Article Text

Abstract
Background High-sensitivity C reactive protein (hsCRP) has been proposed as a marker of incident cardiovascular disease and vascular mortality, and may also be a marker of non-vascular mortality. However, most evidence comes from either North American or European cohorts. The present proposal aims to investigate the association of hsCRP with the risk of all-cause mortality in a multiethnic Brazilian population.
Methods Baseline data (2008–2010) of a cohort of 14 238 subjects participating in the Brazilian Longitudinal Study of Adult Health were used. hsCRP was assayed with immunochemistry. The association of baseline covariates with all-cause mortality was calculated by Cox regression for univariate model and adjusted for different confounders after a mean follow-up of 8.0±1.1 years. The final model was adjusted for age, sex, self-rated race/ethnicity, schooling, health behaviours and prevalent chronic disease.
Results The risk of death increased steadily by quartiles of hsCRP, from 1.45 (95% CI 1.05 to 2.01) in quartile 2 to 1.95 (95% CI 1.42 to 2.69) in quartile 4, compared with quartile 1. Furthermore, the persistence of a significant graded association after the exclusion of deaths in the first year of follow-up suggests that these results are unlikely to be due to reverse causality. Finally, the HR was unaffected by the exclusion of participants who had self-reported medical history of diabetes, cancer and chronic obstructive pulmonary disease.
Conclusions Our study shows that hsCRP level is associated with mortality in a highly admixed population, independent of a large set of lifestyle and clinical variables.
- epidemiology
- mortality
- cohort studies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
C reactive protein (CRP), which is synthesised by the liver, is a biomarker of the innate immune response. Its main function is as defence against bacteria and clearance of damaged cells. Circulating CRP is not proinflammatory in healthy subjects, but undergoes conformational changes when tissue is damaged, activating complement and immune response. It is regulated by proinflammatory cytokines including interleukin (IL)-6, IL-1 and tumour necrosis factor-α.1 2 CRP has been shown to be a useful marker for presence of infection and of severity of trauma, but more recently the development of methodologies has allowed for the detection of high-sensitivity C reactive protein (hsCRP), which is associated with chronic non-communicable diseases (NCD), in which there is an activation of the proinflammatory state. These include type 2 diabetes, obesity, metabolic syndrome and atherosclerosis.3 4
Previous studies have shown that hsCRP level is independently associated with incident cardiovascular disease (CVD). In observational epidemiological studies, elevated plasma hsCRP levels are consistently associated with increased risk of ischaemic heart disease and ischaemic cerebrovascular disease. Studies carried out among individuals with no history of CVD demonstrate that hsCRP is a strong predictor of future vascular events, and in most cases has proven independent of the major ‘traditional’ risk factors (sex, age, smoking, cholesterol level, blood pressure and diabetes).5–7 However, most evidence comes from either North American or European cohorts. A very recent study demonstrates that higher hsCRP significantly increased the risk of developing CVD in a Chinese population.8
Monitoring and maintaining ideal hsCRP levels can be an important therapeutic target and can be used as criteria for primary and secondary prevention.9–12 Low-grade systemic inflammation can be defined by hsCRP level, and decreased inflammation may reduce atherothrombotic risk. hsCRP values of 1–3 mg/L are considered a marker of moderate cardiovascular risk and levels of >3 mg/L may indicate higher cardiovascular risk.13
The relation of hsCRP with all-cause mortality was also evaluated in The Emerging Risk Factors Collaboration (2010), which shows that the risk ratio (RR) for vascular mortality per threefold higher loge CRP concentration was 1.71 (1.53–1.91) when initially adjusted for age and sex only, and 1.55 (1.37–1.76) when adjusted further for conventional risk factors. RRs for non-vascular mortality were 1.55 (1.41–1.69) and 1.54 (1.40–1.68), respectively, for each adjustment.7 The recent Whitehall II study suggests that IL-6 and hsCRP are more important predictors of mortality than alpha-1-acid glycoprotein for cardiovascular, cancer and all-causes-related mortality.14
The causal role of the different inflammatory biomarkers in the incidence of NCD is difficult to determine because inflammatory responses may be due to a multiplicity of factors, such as tobacco consumption, overweight and obesity, physical inactivity, persistent and/or transient infection, ethnicity, and socioeconomic condition,5 15–17 all associated with mortality.
The present proposal aims to investigate the association of hsCRP with the risk of all-cause mortality in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) cohort. This analysis may help extend previous observations to a unique multiethnic and highly admixed population.
