Article Text

Abstract
Objective This 12-month study in a primary healthcare network aimed to assess the effectiveness of usual smoking cessation advice compared with personalised information about the spirometry results.
Design Randomised, parallel, controlled, multicentre clinical trial.
Setting This study involved 12 primary healthcare centres (Tarragona, Spain).
Participants Active smokers aged 35–70 years, without known respiratory disease. Each participant received brief smoking cessation advice along with a spirometry assessment. Participants with normal results were randomised to the intervention group (IG), including detailed spirometry information at baseline and 6-month follow-up or control group (CG), which was simply informed that their spirometry values were within normal parameters.
Main outcome Prolonged abstinence (12 months) validated by expired-CO testing.
Results Spirometry was normal in 571 patients in 571 patients (45.9% male), 286 allocated to IG and 285 to CG. Baseline characteristics were comparable between the groups. Mean age was 49.8 (SD ±7.78) years and mean cumulative smoking exposure was 29.2 (±18.7) pack-years. Prolonged abstinence was 5.6% (16/286) in the IG, compared with 2.1% (6/285) in the CG (p=0.03); the cumulative abstinence curve was favourable in the IG (HR 1.98; 95% CI 1.29 to 3.04).
Conclusions In active smokers without known respiratory disease, brief advice plus detailed spirometry information doubled prolonged abstinence rates, compared with brief advice alone, in 12-month follow-up, suggesting a more effective intervention to achieve smoking cessation in primary healthcare.
Trial registration number NCT01194596.
- smoking
- public health
- epidemiology
Data availability statement
Data are available on reasonable request. Patient level data, the full dataset and statistical code are available from the corresponding author (fmartin.tgn.ics@gencat.cat).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Smoking is a risk factor for major preventable diseases worldwide; therefore, smoking cessation is key to their prevention.1 Although most developed countries have reduced tobacco consumption in recent decades,2 smoking continues to be an epidemic worldwide and contributes to premature morbidity, disability and mortality.3
Nicotine dependence is composed of behavioural, cognitive and physiological phenomena, characterised by difficulty to quit smoking. A large proportion of smokers (70%–80%) express a desire to quit, but the process tends to be long and complex, and most patients find it very difficult to quit on their own. Successful stop-smoking interventions begins with identifying the patient’s willingness to quit and assisting, by using behavioural or pharmacological treatment, to help patient quit (5A’s strategy: Ask, Advise, Assess, Assist and Arrange).4
Several pharmacological and non-pharmacological methods are available to help smokers quit, and there is good-quality evidence on the effectiveness of many of them.5 However, pharmacological treatments are not always covered by the health system, and some patients cannot afford the associated costs. On the other hand, non-pharmacological methods have the advantage of being low-cost and feasible to implement, and may be particularly appropriate for primary healthcare patients.6 In this context, the role of healthcare professionals in promoting smoking cessation is essential, and is maximised when discussion of smoking habits and approaches to smoking cessation is routinely integrated into clinical practice.7 Despite highly variable rates of actual provision of these services, the net effect on reducing rates of smoking consumption can be substantial from a public health perspective.8 9
A recent systematic review found that motivational intervention may increase smoking cessation rates.10 An alternative approach could be to provide individually tailored information about the effects of tobacco, such as biomedical tests.11 Among them, spirometry appears to have a positive influence on smoking cessation,12 especially when an air-flow alteration can be demonstrated to the smoker.13 However, the available scientific evidence on the usefulness of spirometry as an intervention to tackle tobacco consumption is limited14 15; further studies are needed.
In this context, we hypothesised that detailed information about interpreting normal spirometry results is an effective motivational tool to encourage smoking cessation. Provide information on evidence of smoking-related health risks or harms could offer a ‘teachable moment’ that may facilitate a positive behaviour change. It has been documented that concerns about health status could be a circumstance which can lead patients to make an attempt to quit smoking.16 Thus, the aim of the trial was to compare the effectiveness of the usual counselling recommended in the primary healthcare setting to a combination of that health advice and personalised information on spirometry results. If the effectiveness of this approach is confirmed, spirometry would be an easy, low-cost intervention to implement and could have considerable implications for the prevention of diseases associated with tobacco.
