Article Text

Abstract
Background The relationship between educational attainment and ischaemic heart disease (IHD) is limited in evidence in middle-income countries like China. Exploring lifestyle-related mediators, which might be not universal between socioeconomic status and health outcomes in diverse regions, can contribute to interventions targeted at the Chinese to narrow the educational gap in IHD.
Methods Based on the China Kadoorie Biobank of 489 594 participants aged 30–79 years who did not have heart disease or stroke at baseline, this study examined the association of educational attainment with IHD. Total IHD cases were further divided into acute myocardial infarction (AMI) cases and non-AMI cases. The Cox proportional hazard model was performed to estimate the HRs and 95% CIs for mortality and incidence of IHD. Logistic regression was used to estimate the ORs and 95% CIs for case fatality.
Results During the median follow-up period of 11.1 years, this study documented 45 946 (6668) incident IHD (AMI) cases and 5948 (3689) deaths altogether. Lower educational attainment was associated with increased risk of incident AMI as well as death and fatality of total IHD including its subtypes (ptrend <0.001). Although the risk of incident non-AMI was greater for participants with higher levels of education in the whole population (ptrend <0.001), an inverse association of education with its incidence was found in participants from <50 years age group and rural areas. Smoking and dietary habits were the two most potent mediating factors in the associations of education with mortality and AMI incidence; whereas, physical activity was the major mediating factor for non-AMI incidence in the whole population.
Discussion Interventions targeting unhealthy lifestyles are ideal ways to narrow the educational gap in IHD while solving ‘upstream’ causes of health behaviours might be the most fundamental ones.
- education
- ischaemic heart disease
- lifestyle
- cohort studies
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
It has been reported by WHO that cardiovascular diseases (CVDs) are the leading cause of death globally, and an estimated 17.9 million people died from CVDs in 2016, representing 31% of all global deaths.1 At the national level, ischaemic heart disease (IHD) and stroke were the major causes of death and disability-adjusted life-year lost in China in 2017.2
Social determinants of health, as ‘cause of causes’ of diseases, are acquiring extensive attention. With education being a vital index of socioeconomic circumstances,3 the relationship between educational attainment and cardiovascular outcomes has been widely studied.4–8 A negative educational gradient is established for IHD mortality.5 6 Though the educational pattern of acute myocardial infarction (AMI) incidence showed a consistent inverse association in high-income countries, only a few studies have been done in middle-income countries and they displayed controversial results.7
The association of educational attainment with IHD is limited in evidence among the Chinese. Existing studies in China include a case–control study,9 with limitations of selection bias and only surviving cases investigated, and the cohort studies either confined to the retired employees of a company or only considering the composite of cardiovascular outcomes.6 10 Furthermore, the level of education was classified into only two categories due to the limited sample size.9 10 There were no in-depth investigations into the potential reasons for educational disparities in IHD in most studies. Given IHD’s established lifestyle risk factors and implications of educational attainment for a health conscious lifestyle,11 12 it might be an appropriate health outcome to explore the pathway through which education works in the human body in China.
Based on a large prospective cohort in Chinese adults, the present study aimed to investigate the educational disparities in the long-term risk of mortality, incidence and case fatality of IHD. We further examined whether such educational disparities were consistent across other sociodemographic characteristics. The extent to which lifestyle risk factors contributed to the educational disparities in IHD was also explored.
Methods
Study design
The design and procedures of China Kadoorie Biobank have been reported previously.13 Briefly, 512 725 residents aged 30–79 years from 10 geographically diverse regions, five urban and five rural, were invited to participate in the baseline survey between 2004 and 2008, and subsequent follow-up. At baseline, trained staff administered laptop-based questionnaires as well as took anthropometric measurements. All participants provided written informed consent.
Participants who had heart disease (n=15 472) or stroke (n=8884) at baseline, or had missing values for body mass index (BMI; n=2) were excluded from this study. A total of 489 594 participants were included in the final analysis.
Assessment of educational attainment and covariates
In the baseline survey, the trained staff asked participants to provide their highest educational attainment by selecting from: (1) not formally educated (<6 years), (2) primary school (6 years), (3) middle school (9 years), (4) high school (12 years), (5) college (15 years), (6) university or above (≥16 years). In the analysis, options of (5 and 6) were combined into category ‘college or above’.