Methods
Population
The ELSA-Brasil is a large, multicentre, prospective cohort study designed primarily to identify the risk factors and the natural history of diabetes and CVD in the country. A total of 15 105 participants, who are government employees from universities and research institutions located in six different states, took part. All active or retired employees of these institutions, aged between 35 and 74 years, were eligible for the study. Exclusion criteria included current or recent (<4 months prior to the first interview) pregnancy, intention to quit working at the institution in the near future, severe cognitive or communication impairment, and, if retired, residence outside the metropolitan area of a study centre. All participants answered a comprehensive questionnaire including questions about their general health conditions, family health issues, medication use, smoking, alcohol consumption, physical activity and mental health. In addition, they underwent a series of clinical and laboratory tests. Baseline examination was performed between 2008 and 2010. Repeated interviews and examinations are conducted every 3–4 years thereafter. The details of the study methodology, including design, eligibility criteria and the cohort’s profile, have been previously described.18 Of the 15 105 participants of the ELSA-Brasil baseline study, 683 outliers were excluded due to hsCRP levels greater than 10 mg/L, and 184 were removed due to missing information for self-rated race. A total of 14 238 individuals remained in our data set.
Biomarkers as measure of exposure
All biochemical analyses were assayed from fasting serum samples collected between 07:30 and 10:30 in 2008–2010. hsCRP was assayed with immunochemistry (nephelometry) using BN II (Siemens). For analytical purposes, the levels were equally split into four groups (quartiles).
All-cause mortality as measure of outcome
All-cause mortality data up to December 2017 were collected from annual telephone monitoring and confirmed by death certificate.18
Covariates
Demographics
Demographic information included age, sex, schooling (defined by incomplete elementary: <8 years; complete elementary: 8–11 years; complete high school: 11–14 years; and university degree: ≥15 years) and self-rated race/ethnicity (defined by white, black, ‘brown’ or of mixed colour, native indigenous, and Asian ethnicity).
Health behaviour
Health behaviours included self-reported alcohol consumption (categorised as excessive: men ≥210 g alcohol/week, women ≥140 g alcohol; moderate: men <210 g alcohol/week, women <140 g alcohol; and none), smoking status (current, former and never smoker), physical activity level (low, moderate or high, based on the International Physical Activity Questionnaire), and fruits and vegetables consumption (a food frequency questionnaire was applied in order to evaluate participants’ usual consumption in the previous 12 months), and body mass index (BMI, kg/m²) was used as a continuous variable.
History of chronic disease
This included history of diabetes mellitus (DM), classified using blood glucose (fasting plasma glucose ≥126 mg/dL or ≥200 mg/dL, 2 hours after overload with 75 g anhydrous glucose) or glycated haemoglobin ≥6.5% threshold measurements defined by the American Diabetes Association, or by self-reported diagnosis or reported use of insulin or hypoglycaemic medication identified in the baseline survey of the ELSA study; systolic blood pressure (mm Hg) obtained as the mean of the last two out of three measurements taken 5 min apart, and used as a continuous variable; use of antihypertensive drugs; and CVD, defined based on report of coronary revascularisation or of a medical diagnosis of myocardial infarct and/or stroke and/or heart failure. Finally, we included self-reported diagnosis of cancer (CA), chronic obstructive pulmonary disease (COPD) and presence of depression over the previous 7 days, assessed through the adapted Brazilian Portuguese version of the Clinical Interview Schedule-Revised, which is a structured interview for measurement and diagnosis of non-psychotic psychiatric morbidity in community and primary care settings.
Statistical analysis
The demographic and clinical characteristics of participants are expressed as frequencies with proportions for categorical variables, and median with IQR or mean with SD for continuous variables. We examined participants’ characteristics by sex. The association of baseline covariates with all-cause mortality was calculated by Cox regression for univariate model. The association of baseline covariates with quartiles of hsCRP was calculated by analysis of variance for continuous variables and Pearson’s χ2 for categorical variables. Kaplan-Meier method was used to estimate the risk of fatal event, and differences in curves were tested by log-rank test. Finally, Cox regression analysis was used to explore the association between hsCRP and all-cause mortality, adjusted for different confounders. Results are expressed as HR and 95% CI. Testing the proportional hazard assumption suggested no violation of proportionality. The first model was adjusted for age, while the second model for age and sex. In the third model we adjusted for self-rated race/ethnicity and BMI, and in the fourth model we adjusted for schooling and health behaviours (alcohol consumption, smoking status, physical activity level, fruits and vegetables consumption). In the final model we included all covariates: systolic blood pressure, use of antihypertensive drugs and prevalent chronic disease (DM, depression, CVD, CA, COPD). The area under the curve (AUC) was used to estimate improvement in risk discrimination of hsCRP. Sensitivity analyses were also performed to exclude bias due to reverse causality (model 5 after exclusion of deaths in the first year) and bias due to self-reported medical history of DM, CA and COPD. The level of significance was set at p<0.05. Statistical analyses were performed using STATA V.15.1 and R V.3.5.3 statistical software packages.