Methods
Study design and patient involvement
A randomised, parallel, controlled multicentre clinical trial was carried out in twelve public primary healthcare centres in Tarragona (Spain). Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research. The study protocol has been published somewhere else 17
Participants
Men and women who visited the primary healthcare centres for any medical reason between June 2008 and June 2010 were invited to participate if they met the inclusion criteria: aged 35–70 years, active smoker and cumulative consumption >10 packs-year and provided informed consent. Participants did not receive any type of compensation for participating in the study. Exclusion criteria were any evidence of previous diagnosis of a respiratory disease (eg, chronic obstructive pulmonary disease (COPD), chronic bronchitis, emphysema, bronchiectasis or asthma) or functional pulmonary testing conducted within the previous 12 months, chronic or terminal condition that would affect the baseline parameters or complicate follow-up, or unwilling or unable to attend follow-up visits.
All eligible participants completed a comprehensive baseline assessment, including affiliations and sociodemographic data, comorbidity history and basic clinical evaluation, health habits and several measures of smoking habit (age onset, current daily consumption (cigarettes/day) and accumulated consumption (packs-year), nicotine dependence level, motivation to quit smoking and stage of the change process according to Prochaska and DiClemente’s model) and previous quit attempts and therapeutics resources used (online supplemental material table S1).
Supplemental material
Procedures and random allocation
Both the primary healthcare physician and the nurses of the participating centres were invited to collaborate in the study as associate researchers. Those who accepted received specific training, which was accredited by the Catalan Institute of Health, followed the principles of Good Clinical Practice, and signed a document in which they agreed to follow the study protocol.
At the recruitment visit, all potential subjects were advised that smokers are susceptible to COPD and spirometry is a simple, non-invasive test that allows diagnosis. Then, they were informed about the study and offered the opportunity to participate. Those who accepted signed the informed consent.
For all selected participants, pulmonary function (forced vital capacity (FVC), forced expiratory volume in the first second (FEV1) and FEV1/FVC ratio) was evaluated with spirometry and bronchodilation using the Datospir-600 spirometer (SIBELMED, Barcelona-Spain), which selects the best measure from three valid attempts and compares the result to the Spanish Society of Pulmonology and Thoracic Surgery-based norms, adjusted for age, sex, height, weight and ethnicity. Pulmonary function was considered normal if spirometry results met the following criteria: FVC ≥80% of the theoretical reference value, FEV1 ≥80% of the theoretical reference value, and FEV1/FVC ratio ≥0.7.18 Also, the ‘lung age’ (mean age of a non-smoker with the participant’s spirometry values) was determined.
Participants with normal spirometry results were randomly assigned to the intervention group (IG=286) or control group (CG=285). Randomisation was based on a (1:1) computerised sequence prepared by the research team’s statistician (figure 1).
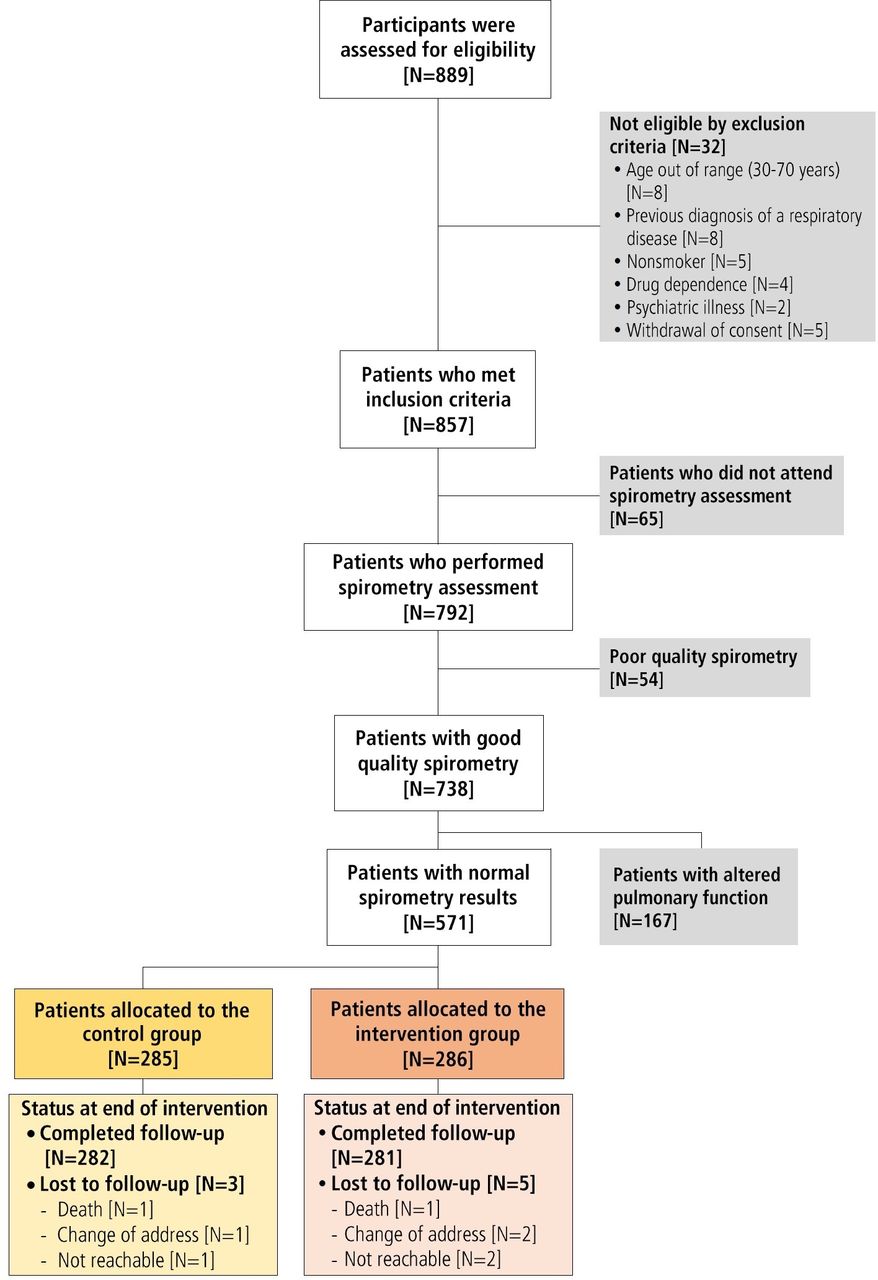
Screening, randomisation and follow-up of the participants (CONSORT diagram). CONSORT, Consolidated Standards of Reporting Trials.