Other covariates at baseline were also collected by questionnaires, including demographic and socioeconomic status (household income, educational attainment, and occupation), lifestyle behaviours (tobacco smoking, alcohol drinking, dietary habits, physical activities and so on), personal medical history and family history of diseases. Details of the lifestyle assessments have been published previously.14 Participants who reported any of the parents or siblings having heart disease or stroke were defined as having a family history of CVDs.
Anthropometric measurements were performed to measure the standing height, weight, waist circumference (WC) and blood pressure (BP). BMI was derived as weight (kg) divided by height (m) squared.
Ascertainment of outcome
Long-term follow-up was initiated after the completion of the baseline survey. We established electronic linkages for each participant to the local Chinese Disease Surveillance Points system, the local disease registry system and the national health insurance claim databases in which >97% of participants were covered using the unique national ID. The death or disease information was updated for the participants periodically. Active confirmation of vital status was also being done annually by reviewing residential records or visiting local communities in case some participants had moved permanently out of the study areas. All events were coded in the International Classification of Diseases, 10th Revision (ICD-10) by trained staff blinded to baseline information.
In this study, the endpoints of interests are the incidence of IHD (ICD-10: I20-I25), AMI (ICD-10: I21) and other IHD but AMI (hereinafter referred to as ‘non-AMI’) and mortality of the three outcomes listed above as underlying causes of death. Case fatality was defined as all-cause death within 28 days of onset of IHD.
Statistical analysis
For baseline characteristics, means were calculated for continuous variables and percentages for categorical variables using linear or logistic regression, with adjustment for 5-year age groups, sex and study regions where appropriate. The mortality and incidence rate of each educational category were yielded by negative binomial regression, while the case fatality rate by logistic regression, with the same adjustment listed above.
Person-years were calculated from the date of completion of the baseline survey to the date of confirmed endpoint event, death from other causes, lost to follow-up, or 31 December 2017, whichever came first. We used the Cox proportional hazard model to estimate the HR and 95% CIs for mortality and incidence of IHD and its subtypes adjusting for sex and CVDs family history. The proportional hazard assumption was examined by log-log survival plot for our Cox models and found to be satisfied for all endpoints. The model was stratified by ten study regions and 5-year age groups using age as the time scale. The participants who attended college or above were considered as the reference group. Logistic regression was used to estimate the OR and 95% CIs for case fatality among those who had incident IHD with adjustment for age groups, sex, study regions and CVDs family history.
We performed the stratified analysis to determine whether the association between educational attainment (primary school or lower vs middle school or higher) and IHD differed between sex (male or female), age groups (<50, 50–59 or ≥60 years) and regions (rural or urban). We used the likelihood ratio test to compare nested models, with or without the interaction term.
By additionally adjusting for lifestyle risk factors (tobacco smoking, alcohol drinking, dietary habits, physical activity, BMI, and WC) in the Cox model, we explored their mediating effect on the associations of educational attainment with specific endpoints in the total and sex-specific population.15 In detail, we added lifestyle risk factors to the basic model and examined the per cent change in the logHRs of educational attainment, respectively. The proportion of the association that was explained by a lifestyle risk factor was calculated as follows:  %. When dietary habits were included in the model, we adjusted for the frequency (by assigning the midpoint of each category and including the variable as continuous) of eating fresh vegetables, fresh fruits and red meat simultaneously.
%. When dietary habits were included in the model, we adjusted for the frequency (by assigning the midpoint of each category and including the variable as continuous) of eating fresh vegetables, fresh fruits and red meat simultaneously.
Statistical significance was set at p value (two sided) <0.05. All analyses were conducted by Stata (V.15.0; StataCorp).
Patient and public involvement
This study was performed without patient involvement. Patients were not invited to comment on the study design, not consulted to develop patient-relevant outcomes or to interpret the results. The results will be disseminated to the public through appropriate media channels.
