Article Text

Abstract
Background While many high-income countries including Australia have successfully implemented a range of tobacco control policies, smoking remains the leading preventable cause of cancer death in Australia. We have projected Australian mortality rates for cancer types, which have been shown to have an established relationship with cigarette smoking and estimated numbers of cancer deaths attributable to smoking to 2044.
Methods Cancer types were grouped according to the proportion of cases currently caused by smoking: 8%–30% and >30%. For each group, an age–period– cohort model or generalised linear model with cigarette smoking exposure as a covariate was selected based on the model fit statistics and validation using observed data. The smoking-attributable fraction (SAF) was calculated for each smoking-related cancer using Australian smoking prevalence data and published relative risks.
Results Despite the decreasing mortality rates projected for the period 2015–2019 to 2040–2044 for both men and women, the overall number of smoking-related cancer deaths is estimated to increase by 28.7% for men and 35.8% for women: from 138 707 (77 839 men and 60 868 women) in 2015–2019 to 182 819 (100 153 men and 82 666 women) in 2040–2044. Over the period 2020–2044, there will be 254 583 cancer deaths (173 943 men and 80 640 women) directly attributable to smoking, with lung, larynx, oesophagus and oral (comprising lip, oral cavity and pharynx) cancers having the largest SAFs.
Interpretation Cigarette smoking will cause over 250 000 cancer deaths in Australia from 2020 to 2044. Continued efforts in tobacco control remain a public health priority, even in countries where smoking prevalence has substantially declined.
- health services
- neoplasms
- smoking
- mortality
- prevention
Data availability statement
Data are available upon reasonable request. The tabulated data on cancer mortality are available from the Australian Institute of Health and Welfare at https://www.aihw.gov.au/. Access restrictions apply to the National Drug Strategy Household Surveys data on smoking behaviour. Approved release of these data can be obtained through an application to the Australian Institute of Health and Welfare.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A range of tobacco control interventions have reduced smoking prevalence over time in Australia. Prior analyses have estimated the associated past and future reductions in lung cancer mortality.
There are limited data on long-term projections of mortality rates for all smoking-related cancer types or the estimated all-cancer deaths directly attributable to cigarette smoking.
WHAT THIS STUDY ADDS
Taking into account historical smoking patterns, this study estimated mortality rates for all smoking-related cancers to 2044 in Australia. The findings predict that there will be more than 250 000 cancer deaths directly attributable to smoking in the period 2020–2044.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These projections can serve as benchmarks against which to measure the impact of future cancer control initiatives.
This study highlights the ongoing and future impact of smoking on the cancer burden. Continued efforts in tobacco control remain an urgent public health priority, even in countries such as Australia, where smoking prevalence has substantially declined.
Introduction
Decreasing trends in cigarette smoking and tobacco consumption have been observed in many high-income countries that have successfully implemented tobacco control initiatives, including Australia. However, globally over one-third of men and approximately 1 in 10 women were current smokers in 2015,1 and estimates from the most recent Global Burden of Disease study suggest that tobacco smoking killed more than 8.7 million people in 2019.2 Australia has successfully implemented many tobacco control interventions, which have resulted in a marked decline in the prevalence of smoking in Australian men since the 1950s and in women since the 1980s. There has been a subsequent reduction in lung cancer mortality,3 although projections indicate that the number of lung cancer deaths will continue to be substantial in 2040.3 Over many years, from early studies establishing the association with lung cancer4 5 through the International Agency for Research on Cancer (IARC) monograph6 to a systematic review in 2013,7 smoking has become causally associated with an increasing number of cancers, including lung, larynx, liver, oesophagus, bladder, pancreas, lip, oral cavity, pharynx, stomach, colorectum, kidney, cervix, uterus, myeloid leukaemia, gallbladder and biliary tract. These cancers at least in part attributable to smoking are hereafter referred to as ‘smoking-related cancers’. However, little is known about past and future trends in mortality rates for cancers other than lung cancer in relation to smoking.
A number of different statistical models have been developed and used to project future cancer mortality rates, ranging from a simple assumption of a constant cancer mortality rate to more complex methods such as age-period-cohort (APC) models, and extended methods that account for changes in exposure to risk factors.8 To project lung cancer mortality rates, we have previously validated a generalised linear model (GLM), which included tobacco consumption as a covariate.3 This method may also be applied to other cancers with an established association with cigarette smoking. We previously developed statistical models for the projections of all cancers combined and 21 individual cancer types.9 However, to our knowledge, there have not yet been any published studies that report long-term projections of mortality rates for all smoking-related cancers in relation to past smoking behaviour, nor have there been estimates of the future number of cancer deaths directly attributable to smoking in Australia.