As the intervention was based on behavioural change, this was not a blinded clinical trial. The IG participants received a detailed, structured explanation on the spirometry results obtained and their interpretation, summarised as ‘lung age’. The CG participants received usual care and were simply informed that the spirometry results were within normal parameters (table 1).
Smoking cessation counselling
All participants received brief counselling about smoking cessation as recommended by current guidelines: firm, concise, individual advice (trying to find the most important motivation for each patient), appropriate to the individual’s stage of the change process.4 They were also offered a specific ‘quit smoking’ medical visit applying other approaches, such as a motivational intervention or pharmacological treatment. Abstinence status was assessed at 6 months and 12 months. Smoking cessation advice was repeated at each follow-up visit.
Participants showing altered pulmonary function were excluded from randomisation for ethical reasons. In addition, those with altered pulmonary function usually require combined strategies to quit smoking, which would make it difficult to assess the independent effect of spirometry.19 20 So, they were informed of the spirometry results and referred to their primary healthcare physician to assess the findings in the clinical setting, and these participants were followed-up during the study period (reported as online supplemental material).
Outcomes assessment
Primary outcome was self-reported prolonged abstinence (12 months) from smoking, confirmed by expired-carbon monoxide (CO) determined at each follow-up visit (at 30 days, at 6 and 12 months). On the other hand, self-report and/or expired-CO levels>10 ppm were considered as active tobacco consumption.21 Point-prevalence tobacco abstinence and self-reported smoking reduction at the end of follow-up were considered a secondary outcome measures.
Statistical analysis
The sample obtained from 571 participants allows to detect >8% difference between the IG and CG in abstinence (absolute risk), a 10% in the CG,15 maintained a power of 80% (beta risk) and a significance level (alpha risk) of 5%, in a two-tailed contrast, and assuming a patient loss to follow-up of 10%.
Data were drawn from a centralised database and grouped so that those responsible for analysis were blinded to study group assignments. Effect calculations were based on intention-to-treat analysis and a ‘worst-case’ strategy was used: all patients originally randomly assigned were included, regardless of whether they actually satisfied the treatment received, and subsequent withdrawal or deviation from the protocol, in both groups, it was assumed that the expected response (smoking cessation) did not occur in patients lost to follow-up, so they were considered as smokers.22
Descriptive analysis includes frequencies and percentages for categorical variables and means and SD for continuous variables. χ2 or Fisher’s exact test (categorical variables) and Student’s t test (continuous variables) were used for bivariate analyses baseline characteristics according to the groups. Prolonged abstinence and point-prevalence abstinence at 6 months and 12 months postintervention rated were calculated. Covariates that predicted abstinence with significant p value and those considered clinically or epidemiologically relevant (eg, age, sex, educational level, number of previous quit attempts, nicotine dependence, motivation to quit smoking, comorbidity) were considered to be included in a multivariate logistic regression analysis, and in a Cox analysis of survival (abstinence).23 The selection of a subset of covariates, which were included in the final models, was based on the purposeful selection method.24 Results are presented as a risk measure, OR and HR.