Results
Baseline characteristics
The mean age of all participants included in the analysis was 51.6±10.6 years, women accounted for 59.1% of the total population, and 43.2% were from urban areas. The baseline characteristics of five educational groups are presented in table 1. Well-educated participants tend to be younger, men, living in urban areas, work as managers or professionals and have higher household income. Also, participants with higher educational attainment tended to have a healthier lifestyle than those lower educated, except for physical activity in both men and women and body weight and shape in men.
Baseline characteristics of 489 594 participants by educational attainment
Educational attainment and IHD
During the total follow-up period of 5.3 million person-years (median: 11.1 years; IQR: 1.9 years), there were 45 946 (6668) incident IHD (AMI) cases and 5948 (3689) deaths altogether. The unadjusted mortality and incidence rate of IHD was 1.12 and 8.94 per 1000 person-years, respectively, and the unadjusted case fatality was 10.5%. Figure 1 demonstrates the corresponding values by educational attainment with adjustment for age groups, sex, and study areas. With the decline of educational attainment, both mortality and case fatality of IHD showed an upward trend; by contrast, the incidence of IHD is highest among the participants with a ‘college or above’ degree. Concerning AMI, the unadjusted mortality and incidence rate was 0.69 and 1.26 per 1000 person-years, respectively; and case fatality was 54.7%. All three indices increased steadily with the decline of educational attainment (figure 1).

Mortality, incidence and 28-day case fatality rate for ischaemic heart disease by educational attainment. Case fatality was defined as death within 28 days of onset of IHD. All the rates were based on the model with adjustment for 5-year age groups, sex and study regions. The error bars stand for 95% CIs of the values.
Compared with the participants getting a ‘college or above’ degree, the ones with lower educational levels were associated with an increased risk of death due to IHD (ptrend <0.001), and the adjusted HR (95% CIs) for participants with no formal education was 2.25 (1.92 to 2.63). Lower education was also associated with higher AMI and non-AMI mortality, AMI incidence and case fatality of IHD in total and both AMI and non-AMI (ptrend <0.001) (figure 2).
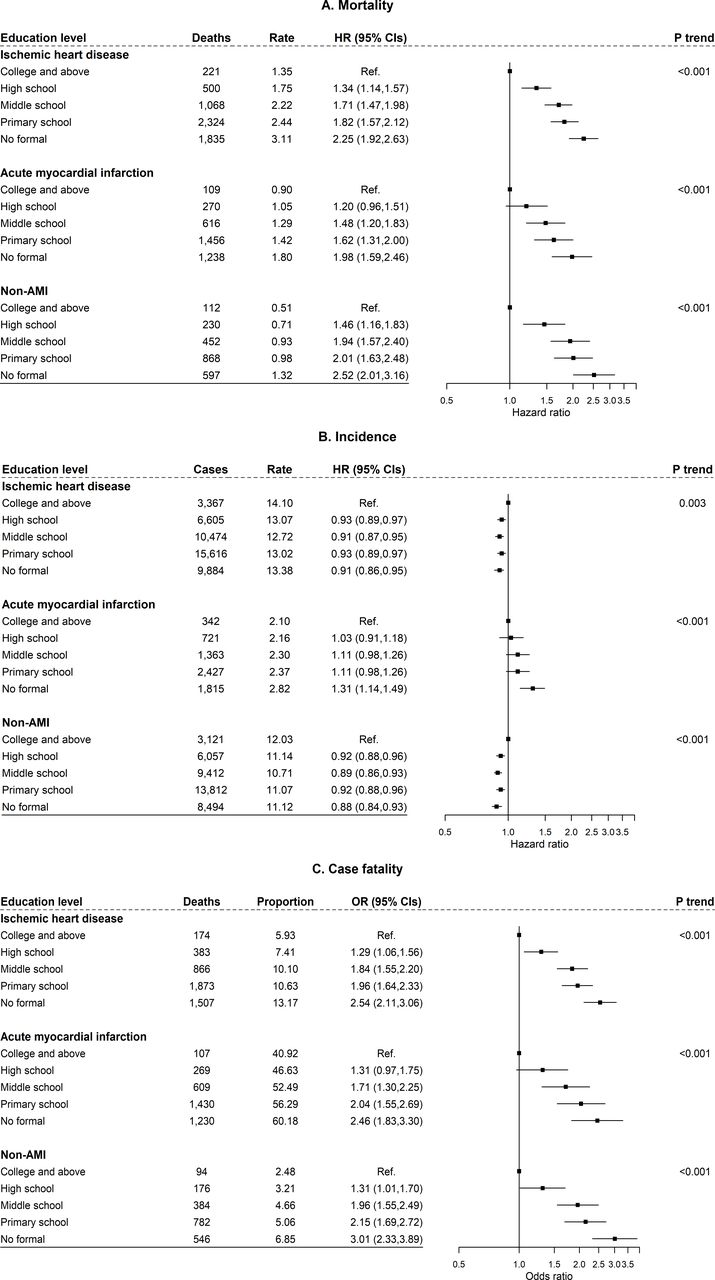