In this study, we have projected Australian mortality rates for all smoking-related cancers combined by taking into account historical smoking patterns, and also estimated the number of deaths from these cancers directly attributable to cigarette smoking for the period 2020–2044.
Methods
Data sources
We obtained national tabulated data on the numbers of deaths from cancer in Australia from 1955 to 2019 by sex, age and calendar year from the WHO’s Mortality Database10 sourced from the Australian Institute of Health and Welfare (online supplemental material 1).11 Australian population data by sex, 5-year age group and calendar year from 1955 to 2044 (Series B, based on medium population growth) were obtained from the Australian Bureau of Statistics.12 13 Smoking data for 1945–2004 were obtained from the International Smoking Statistics Web Edition14 and the National Drug Strategy Household Survey (NDSHS) data for 2007–2019.15 Sex–age–period-specific smoking prevalence and cigarette tar exposure per capita in Australia were reconstructed backwards to 1920 and forwards to 2044.3 For the purposes of our analyses, all data were aggregated into 5-year age groups and 5-year calendar periods. All age-standardised rates were standardised to the 2001 Australian population. Here, we use the terms men and women to denote males and females, given that the majority of deaths occur in people over the age of 18 years.
Supplemental material
Selected cancer types and grouping of smoking-related cancers
We included all cancers listed by the IARC as causally related to smoking,6 and also included gallbladder and biliary tract cancer based on more recent evidence.7 We grouped cancer types into two groups according to the current proportion of cases caused by smoking. These groups were cancer types with >30% of cases currently caused by smoking, including lung, bladder, larynx, oesophagus and oral (comprising lip, oral cavity and pharynx) cancers and cancer types with 8%–30% of cases currently caused by smoking, including liver, stomach, gallbladder and biliary tract, pancreas, colorectal, kidney and ureter, myeloid leukaemia, uterus, cervix and ovarian cancers (online supplemental table S1).6
Statistical methods used for mortality rate projections
The outcomes of interest were the mortality rate and the number of deaths attributable to smoking for all smoking-related cancers. The selection of the most appropriate statistical projection model for each cancer group was based on the Bayesian Information Criterion and model validation using observed mortality rates (online supplemental material 2). For the group of cancer types with >30% of cases currently caused by smoking, GLMs including age, cohort and cigarette tar exposure (lagged 27 years for men and 29 years for women) were used to project mortality rates (online supplemental figure S1).3 For the group of cancer types with 8%–30% of cases currently caused by smoking, APC models incorporating cigarette smoking exposure (lagged 32 years for men and 33 years for women)16 were used to project mortality rates (online supplemental figure S2). The estimated numbers of deaths for these two cancer groups were then combined to estimate the overall projected mortality rate for all smoking-related cancers. To project the mortality rate for lung cancer, we used previously validated GLMs including age, cohort and cigarette smoking exposure.3 A standard APC model was used to project the mortality rate for each remaining cancer types (online supplemental table S2).
Supplemental material
Number of cancer deaths directly attributable to smoking
The smoking-attributable fraction (SAF) is the proportion of deaths that are directly attributable to smoking.17 The total number of cancer deaths directly attributable to smoking for people aged 35 years and above was calculated by multiplying the SAF and the corresponding numbers of cancer deaths for each cancer type, age group and sex category and then aggregating these.
The SAF is calculated using the standard formula:

where  is the prevalence of current smokers and
is the prevalence of current smokers and  is the prevalence of former smokers (both available from the NDSHS data),
is the prevalence of former smokers (both available from the NDSHS data),  and
and  are the relative risks of death from cancer for current and former smokers compared with never smokers, respectively. Sex-specific relative risks for each cancer type were derived from the American Cancer Society’s Cancer Prevention Study II (CPS-II).17 18 Due to the lack of reliable relative risk data, we did not calculate the numbers of smoking-attributable deaths for ovarian, gallbladder and biliary tract cancers. Due to the limited data on the past prevalence of current and former smokers in the population, smoking-attributable deaths were only calculated from 2000 onwards. All statistical analyses were performed using Stata (V.17, Stata Corporation, College Station, Texas).
are the relative risks of death from cancer for current and former smokers compared with never smokers, respectively. Sex-specific relative risks for each cancer type were derived from the American Cancer Society’s Cancer Prevention Study II (CPS-II).17 18 Due to the lack of reliable relative risk data, we did not calculate the numbers of smoking-attributable deaths for ovarian, gallbladder and biliary tract cancers. Due to the limited data on the past prevalence of current and former smokers in the population, smoking-attributable deaths were only calculated from 2000 onwards. All statistical analyses were performed using Stata (V.17, Stata Corporation, College Station, Texas).