All measures were expressed with their respective CI of 95%. Two-sided p values of 0.05 or less were considered to indicate statistical significance. Analyses and data handling were performed using IBM SPSS Statistics package version 19.0.
Results
Participants included
In total, 889 smokers were preselected. Good-quality spirometry was obtained in 738 participants. Pulmonary function tests were normal in 571 participants (77.4% (95% CI 74.2% to 80.2%)), 286 were allocated in the IG and 285 in the CG; 563 (98.6%) completed the follow-up (figure 1). Mean age was 49.8 (SD ±7.78) years, 45.9% male and mean cumulative smoking exposure was 29.2 (±18.7) pack-years. There were no significant differences between the groups with respect the characteristics of the participants at baseline (table 2).
Characteristics of the participants at baseline, according to randomised assignment group
Follow-Up and outcomes
Table 3 shows the number of participants who attempted to quit smoking and the methods used according to the groups, during the follow-up study period. Significantly more participants in the IG attempted to quit smoking and accepted professional assistance, compared with the CG. However, there were no significant differences with respect to the methods used to quit smoking between the groups.
Participants who attempted to quit smoking and the methods used according to randomised assignment group during the follow-up
In total, 15.9% (91/571) of the clinical trial participants quit smoking at 12-month follow-up; however, point-abstinence rates were different between the groups (19.9% (95% CI 15.7% to 24.9%) in the IG vs 11.9% (95% CI 8.7% to 16.2%) in the CG; p=0.008). Prolonged abstinence, validated by expired-CO, were higher in the IG compared with the CG, both at 6 months (13.3% (38/286) vs 7.7% (22/285); p=0.04) and at 12 months (5.6% (16/286) vs 2.1% (6/285); p=0.03). Table 4 shows the abstinence rates observed during follow-up, according to randomised assignment group, and multivariate logistic regression analysis. In the multivariate logistic regression analysis, abstinence rates were always favourable in the IG, compared with the CG, both point-abstinence (multivariable-adjusted OR 1.79 (95% CI 1.06 to 3.03; p=0.031)) and prolonged abstinence (multivariable-adjusted OR 2.71 (95% CI 1.04 to 7.29; p=0.044)) at 12-month follow-up.