Results
A total of 14 238 individuals were included in the final analysis, 444 (3.12%) of whom died over a mean follow-up of 8.0±1.1 years (death at a minimum of 16 days and maximum of 9.8 years).
The sociodemographic, behavioural, comorbidity and laboratory characteristics of participants stratified by sex are shown in table 1. The mean age was 52 years at baseline (range 34–75 years). There was a slight predominance of women (54.0%) and self-declared white ethnic origin (52.5%), and most participants had completed higher education (53.0%) and had never smoked (57.2%) (table 1).
Baseline characteristics of participants in the ELSA-Brasil cohort
Significant differences were observed in baseline characteristics in the population ranked by quartiles of hsCRP, as shown in table 2. Comorbidities such as DM, depression, CVD and COPD and health behaviours such as current smoking and low physical activity were progressively more common with increasing levels of hsCRP. Also, the proportion of women increased with increasing levels of hsCRP (table 2).
Baseline covariates by hsCRP quartiles
The Cox regression models revealed a consistent and independent association between hsCRP and death from all causes even after adjusting for all sets of confounders (model 5; table 3). The calculated AUC without hsCRP in the fully adjusted model (model 5) was 0.793 and with hsCRP was 0.797: net reclassification improvement analyses (NRI) (95% CI): 0.1013 (0.0063 to 0.1962) (p=0.036); and integrated discrimination improvement (IDI) (95% CI): 0.0026 (0.0006 to 0.0046) (p=0.010).
Association of hsCRP (quartiles) with all-cause mortality over a mean follow-up of 8.0±1.1 years
In the sensitivity analysis, we found no evidence on the influence of bias due to self-reported medical history of DM, CA and COPD. The HR for hsCRP in model 5 after exclusion of 3086 self-rated DM, CA and COPD, with 226 (2.5%) deaths, was 1.71 (95% CI 1.11 to 2.60), 1.57 (95% CI 1.01 to 2.43) and 2.20 (95% CI 1.42 to 3.39) for those in the second, third and highest quartiles, respectively. A total of 23 deaths (0.2%) were in the first year of follow-up. The HR for hsCRP in model 5 after exclusion of deaths in the first year was 1.40 (95% CI 1.01 to 1.95), 1.50 (95% CI 1.08 to 2.08) and 1.92 (95% CI 1.39 to 2.65) for those in the second, third and highest quartiles, respectively.
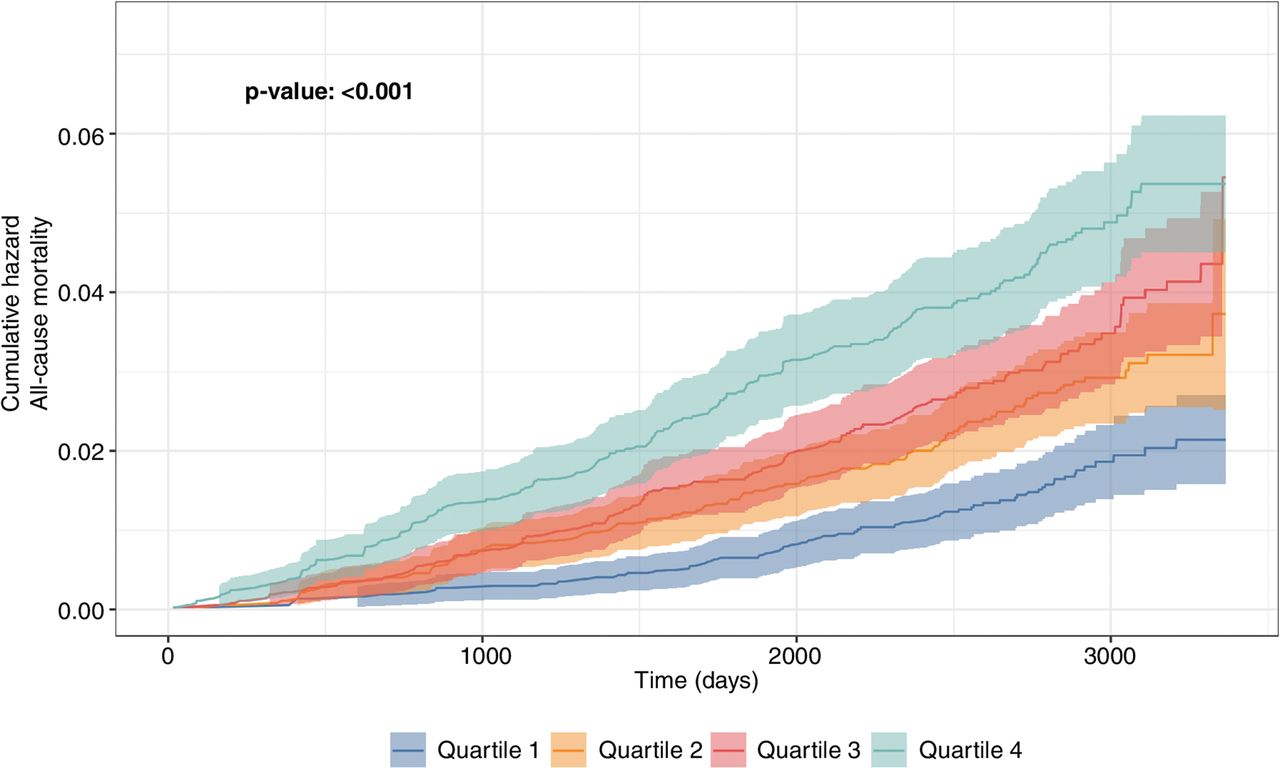
The Kaplan-Meier mortality curve demonstrates that there is an increase in mortality with increasing quartiles of hsCRP levels (see figure 1; p<0.001, log-rank test).