Association of educational attainment with mortality, incidence and case fatality for ischaemic heart disease. Cox models were stratified by 5- year age groups at baseline and study regions with adjustment for sex and CVDs family history. Logistic models were adjusted for age groups, sex, study regions and CVDs family history. All the rates were based on the same models as in figure 1. Rates were per 1000 person-years; proportions were per 100 patients. AMI, acute myocardial infarction; CVDs, cardiovascular diseases.
Contrary to the above findings, lower educational attainment was associated with a marginally decreased risk of incident IHD (ptrend=0.003). Using the best-educated participants as the reference group, the adjusted HR (95% CIs) for those receiving no formal education was 0.91 (0.86 to 0.95). Education and non-AMI also exhibited a positive association (figure 2B).
Subgroup analysis
There was a statistically significant difference in the associations of educational attainment with all AMI and non-AMI endpoints between sex (all pint <0.001), except for the incidence of non-AMI (pint=0.250). Compared with participants with middle school or higher education, those with primary school or lower education had a higher effect size in women than in men (figure 3).

Association of educational attainment with mortality, incidence and case fatality for ischaemic heart disease by subgroups. Cox models were stratified by 5- year age groups at baseline and study regions with adjustment for sex and CVDs family history. Logistic models were adjusted for age groups, sex, study regions and CVDs family history. The figure shows the HRs/ORs of participants with primary school or lower education compared with those with middle school or higher education. AMI, acute myocardial infarction; CVDs, cardiovascular diseases.
The associations between education and risk of two IHD subtypes were almost consistent in all age groups, except for the incidence and case fatality of non-AMI (figure 3). In detail, in the <50 years age group, the participants with lower education had a greater risk of incidence of or fatality from non-AMI, while such a case was not found in the older age groups.
There was a significant rural-urban difference in the incidence of non-AMI (pint <0.001). In the rural areas, participants with lower education had a higher hazard of developing non-AMI (HR 1.09; 95% CIs 1.05 to 1.14); but in the urban areas, lower education was associated with a lower risk of non-AMI (0.91; 0.88 to 0.94). Besides, the hazard of education was greater for urban residents concerning case fatality (figure 3).