Abstinence rates observed, unadjusted, age-adjusted and sex-adjusted and multivariable-adjusted ORs according to randomised assignment group (intention-to-treat analysis)
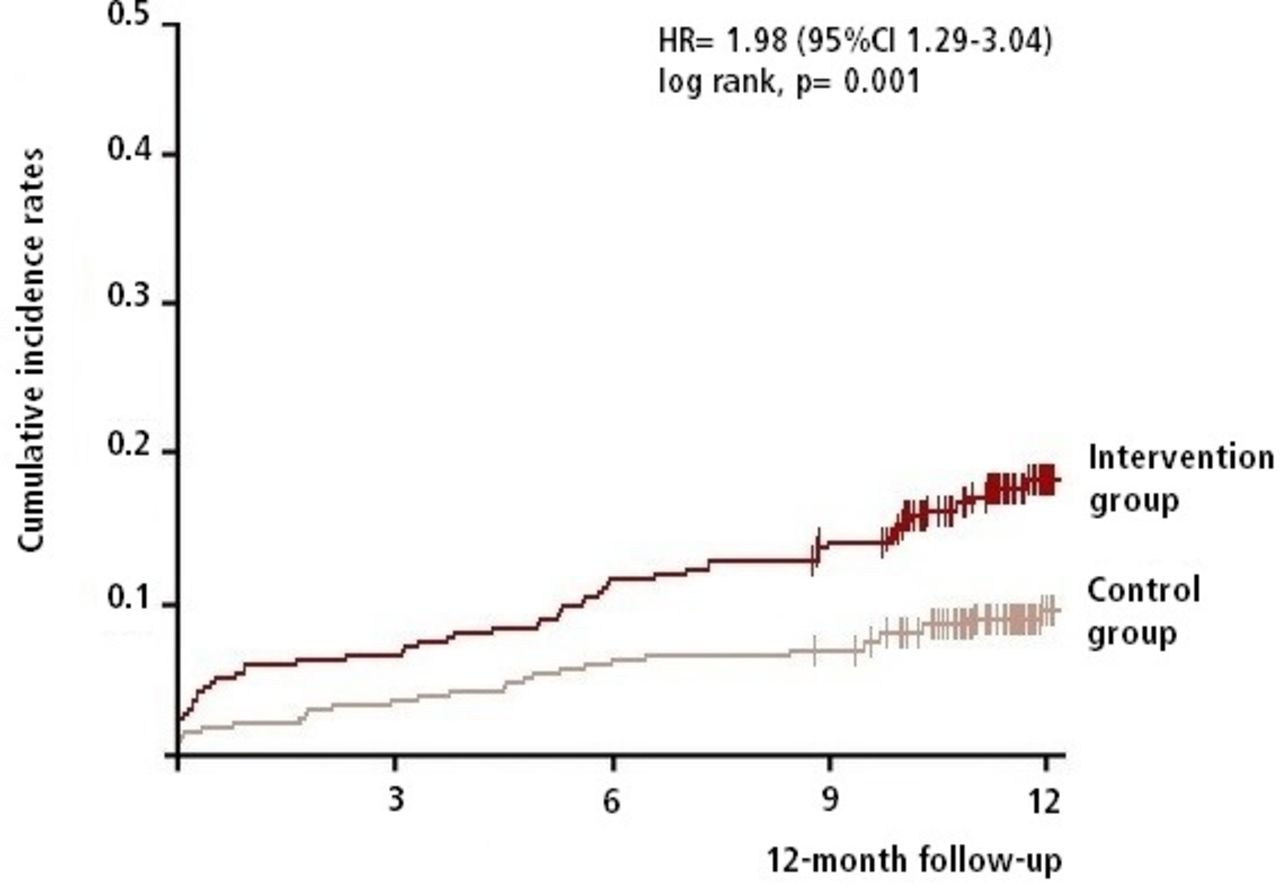
Comparison of the cumulative abstinence curves favoured the IG with an overall HR of 1.98 (95% CI 1.29 to 3.04) (figure 2). Results of bivariate analysis using the log-rank test are reported in a online supplemental material, showing the efficacy of the intervention on abstinence at 12 months follow-up according to some individual and clinical conditions (online supplemental material table S2).

{kind=link}
{kind=link}
Cumulative incidence rates of tobacco abandonment at 12-month follow-up in the intervention group and control group (analysis from Cox regression models).
Table 5 shows results Cox regression analysis assessing multivariable-adjusted risks factors to abstinence at 12-month follow-up. In multivariate analysis, abstinence was independently associated with the spirometry intervention (HR 1.96 (95% CI 1.12 to 2.76)). Other variables considered were significant: the use of pharmacological treatment to quit smoking and/or intensive-motivational intervention, personal motivation and the individual’s stage in the change process (preparation and action), cumulative tobacco consumption and baseline expired-CO values.
Cox regression analyses assessing multivariable-adjusted risks factors to abstinence at 12 months follow-up
Smokers
At 12 months follow-up, 480 participants continued smoking, self-reported reduction in daily-consumption was 2.9 cigarettes/day (SD 0.35), and there were no significant differences between the groups (3.2 (SD 6.5) in the IG, and 2.7 (SD 8.3) in the CG; p=0.530).
Altered pulmonary function
Altered pulmonary function were observed in 167 participants (22.6% (95% CI 19.8% to 25.8%)), and they were excluded from randomisation. The baseline characteristics and abstinence rates at 12-month follow-up are shown as online supplemental material tables S3 and S4.