Results
Projections of mortality rates for cancers related to smoking
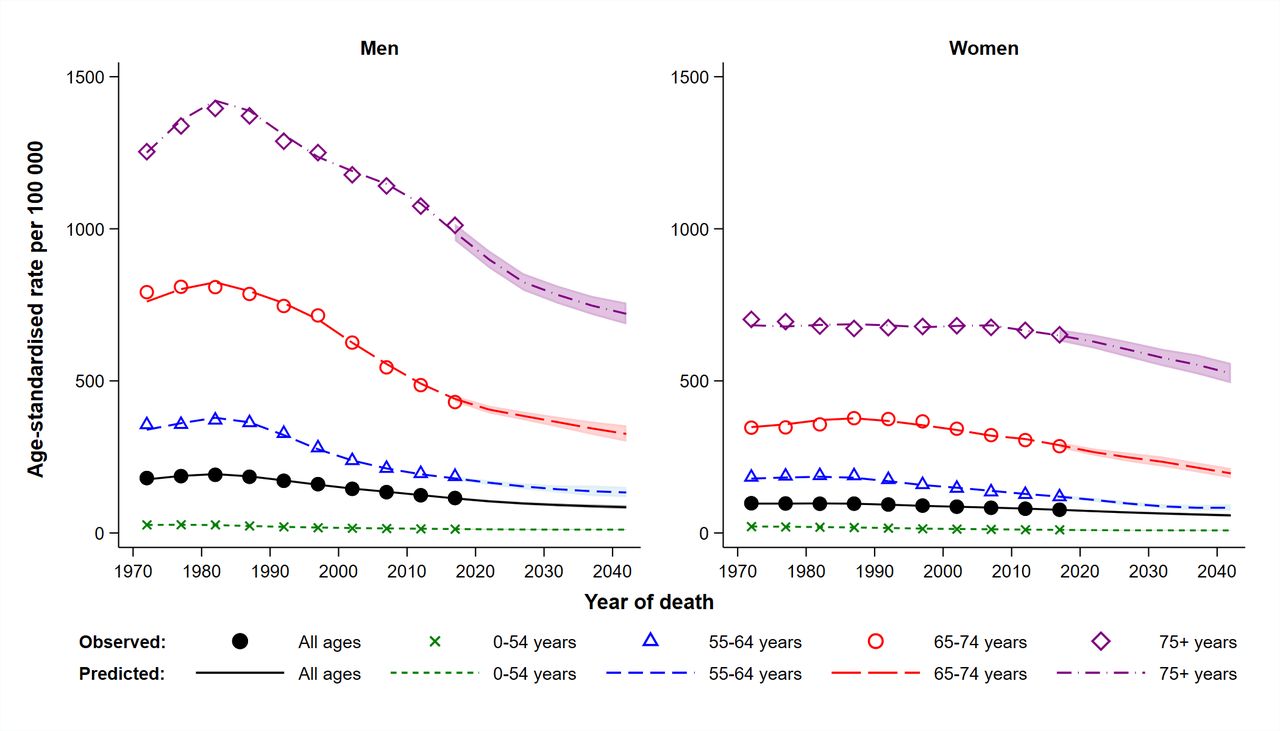
For both men and women, the age-standardised mortality rates for all smoking-related cancers combined are projected to decline continuously over the period 2015–2019 to 2040–2044, from 114.1 to 84.8 per 100 000 men and 76.5 to 57.8 per 100 000 women (figure 1 and table 1). For both men and women, the mortality rates are consistently lowest (<15 per 100 000) for those aged less than 55 years. The mortality rates for men in the older age groups showed a steady decline from the mid-1980s. Different patterns were observed for women, with lower rates overall and the decline occurring at a slower pace and starting later than was observed for men (figure 1). The decline in the mortality rate for women aged 55–64 years began in the 1990s, but for women in the older age groups (65 years and above) the decline began 5–20 years later.