Role of lifestyle risk factors on education and IHD
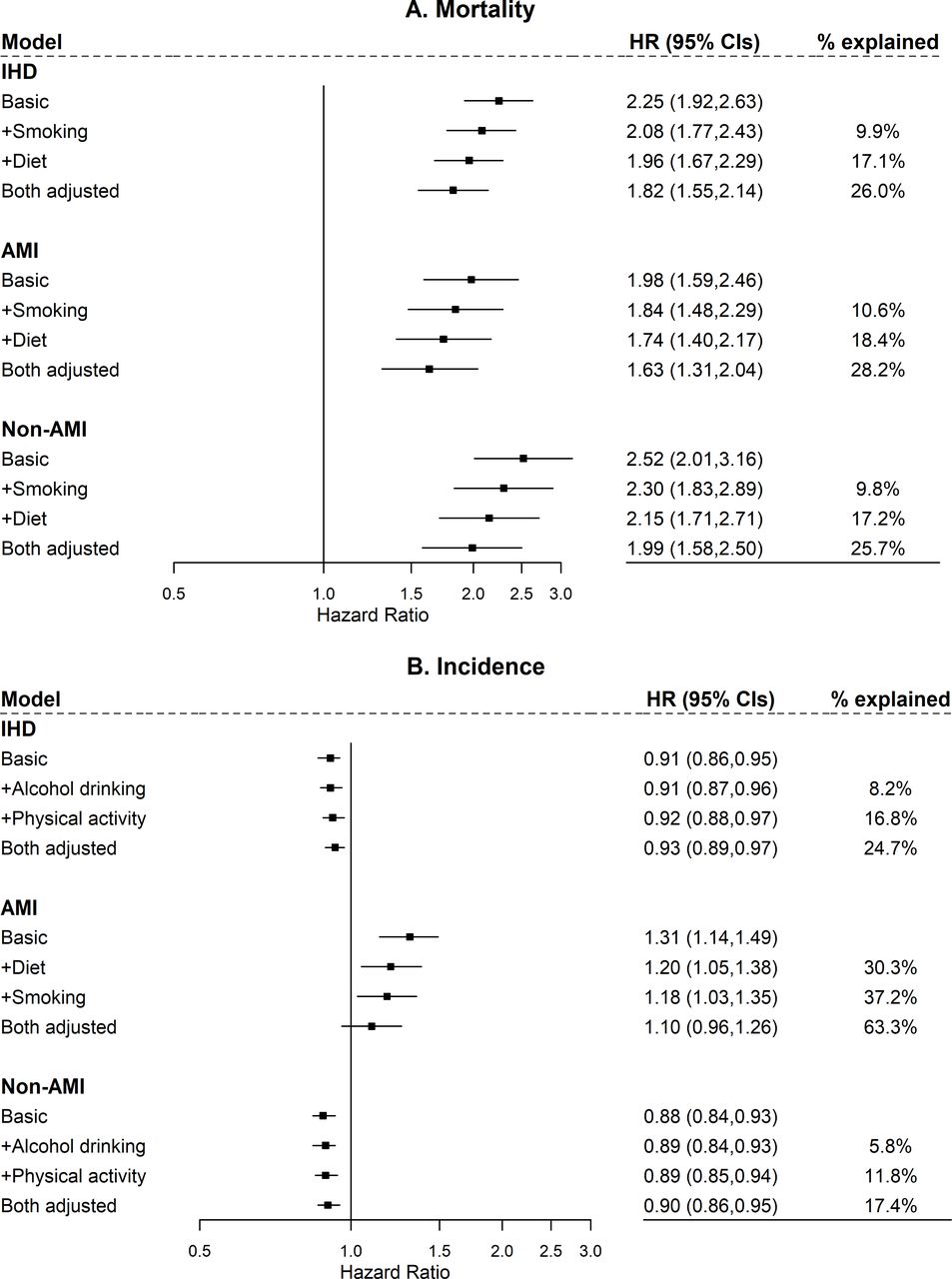
We estimated the extent to which lifestyle risk factors explained the association between education and IHD. Both smoking and dietary habits were two of the most important mediators of the associations between education and mortality endpoints in the total and sex-specific population(figure 4; online supplemental file 1). Smoking and dietary habits explained 9.9% and 17.1% of the inverse association of education with total IHD, respectively; they together accounted for 26.0% of the association (figure 4). Other lifestyle risk factors appeared to demonstrate a subtle mediating effect on the association (eg, HR +Alcohol drinking=2.26; 95% CIs 1.93 to 2.64; other data not shown).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association of educational attainment with IHD with additional adjustment for lifestyle risk factors. The basic model was stratified by 5-year age groups at baseline and study regions with adjustment for sex and CVDs family history. The adjusted model included variables in the basic model plus the listed lifestyle risk factor, including smoking (never, former, current 1–14 cig/day, 15–24 cig/day or ≥25 cig/day; smokers who had stopped due to illness were counted with smokers), alcohol drinking (less than weekly, ex-regular, weekly but less than daily, daily <15 g/day, 15–29 g/day, 30–59 g/day ≥60 g/day of pure alcohol), dietary habits (frequency of eating fresh vegetables, fresh fruits and red meat), physical activity (MET-hour/day), BMI (kg/m2) and WC (cm). The final model adjusted the two most influential lifestyle risk factors listed above. The figure shows the HRs of participants with no formal school compared with those with college or above education. AMI, acute myocardial infarction; BMI, body mass index; CVDs, cardiovascular diseases; IHD, ischaemic heart disease; MET, metabolic equivalent of task; WC, waist circumference.