Discussion
Summary of main findings
The evidence about the effect of spirometry as a motivational strategy to quit smoking is limited and controversial.15 Our findings in this pragmatic clinical trial confirmed that patients who received brief advice plus detailed spirometry information doubled prolonged abstinence rates, compared with brief advice alone, in 12-month follow-up (HR 1.98 (95% CI 1.29 to 3.04)). Success was also more likely in participants at advanced stage of the change process (preparation or action), and in those who accepted an intensive-motivational intervention and/or use smoking cessation pharmacotherapy. This was an expected result because the most effective method to quit smoking combines behavioural and pharmacological treatments.4 5
Comparison with existing literature
Our main interest in this study was to influence smoking habits through explaining the results of pulmonary function testing by spirometry as a motivational strategy. This has been the focus of periodic Cochrane reviews but, so far, the results are inconsistent.25 In a recent systematic review that examined the effects of spirometry on smoking cessation, only one study (of five total) indicated efficacy of spirometry feedback and linked lung age to increased smoking quit rates.15
Spirometry is one of the main pulmonary function tests. There is a high availability of spirometers in primary healthcare, and their use has increased in this setting.26 It is a simple, non-invasive diagnostic procedure that provides information about pulmonary function and could be useful to increase motivation to quit smoking. If pulmonary function is normal, probably, there is a motivation to quit smoking before there is a lung damage. If pulmonary function is no-normal then, probably, this is a message that the lungs are undergoing accelerated deterioration that would be slowed if the smoker stopped.15 However, the best results are observed in patients with chronic airflow obstruction, in which various smoking cessation strategies are used together.19 20 This makes it difficult to specify the independent effect of spirometry.
Only a few studies have evaluated the isolated effect of spirometry as an aid to quit smoking, and they provide contradictory data.27 An Italian study in primary healthcare by Segnan et al found no significant differences between applying a brief individual intervention and an intensive intervention with spirometry on smoking cessation (RR 1.19 (95% CI 0.62 to 2.30)).28 Other study in Belgium, Buffels et al observed a favourable but no significant effect of the intervention with spirometry on smoking cessation (RR 1.17 (95% CI 0.66 to 2.06)).29 A study conducted under conditions similar to ours, by Irizar-Aramburu et al, found no favourable effect of spirometry on prolonged smoking abstinence (RR 0.79 (95% CI 0.42 to 1.48)).30 Most studies have had a small sample, with insufficient statistical power to detect significant effects. Other interventions based on biomedical risk assessment, such as expired-CO levels, do not seem to be useful. A pooled analysis of four trials using expired-CO measurement together with spirometry observed no significant benefit on the rate of smoking cessation (RR 1.27 (95% CI 0.83 to 1.21)).15 Only Parkes et al report a significant beneficial effect of spirometry (including ‘lung age’ information) on the abstinence rate (13.6% vs 6.4%, RR 2.12 (95% CI 1.24 to 3.62)).12 This could be explained by the smoker’s ability to more easily see a causal link between smoking and direct damage (eg, older lung age), while indirect measures of exposure to tobacco (eg, expired CO), might not be enough to motivate behavioural change.15
Some methodological characteristics could also explain contradictory study results. Only a few studies provide a definition of being a smoker, such as nicotine addiction levels according to the Fagerström score or stages of change according to Prochaska and Di Clemente.25 It has been established that the different basic motivational stages of the participants could be responsible for the differences observed between the studies. In a few studies, motivation to quit smoking was so high that any comparison with the usual brief advice would have little opportunity to make a significant difference and the incremental effect of the biomedical risk assessment could have been attenuated. Therefore, there is scope to improve the methodological quality of studies that evaluate the effectiveness of biomedical risk assessment as an aid to quit smoking.15
Major strengths and limitations of this study
The present trial is a pragmatic study carried out in the usual working conditions of primary healthcare centres, with a complete follow-up by the patient’s own primary healthcare providers and collection of a wide range of information. Therefore, our results should reflect the actual effectiveness of the intervention tested. It included an adequate sample of adult smokers in several stages of the change process related to smoking cessation. Prior to the intervention, patients had a complete clinical evaluation, as recommended by the clinical guidelines (as detailed in online supplemental material). The study sample was recruited during the medical visits in twelve primary healthcare centres (eight urban and four rural) managed by the Catalan Health Institute, serving a representative adult population (195 343 patients, aged >18 years).17 Furthermore, few participants were lost to follow-up after 12 months, both in IG and CG (five and three, respectively). This could be relevant, since it is rarely seen in clinical trials (such rates often exceed 20%) and could have potential implications for estimates of the effect of interventions.31 The explanation for this high follow-up rate could be that data were collected by the healthcare providers of the participants. In Spain, attendance at primary healthcare providers is high (>5 times patient-year),32 and this could facilitate the follow-up of study patients. Therefore, our results should reflect the actual effectiveness of the intervention assessed in the Spanish primary healthcare population.
