscript. DN, KU, MS and TO critically reviewed the manuscript and provided comments. SK, AS and NK finalised the manuscript. All authors read and approved the final manuscript. SK is the guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was supported by Grant-in-Aid for JSPS Fellows (JP20J01910), JSPS KAKENHI Grant Number (JP22K17266, JP15H01972), Health Labour Sciences Research Grant (H28-Choju-Ippan-002), Japan Agency for Medical Research and Development (AMED) (JP17dk0110017, JP18dk0110027, JP18ls0110002, JP18le0110009, JP20dk0110034, JP20dk0110037), Open Innovation Platform with Enterprises, Research Institute and Academia(OPERA, JPMJOP1831)from the Japan Science and Technology (JST), a grant from Innovative Research Program on Suicide Countermeasures (1-4), a grant from Sasakawa Sports Foundation, a grant from Japan Health Promotion and Fitness Foundation, a grant from Chiba Foundation for Health Promotion and Disease Prevention, the 8020 Research Grant for fiscal 2019 from the 8020 Promotion Foundation (adopted number: 19-2-06), a grant from Niimi University (1915010), grants from Meiji Yasuda Life Foundation of Health and Welfare and the Research Funding for Longevity Sciences from National Center for Geriatrics and Gerontology (29-42, 30-22).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.