Regarding the incidence endpoints, both smoking and dietary habits were also the most influential mediators for AMI in the whole population; they could explain 63.3% of the association altogether (figure 4). In contrast, for non-AMI, alcohol drinking and physical activity were the two most potent explanatory variables in the whole population (figure 4). For men, none of the associations of education with the incidence endpoints in the basic models were statistically significant. For women, both smoking and dietary habits could explain 33.6% of the association for AMI; while the mediating effect of lifestyle risk factors was negligible for non-AMI (online supplemental file 1).
Discussion
In this nationwide community-based cohort of Chinese, we presented educational disparities in total IHD and its subtypes. As the level of education decreased, the risk of death and fatality of total IHD and its subtypes as well as the potential for the onset of AMI increased. Although the risk of incident non-AMI was greater for participants with higher levels of education in the whole population, our subgroup analysis showed an expected inverse association of education with its incidence in participants from <50 years age group and rural areas. Smoking was the most potent mediating factor in the associations of education with mortality and AMI incidence; whereas, physical activity was the major mediating factor for non-AMI incidence in the whole population.
The inverse gradient of educational attainment in endpoints related to death or AMI incidence in our study was concordant with previous findings in western countries.4 7 16 Two studies of Chinese people showed that the risk of AMI in participants with the education of <9 years was greater than that with the education of ≥9 years.9 10 Compared with low-educated participants, the adjusted HR for incident AMI in those highly educated was 0.89 (95% CI 0.80 to 0.98).10 An explanation is that people with higher educational levels were likely to have higher access to healthcare services and better performance in disease prevention and management.6 17–20
In the present study, participants with ‘college or above’ education were associated with higher incidence of non-AMI (including less severe subtypes), which accounted for most of the total IHD cases. A similar finding of the education-IHD incidence association was also seen in the Puerto Rico Heart Health Programme among urban men, with a poorer status of healthy lifestyles and clinical indices in higher-educated participants.21 However, in our study, higher-educated participants showed better performance in some lifestyle factors than the lower-educated. Another explanation might be inadequate utilisation of healthcare services and underdiagnosed IHD in low-educated participants. Further subgroup analysis indicated the positive association was only seen in older and urban population; in the <50 years age group and rural areas, participants with lower levels of education still exhibited a greater risk of non-AMI.
In a study comprising 49 cohorts of middle-aged European adults in 2015, the researchers broke down inequalities in IHD mortality into IHD incidence and 28-day case fatality. They observed that inequalities in IHD mortality were mainly a reflection of the corresponding incidence in the Nordic countries, Scotland and Lithuania and driven by 28-day case fatality in the remaining central/South Europe.22 In our study, the educational disparity in IHD mortality might be mainly attributed to the gap in case fatality; while in <50 years participants, the AMI mortality differences between each level of education seemed likely to be ascribed to AMI incidence discrepancies.
Our subgroup analysis suggests that there was a significantly greater excess risk associated with lower educational attainment in women compared with men. The result was consistent with a meta-analysis, including over 22 million individuals of various ancestries, which highlights the significance of education on women.23 Instead, worse lifestyles or health indicators in male participants due to different social roles and greater pressures might offset the benefits brought by higher educational levels.