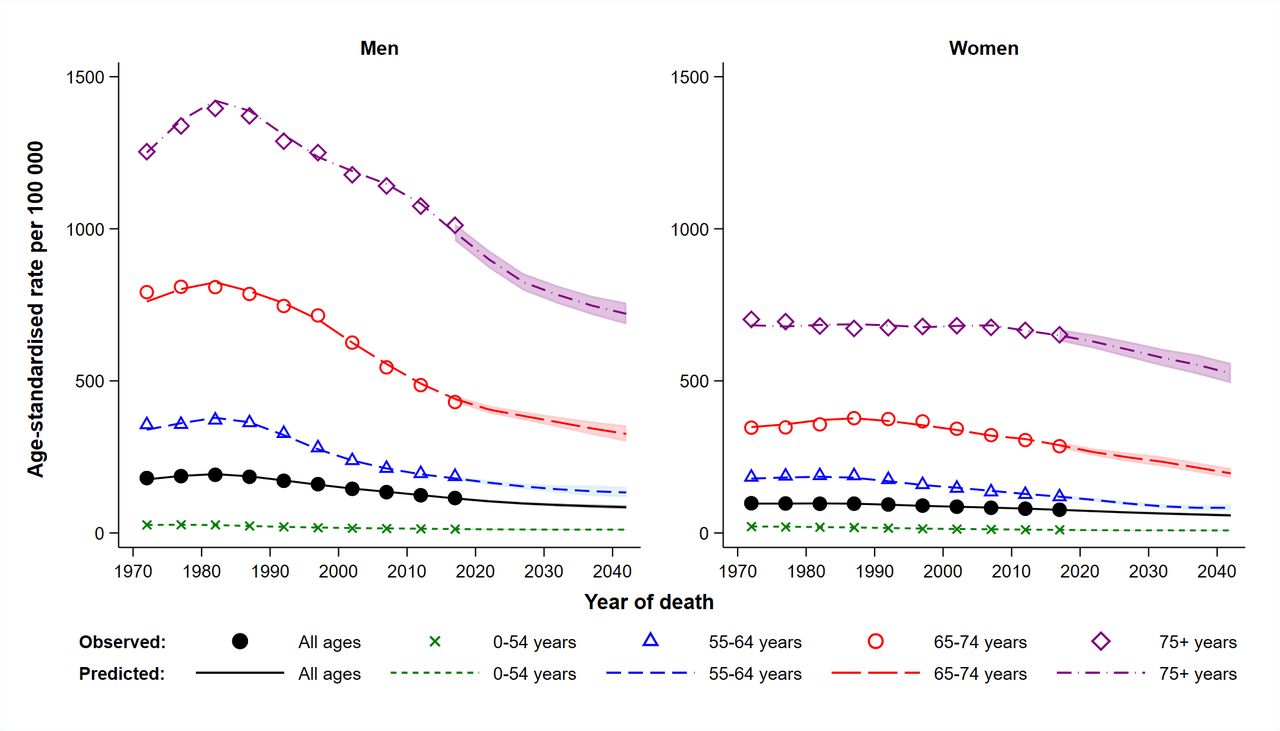
Observed and projected age-standardised mortality rates for smoking-related cancers by age group and sex in Australia, 1970–2044. All rates are age-standardised to 2001 Australian population. The shaded area represents the 95% confidence interval.
Observed and predicted age-standardised mortality rates and numbers of deaths (with 95% confidence intervals) from all smoking-related cancers combined by sex and 5 year period, 2015–2044
Despite the decreasing mortality rates, due to population growth and ageing, the overall number of smoking-related cancer deaths is projected to increase by 31.8% (28.7% for men and 35.8% for women) from 138 707 (77 839 men and 60 868 women) in 2015–2019 to 182 819 (100 153 men and 82 666 women) in 2040–2044 (table 1).