All staff members were standardised and received specific training before the implementation of the intervention, to guarantee that the advices, attitudes and behaviours were applied according to the study protocol. Our intervention followed the 5A’s strategy for smoking cessation plus spirometry information. The 5A’s framework has been widely recommended for the delivery of brief advice in primary healthcare visits. After giving clear, strong and personalised messages to quit smoking (advise), it was recommended to identify the patient’s willingness to quit (assess) and provide assistance by recommending or prescribing behavioural or pharmacological treatment (assist and arrange).4 These additionally methods were recorded, there were no significant differences between the groups, and our adjusted analyses included the numbers of participants who accepted the assistance. Therefore, we emphasise that this intervention reflects the pragmatic aspect of this study, since it is not a pure randomised controlled trial, as these normally prevent participants from receiving additional treatments. We assumed that our proposed intervention was less intense, compared with other interventions, such as motivational intervention and/or use of pharmacological treatment, and it has been demonstrated a direct dose-response association between intensity, success of the intervention and abstinence rates.33 Although a more intensive approach may be more successful, at the same time, we believe that this could lead us away from a basic strategy for daily practice that the study tries to reflect.34
Our study also has limitations. The population was enrolled from patients who had a medical visit for any reason. Illness may increase motivation to quit smoking and the patient may be more likely to respond when advised.35 Population bias might have led to overestimation of the true effect size of health counselling to quit smoking. Therefore, we only included smokers without known lung disease. An age limit of at least 35 years could have been a limitation, but it is generally accepted that pathologies of pulmonary function associated with smoking are not expected in younger patients.36 Self-report of tobacco abstinence was confirmed by expired-CO measurement; although this is not the best indicator of smoking cessation, it is currently considered an easy, non-invasive, objective test to evaluate smoking behaviour.37 38 Therefore, an overestimation of smoking cessation could occur, but in view of the observed abstinence rates, it is unlikely to have great impact on the results. In any case, we assumed that overestimations were evenly distributed because the groups had comparable characteristics.
We assume these inherent limitations but note that our study provides age-adjusted and sex-adjusted and multivariate-adjusted data that evaluate the probable causes and risks of abstinence, compared with other studies that report unadjusted data. It is important to note that estimates can vary considerably depending on the type of analysis and adjustments performed; therefore, we emphasise again the importance of maximising adjustments. And although we did multivariate adjustment analyses, as in all clinical studies, a residual confounder cannot be excluded due to unmeasured factors (eg, healthcare-related or lifestyle factors, potential contamination within the trial sites).
Implications for clinical practice and future research
Our results indicate that spirometry interventions can improve smoking cessation outcomes in primary healthcare settings. Given the contradictory results in previous studies, we believe that ESPITAP study makes a relevant contribution to the evidence: in active smokers without spirometry-confirmed respiratory disease, brief advice plus detailed spirometry results doubled prolonged abstinence rates at 12 months, compared with only the recommended brief advice. This suggests a role for normal-spirometry information as an effective tool to achieve smoking cessation in primary healthcare.
Pharmacological treatments have been shown to be more effective in quitting smoking, and there is evidence that smokers are much more likely to attempt to quit smoking if tobacco treatment is a full coverage by healthcare system or health insurance companies.33 39 However, many of them have a high economic cost or they are not full coverage by the healthcare system. Therefore, we believe that, despite the reported effectiveness of medical advice is lower, an intervention that is within the usual practice of primary healthcare, plus personalised information on spirometry results, would have a large-scale impact on general population.
The general practice is an appropriate environment for counselling to quit smoking. General practitioners should be encouraged to assume their significant role in quit smoking interventions as part of global tobacco control activities.8 Therefore, spirometry assessment could be important to patients who seek medical help to quit smoking. Future trials are needed to investigate the efficacy and cost-effectiveness in actual practice. In this context, our research group intends to continue evaluating the usefulness of spirometry as part of healthcare interventions tackling tobacco use.40
What is already known on this subject
Throughout the world tobacco smoking is the leading cause of preventable death and illness.
There are several methods (pharmacological and non-pharmacological) to help smokers quit.
There are few studies that have evaluated the effect of biomedical risk assessment with spirometry as an aid to smoking cessation, and they provided contradictory data.
What this study adds
Brief advice plus detailed spirometry information, compared with brief advice alone, suggesting a more effective intervention to achieve smoking cessation in primary healthcare.