The previous studies in western countries investigated that modifiable lifestyle factors, including smoking,24–27 physical activity,27 dietary habits,26 alcohol drinking26 and BMI,24 25 27 could explain a relatively significant proportion of the educational gradient of coronary heart disease (CHD) incidence. However, the contribution of each explanatory factor varied among studies. For example, the Women’s Lifestyle and Health Cohort Study in Sweden showed the HR of incident CHD comparing the lowest education group to the highest was attenuated by 34% with further adjustment for exercise,28 while the effects of low physical activity were negligible both among women and men in seven Danish cohort studies.27 In our study, smoking and dietary habits were two of the most important mediators in the association of educational attainment with IHD mortality and AMI incidence. In contrast, for non-AMI incidence, educational attainment might work through different pathways. All the above suggest there might have no universal mediators between education and IHD between regions where the social context and distribution of lifestyle risk factors and health resources are various. Furthermore, in the present study, the large proportion of education-IHD association unexplained by lifestyle risk factors indicates there were other key characteristics such as poor awareness of the need for treatments and medical care utilisation mediating the process.29
This study provided the first comprehensive presentation of educational disparities in the incidence, mortality and case fatality of IHD and its subtypes, as well as conducted an in-depth analysis of the mediation effect of lifestyle risk factors on the educational disparities of IHD in the Chinese population. The 10 representative areas across China chosen could maximise regional (urban–rural) diversity. Owing to the massive amounts of participants and long-term follow-up, our study could explore the potential non-linear relationship between educational attainment and IHD across multiple educational categories. The prospective design, low rate of lost to follow-up, and rich information on sociodemographic and behavioural characteristics are also highlights of the study.
There still exist several limitations. First, a lack of related information on psychological stress and health service utilisation restricted all-round exploration of how educational level affected the onset and death of IHD. Second, self-reported information related to lifestyle behaviours in this study might bring information bias.
Conclusion
In such a large prospective cohort of Chinese adults, educational disparities did exist in IHD and were more prominent in IHD-attributable deaths. People with low education, an absolutely large part of the population in China, bear a greater burden of IHD. Diseases or deaths further increase social inequality through employment opportunities and illness-caused poverty. Lifestyle factors, especially smoking and dietary habits, are important explanatory factors in the education-IHD pathway. Interventions targeting unhealthy lifestyles are one of the ideal ways to narrow the educational gap in IHD. However, solving ‘upstream’ causes of health behaviours might be the most fundamental means.
What is already known on this subject
The educational pattern of ischaemic heart disease (IHD) has consistently shown an inverse association in high-income countries.
However, such an association is limited in evidence among middle-income countries like China.
What this study adds
This prospective cohort study of general Chinese population demonstrated a significantly inverse association of educational attainment with the risk of death and fatality of total IHD and its subtypes and the onset of AMI.
Although the risk of incident non-AMI was greater for participants with a higher level of education in the whole population, our subgroup analysis showed an expected inverse association in participants from <50 years age group and rural areas.
Smoking and dietary habits were the two most potent mediating factors in the associations of education with mortality and AMI incidence; whereas, physical activity was the major mediating factors for non-AMI incidence.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Ethical Review Committee of the Chinese Center for Disease Control and Prevention (Beijing, China: 005/2004) and the Oxford Tropical Research Ethics Committee, University of Oxford (UK: 025–04).