Estimated number of cancer deaths directly attributable to smoking
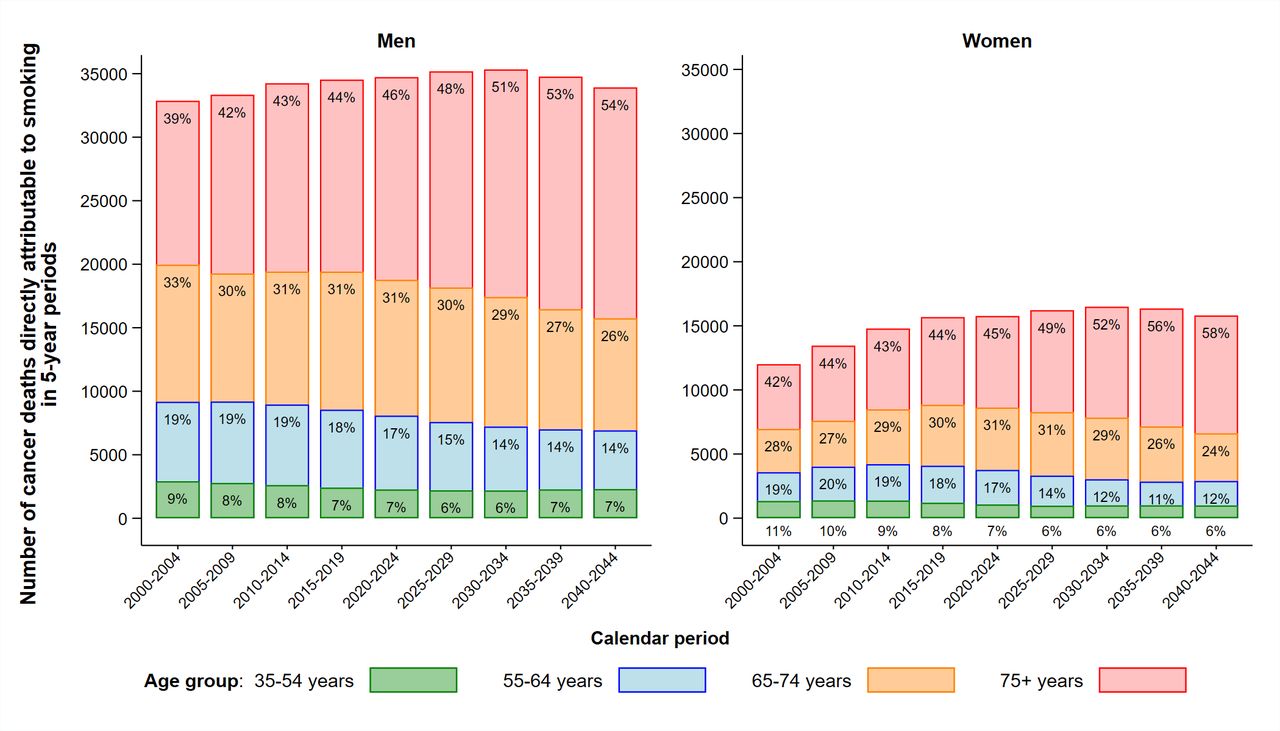
Figure 2 shows the total estimated numbers of cancer deaths directly attributable to smoking by age group and sex for people aged 35 years and above in Australia in 2000–2044. For both men and women, the numbers of cancer deaths directly attributable to smoking for the youngest age group (35–54 years) are consistently low (≤11% of the total), and the numbers of cancer deaths directly attributable to smoking for the 55–64 and 65–74 year age groups showed a steady decline over the projection period 2020–2044. In contrast to the younger age groups, the numbers of cancer deaths directly attributable to smoking for those aged 75 years and above are expected to continue to increase to 2044. We estimate that in Australia over the period 2020–2044, there will be 254 583 cancer deaths (173 943 men and 80 640 women) directly attributable to smoking, representing 32.3% (37.2% for men and 25.2% for women) of the total deaths from cancers, which are known to be related to smoking (table 2). Lung cancer is estimated to remain the cancer type with the largest number of deaths directly attributable to smoking, accounting for 61.7% of the total cancer deaths directly attributable to smoking in 2020–2044 (figure 3 and table 2). For every smoking-related cancer type, the SAF decreased over the period 2000–2044 (table 2). Cancer types with the largest SAFs for the period 2020–2044 are cancers of the lung, larynx, oesophagus and oral cancers (comprising lip, oral cavity and pharynx).