Data availability statement
Data are available on reasonable request. Patient level data, the full dataset and statistical code are available from the corresponding author (fmartin.tgn.ics@gencat.cat).
Ethics statements
Ethics approval
The trial was approved by the regional Ethics Committee for Clinical Research (IDIAP Jordi Gol. Barcelona, Spain), and conducted in accordance with the principles of the Declaration of Helsinki, ICH Guidelines for Good Clinical Practice, and requirements of Spain’s Data Protection legislation and registered with the 4R07/040 identifier.
Acknowledgments
The study will be funded by a grant from the Institut Universitari d’Investigació en Atenció Primària-IDIAP Jordi Gol, and will be possible thanks to the generous collaboration of doctors and nurses from the Tarragona-Reus Primary Care Area (Catalan Health Institute) which constitute the participants of the ESPITAP Study Group.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators ESPITAP Study Group Investigators: Aguirre-Alava G, Altamiras-Badia M, Alvarez-Soler E, Anguera-Perpiña C, Arnau-Adan V, Baiges-Folch M, Basora-Gallisa J, Berenguer-Atrio P, Bibiloni-Sole A, Blade-Creixenti J, Blanch-Aubia J, Boada-Tous A, Borras-Gavalda A, Borras- Vicente D, Cabre-Vila JJ, Camos-Guijosa P, Canalejo-Escudero JJ, Cando-Guasch G, Castellar- Salinas MJ, Castro-Pamies R, Comino-Sillero L, Dalmau-Vidal S, DeAndres-DePablo MJ, DelPozo-Nubio J, Diego-Ferrer A, Duran-Visiedo JM, Elviro-Bodoy T, Ferrater-Cubells J, Ferre-Gras J, Fustero-Fustero I, Garcia-Aguila R, Garcia-Gonzalo C, Garcia-Masso A, Gens- Barbera M, Gil-Mancha S, Gil-Sanchez MD, Giner-Aguilo C, Giro-Guasch JM, Girona-Real R, Gomez-Santidrian F, Grau-Perez C, Grive-Isern M, Guinjoan-Aymemi N, Hernandez-Anguera JM, Hernandez-Lazaro E, Hernandez-Vidal N, Isach-Subirana A, Jovani-Puig MD, Juncosa- Cabre M, Lara-Pedrosa A, Lara-Pedrosa MT, Ledo-Garcia J, Lluis-Burgeño M, Lorente-Zozaya A, Mangrane-Ferrando M, Mangrane-Guillen C, Marimon-Barba J, Marti-Suau E, Martín- Lorente A, Martin-Vergara N, Martinez-Blesa MT, Martinez-Perez T, Mas-Escoda R, Medina- Clemente M, Mengual-Miralles M, Mora-Guilabert N, Moreno-Lagunas A, Ortega-Vila Y, Oya-Girona E, Palacios-Llamazares L, Palma-Jimenez MI, Pardo-Andujar J, Pascual-Palacios I, Pelleja-Pellicer ML, Perez-Bauer M, Perez-Galvez E, Pineda-Rigau T, Piñol-Moreso JL, Poca- Pastor A, Prats-Caellas A, Profitos-Amiell R, Reche-Martinez A, Revuelta-Garrido V, Rey- Reñones C, Ribes-Arganuy M, Riera-Sole A, Rius-Fernandez B, Rubio-Gascon C, Sabate- Mestre J, Sagarra-Alamo R, Sanchez-Oro I, Sardaña-Alvarez E, Sarra-Manetas N, Sarre-Torra Y, Silva-Orjuela AR, Soler-Barreras P, Solis-Narvaez R, Subirats-Sanz E, Subirats-Segarra R, Tersa-Alcobe M, Timon-Torres M, Urbaneja-Diez A, Vazquez-Martinez O, Vers-Lopez O, Vila-Molet M, Vila-Rodrigo RV, Vizcaino-Marin J.
Contributors FM-L, JB-G and RS form the nucleus of the team of researchers in the ESPITAP study. FM-L is the principal investigator and developed the original idea for the project. The study design was further developed by FM-L, JB-G and NM-V. The following have intervened in the planning of the intervention and statistical methods that is evaluated: FM-L, JB-G, FV, NM-V, IP-P, EA-L, AS-A, R-EC, CR-R and RS. All authors have read and corrected draft versions and approved the final manuscript.
Funding The study was funded by departmental resources from the University Institute for Research in Primary Care – IDIAP Jordi Gol (Barcelona, Spain).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.