Acknowledgments
The most important acknowledgement is to the participants in the study and the members of the survey teams in each of the 10 regional centres, as well as to the project development and management teams based at Beijing, Oxford and the 10 regional centres.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators International Steering Committee: Junshi Chen, Zhengming Chen (PI), Robert Clarke, Rory Collins, Yu Guo, Liming Li (PI), Jun Lv, Richard Peto, Robin Walters. International Co-ordinating CenterCentre, Oxford: Daniel Avery, Ruth Boxall, Derrick Bennett, Yumei Chang, Yiping Chen, Zhengming Chen, Robert Clarke, Huaidong Du, Simon Gilbert, Alex Hacker, Mike Hill, Michael Holmes, Andri Iona, Christiana Kartsonaki, Rene Kerosi, Ling Kong, Om Kurmi, Garry Lancaster, Sarah Lewington, Kuang Lin, John McDonnell, Iona Millwood, Qunhua Nie, Jayakrishnan Radhakrishnan, Paul Ryder, Sam Sansome, Dan Schmidt, Paul Sherliker, Rajani Sohoni, Becky Stevens, Iain Turnbull, Robin Walters, Jenny Wang, Lin Wang, Neil Wright, Ling Yang, Xiaoming Yang. National Co-ordinating CenterCentre, Beijing: Zheng Bian, Yu Guo, Xiao Han, Can Hou, Jun Lv, Pei Pei, Chao Liu, Canqing Yu. 10 Regional Co-ordinating CentersCentres: Qingdao CDC: Zengchang Pang, Ruqin Gao, Shanpeng Li, Shaojie Wang, Yongmei Liu, Ranran Du, Yajing Zang, Liang Cheng, Xiaocao Tian, Hua Zhang, Yaoming Zhai, Feng Ning, Xiaohui Sun, Feifei Li. Licang CDC: Silu Lv, Junzheng Wang, Wei Hou. Heilongjiang Provincial CDC: Mingyuan Zeng, Ge Jiang, Xue Zhou. Nangang CDC: Liqiu Yang, Hui He, Bo Yu, Yanjie Li, Qinai Xu,Quan Kang, Ziyan Guo. Hainan Provincial CDC: Dan Wang, Ximin Hu, Jinyan Chen, Yan Fu, Zhenwang Fu, Xiaohuan Wang. Meilan CDC: Min Weng, Zhendong Guo, Shukuan Wu,Yilei Li, Huimei Li, Zhifang Fu. Jiangsu Provincial CDC: Ming Wu, Yonglin Zhou, Jinyi Zhou, Ran Tao, Jie Yang, Jian Su. Suzhou CDC: Fang liu, Jun Zhang, Yihe Hu, Yan Lu, Liangcai Ma, Aiyu Tang, Shuo Zhang, Jianrong Jin, Jingchao Liu. Guangxi Provincial CDC: Zhenzhu Tang, Naying Chen, Ying Huang. Liuzhou CDC: Mingqiang Li, Jinhuai Meng, Rong Pan, Qilian Jiang, Jian Lan,Yun Liu, Liuping Wei, Liyuan Zhou, Ningyu Chen Ping Wang, Fanwen Meng, Yulu Qin, Sisi Wang. Sichuan Provincial CDC: Xianping Wu, Ningmei Zhang, Xiaofang Chen,Weiwei Zhou. Pengzhou CDC: Guojin Luo, Jianguo Li, Xiaofang Chen, Xunfu Zhong, Jiaqiu Liu, Qiang Sun. Gansu Provincial CDC: Pengfei Ge, Xiaolan Ren, Caixia Dong. Maiji CDC: Hui Zhang, Enke Mao, Xiaoping Wang, Tao Wang, Xi zhang. Henan Provincial CDC: Ding Zhang, Gang Zhou, Shixian Feng, Liang Chang, Lei Fan. Huixian CDC: Yulian Gao, Tianyou He, Huarong Sun, Pan He, Chen Hu, Xukui Zhang, Huifang Wu, Pan He. Zhejiang Provincial CDC: Min Yu, Ruying Hu, Hao Wang. Tongxiang CDC: Yijian Qian, Chunmei Wang, Kaixu Xie, Lingli Chen, Yidan Zhang, Dongxia Pan, Qijun Gu. Hunan Provincial CDC: Yuelong Huang, Biyun Chen, Li Yin, Huilin Liu, Zhongxi Fu, Qiaohua Xu. Liuyang CDC: Xin Xu, Hao Zhang, Huajun Long, Xianzhi Li, Libo Zhang, Zhe Qiu.
Contributors JL conceived and designed the paper. LL, ZC and JC, as members of the CKB steering committee, designed and supervised the conduct of the whole study, obtained funding, and together with CY, YG, PP, LY, YC, HD and XW acquired the data. LC and YT analysed the data and drafted the manuscript. JL contributed to the interpretation of the results and critical revision of the manuscript for important intellectual content. All authors contributed to and approved the final manuscript. JL is the study guarantor.
Funding This work was supported by National Natural Science Foundation of China (81941018). The CKB baseline survey and the first re-survey were supported by a grant from the Kadoorie Charitable Foundation in Hong Kong. The long-term follow-up is supported by grants (2016YFC0900500, 2016YFC0900501, 2016YFC0900504) from the National Key R&D Programme of China, National Natural Science Foundation of China (81390540, 81390541, 81390544) and Chinese Ministry of Science and Technology (2011BAI09B01).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.