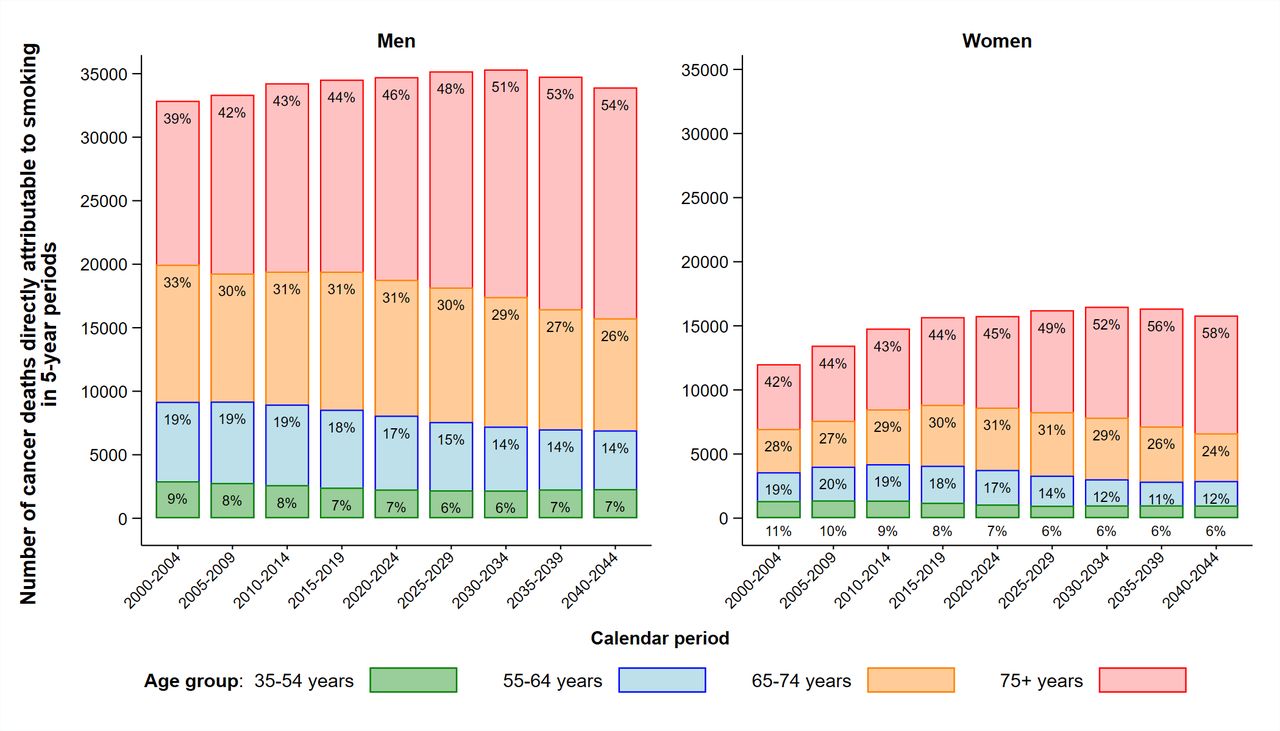
Total numbers of cancer deaths directly attributable to smoking by age group and sex in Australia, 2000–2044.

{kind=link}
{kind=link}
{kind=link}
Numbers of cancer deaths directly attributable to smoking by cancer type, sex and age group to 2044 in Australia, ranked by the number of cancer deaths directly attributable to smoking in 2015–2019.
Observed and projected numbers of cancer deaths directly attributable to smoking and smoking attributable fraction by cancer type for people aged 35 years and above in 2015–2044 in Australia, ranked by the total number of cancer deaths directly attributable to smoking in 2015–2019
Discussion
Using Australia as an example of a high-income country with successfully implemented tobacco control initiatives, resulting in declining cigarette smoking and tobacco consumption, we have projected the future national burden of cancer deaths from smoking-related cancers. Our projections indicate that mortality rates for smoking-related cancers for both men and women in Australia are expected to continuously and gradually decline to 2044, to a large extent reflecting the success and velocity of past and current tobacco control measures. Despite these declining mortality rates, our results project that the overall number of deaths from smoking-related cancers are likely to increase by 32% over the period 2015–2019 to 2020–2044, as a result of the ageing population and increasing population size.
We estimate that there will be more than 250 000 cancer deaths directly attributable to smoking between 2020 and 2044, accounting for one-third of the total number of deaths from smoking-related cancers. Fortunately, the number of cancer deaths directly attributable to smoking for people aged less than 75 years is expected to decrease over the 25 years to 2044. A decline in the proportion of deaths directly attributable to smoking was apparent overall and for each individual cancer type, although the SAFs were still high for cancers of the lung, larynx, oesophagus and oral cancers. Lung cancer is estimated to remain the leading cause of smoking-related cancer death in Australia and will account for 61.7% of the total estimated number of cancer deaths directly attributable to smoking over the period 2020–2044. Notably, cancer is only one of many health problems associated with tobacco smoking.17 19 The Australian Burden of Disease study estimated that cancer was responsible for ~56% of all deaths directly attributable to smoking in Australia in 2018,20 thus the total number of deaths directly attributable to smoking in Australia will be substantially greater than estimated in this work for cancer alone.
Given the strong association between smoking and lung cancer mortality,21 there has been increasing interest in incorporating information on smoking in lung cancer mortality projections.3 8 However, these methods have not been used for projecting mortality rates for all smoking-related cancer types. By grouping smoking-related cancer types together based on the proportion of cases currently attributable to smoking, we were able to include historical and current smoking patterns in the projection models for cancer types, which could not be individually fitted using such a model due to the small numbers of deaths.9 We confirmed that the models were reliable by providing validation of the 20-year projections using observed data. As there is a 26–33 year lag between changes in smoking behaviour and any subsequent impact on cancer mortality rates,3 our projections to 2044 are likely to be robust as they are based on past tobacco consumption up to 2019.
The successful implementation of a range of tobacco control programmes has been crucial in the reduction in smoking prevalence and cigarette consumption evident in many high-income countries, including Australia.22 23 The findings from this study confirmed that historical patterns in tobacco smoking are a strong predictor of mortality rates for smoking-related cancers.3 The earliest research that revealed the link between smoking and cancer was published in the 1950s4 5 and eventually initiated the introduction of tobacco control interventions internationally.3 4 In Australia, mandatory health warnings on all cigarette packs were first implemented in 1973, and all cigarette advertising on radio and television was banned in 1976 with more comprehensive advertising and promotion bans in subsequent decades.24 More recent tobacco control measures in Australia include media campaigns, plain packaging, a 25% increase in tobacco excise in 2010 and an annual 12.5% increase in tobacco excise implemented from 2013 to 2020.24 All these measures have resulted in decreases in the prevalence of smoking, beginning in the 1950s for Australian men and in the 1980s for Australian women.3
Despite the success of tobacco control in Australia, the most recently published estimates of smoking prevalence in Australia show that over 11% of Australians aged 18 years and over are daily smokers and that an additional 1% smoke less frequently (noting that these data have been collected during the COVID-19 pandemic and may not be directly comparable to previous estimates).25 Data have also shown considerable differences in smoking behaviour across sociodemographic groups in Australia, with higher smoking rates observed for those of lower socioeconomic status or with a lower level of education26 and also among Aboriginal and Torres Strait Islander peoples and other priority populations.27–29 The estimates presented demonstrate the effects of ‘business as usual’ and show that continuing current tobacco control efforts are likely to result in relatively slow declines in cancer rates and in increasing deaths over time. Without accelerated action, supported by adequate resources, it is expected that the positive effects of existing tobacco control measures will lessen over time.30 There are also concerns regarding the impacts of online promotion,22 31 and that electronic cigarettes (e-cigarettes) and other novel tobacco products may have an adverse impact on smoking initiation rates.32 It is, therefore, important to strengthen and implement even more effective tobacco control programmes as soon as possible. A comprehensive time series analysis of the effectiveness of tobacco control measures in Australia in 2008 concluded that the most effective population level interventions were price control through excise and hard-hitting mass media antismoking campaigns, with a synergistic benefit when used in tandem.33 Over the past decade, while excise has reached best-practice levels, there has been little or no commensurate investment in antismoking campaigns, other than targeted campaigns to tackle smoking by Aboriginal and Torres Strait Islander peoples.34
In this study, only cancer types which have been shown to have an established relationship with cigarette smoking were included,6 but it should be acknowledged that smoking may also increase mortality from cancers for which there is limited evidence that smoking is a risk factor.35 For example, previous studies reported that smokers diagnosed with prostate cancer have poorer survival outcomes than non-smokers,17 and it has also been reported that women who were smokers at the time of breast cancer diagnosis are more likely to develop systemic recurrence after surgery.36 In addition, smoking can decrease the effectiveness of many cancer treatments, so quitting smoking is likely to have a range of benefits for smokers who are diagnosed with cancer.37 Furthermore, as tobacco smoking is also known to increase the risk of developing many non-cancer diseases,38 which are not included in this study, the wider benefits from tobacco control on all deaths directly attributable to smoking will be even greater than we have estimated here.
While this study focused on the impact of changing patterns in smoking behaviour on cancer deaths in the future, it is also important to acknowledge that this is only one factor of many which are likely to contribute to the decrease in mortality rates for these cancer types. It is likely that changes in cancer screening and cancer management, and improvements in treatment are all playing a role in the estimated declines in mortality we have reported.39 Moreover, as the results from this study revealed that the proportion of cancer deaths directly attributable to smoking appears to have declined over time, interventions for other risk factors are also important, as is improving and implementing cancer screening and developing effective treatments, so that cancer mortality not attributable to smoking can also be reduced. As a substantial number of cancer deaths occur among former smokers, ongoing investment in the feasibility of targeted lung cancer screening will also be critical for at-risk former smokers.
As with all modelled projections, this study has some limitations, which should be considered when interpreting the results. The main limitation is that the projections are dependent on the assumptions made. The models did not include possible changes in other factors that can contribute to cancer mortality, including other risk factors, and cancer screening or treatment patterns.3 In practice, these effects could plateau as they either decrease or impact only a small proportion of cases, respectively, or in the case of new treatment availability, further reduce cancer mortality. Also, the projection models did not capture the impact of the recent COVID-19 pandemic, which led to disruptions in healthcare provision that may contribute to future excess deaths even for those who did not contract COVID-19.40 41 Estimating these impacts will be the subject of future work. Another limitation of this study is that the SAFs were based on adjusted relative risks from the CPS II, which may not be representative of the Australian population. However, results from a previous study suggest that the relative risk for all-cause mortality for current smokers from the large Australian 45 and Up Study is similar to those for cohorts in the USA.19 Despite these limitations, the study also has many strengths. Most notable are: the use of long-term high-quality observed data with population coverage10; the model design accounted for detailed data on cigarette tar consumption and the degree of association between cancer risk and smoking and the validation of the projections using observed data (online supplemental figure S3). The validated methods presented in this study can be applied to other countries to provide better estimates of cancer mortality related to smoking.
This is the first study to provide longer term national-level projections for the mortality rates for all smoking-related cancers taking into account detailed historical smoking intensity data. These projections for smoking-related cancers can serve as benchmarks against which to measure the impact of future cancer control initiatives, and these projections could also help inform health service planning to meet the future requirements for cancer care and treatment. Recognising that there are other, additional causes of mortality attributable to smoking, our research highlights the ongoing and future impact of smoking on the cancer burden, even in a country with major declines in smoking prevalence. Continued efforts in tobacco control remain an urgent public health priority.
Data availability statement
Data are available upon reasonable request. The tabulated data on cancer mortality are available from the Australian Institute of Health and Welfare at https://www.aihw.gov.au/. Access restrictions apply to the National Drug Strategy Household Surveys data on smoking behaviour. Approved release of these data can be obtained through an application to the Australian Institute of Health and Welfare.
Ethics statements
Patient consent for publication
Ethics approval
This population-based study used tabulated data on cancer mortality and smoking intensity released by the Australian Institute of Health and Welfare. Ethics approval was not required to use these aggregated data.
Acknowledgments
We would like to acknowledge the Australian Institute of Health and Welfare who provided the data from the National Drug Strategy Household Surveys (NDSHS), and the Australian Data Archive for providing access to the NDSHS data. However, they hold no responsibility for the analyses presented within this publication or the interpretation of them. We would like to thank Clare Kahn for editorial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KC: conceived the study. QL: designed the study, conducted the statistical analysis, interpretation and visualisation of results and drafted the manuscript. KC, JS, MW, XQY, MC, DO’C: contributed to the methods, JS and SY: contributed to the statistical analysis. EB and PG contributed to the interpretation of results and provided advice on policy aspects. All authors contributed to the interpretation of results and critically reviewed and revised the manuscript. KC and QL are guarantors of this study. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KC is co-principal investigator of an investigator-initiated trial of cervical screening, Compass, run by the Australian Centre for Prevention of Cervical Cancer (ACPCC), which is a government-funded not-for-profit charity; the ACPCC has received equipment and a funding contribution from Roche Molecular Diagnostics, and operational support from the Australian Government. KC is also co-principal investigator on a major investigator-initiated implementation programme Elimination of Cervical Cancer in the Western Pacific (ECCWP) which will receive support from the Minderoo Foundation, the Frazer Family Foundation, and equipment donations from Cepheid. Neither KC nor her institution on her behalf receives direct funding from industry for any project. MC is an investigator on an investigator-initiated trial of cytology and primary human papillomavirus screening in Australia (Compass; ACTRN12613001207707 and NCT02328872), which is conducted and funded by the Australian Centre for the Prevention of Cervical Cancer, a government-funded health promotion charity. The Australian Centre for the Prevention of Cervical Cancer has received equipment and a funding contribution for the Compass trial from Roche Molecular Systems and operational support from the Australian Government. However, neither MC nor his institution on his behalf (the Daffodil Centre, a joint venture between Cancer Council NSW and The University of Sydney) receive direct funding from industry for Compass Australia or any other project. All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.