{kind=link}
Kaplan-Meier cumulative hazard for all-cause mortality according to high-sensitivity C-reactive protein (mg/dL) categories (quartiles).
Discussion
In this study, we investigated whether hsCRP predicts all-cause mortality in a prospective analysis of middle-aged Brazilian men and women. Our results show that the risk of all-cause mortality increases progressively with increasing levels of hsCRP. The results of our study not only confirm an association between hsCRP and all-cause mortality but also show that it is independent of possible confounders associated with either risk of inflammation or pre-existing chronic disease. Furthermore, the persistence of a significant graded association after the exclusion of deaths in the first year of follow-up suggests that these results are unlikely to be due to reverse causality. Finally, the HR was unaffected by the exclusion of participants who had self-reported medical history of DM, CA and COPD. Addition of hsCRP to the fully adjusted model resulted in an increase in the AUC from 0.793 to 0.797, and the NRI and IDI values indicate that the hsCRP is a significant predictor of risk. However, there is some debate about the use and reporting of these measures.19 20 Therefore, cautions are needed when interpreting these results.
Strengths and limitations
The strengths of this study include its large sample size with diverse demographic, regional and socioeconomic characteristics, inclusion of several potential confounders, long follow-up period, and highly standardised biochemical assessment of exposure and certified deaths. Our results are consistent with previous studies from different international cohorts showing that hsCRP, as well as other inflammatory markers, is associated with age, gender, ethnic background,17 21 BMI,15 smoking22 and chronic diseases.7 23–27
The present study has potential limitations too. Inflammatory markers may have a diurnal variation. In our study however blood samples were collected in a narrow time window (from 07:30 to 10:30); in a previous study, in a comparable British population study, we observed no significant effect of such variation on estimates of associations.28 While the level of hsCRP was assessed using a single measurement, this is consistent with most previous population studies of inflammatory biomarkers.14 21 24 ELSA-Brasil is conducted in six of Brazil’s state capitals and consisted of university and research institute employees with stable employment and a notably high educational achievement; thus, the prevalence and incidence rates found cannot be generalised to Brazil’s overall adult population. However, this fact does not undermine our findings regarding the association between hsCRP and mortality, as most scientific evidence on risk factors for mortality comes from occupational cohorts, such as the British Doctors, or highly community-based ones, such as the Framingham Heart Study.29 30 Finally, we assessed only all-cause mortality, so we are unable to report on associations with cause-specific deaths.
Possible mechanisms
Inflammatory processes play an important role in the development of NCDs. The innate and adaptive immune responses have a pivotal role in the initiation, progression and clinical consequences of atherosclerotic diseases.10 11 31 Components of the immune system are also altered in obesity and type 2 DM; these immunological changes and alterations in the levels of specific cytokines and chemokines suggest that inflammation participates in the pathogenesis of DM.26 Finally, previous studies have also found an association between hsCRP levels and risk of CA (lung, colorectal, skin and bladder), with progression and survival of patients with pancreatic, oesophageal, prostate and colorectal CA.27
CRP is a biomarker of the innate immune response, its main function being as defence against bacteria and clearance of damaged cells, and it is therefore unclear as to whether CRP is simply a marker of underlying systemic response to inflammation or is itself a directly contributing factor to such disorders. The concentration of hsCRP, a non-specific marker of acute-phase inflammatory response, is predictive of future cardiovascular morbidity.5–7 Genetic studies indicate that about 50% of the individual variance in baseline CRP concentration is genetic and largely attributable to non-coding polymorphisms in the CRP gene.1 3 7 11 The other major determinant, independent of genetic factors, is the level of adiposity, especially central abdominal obesity.15 25 32 33
CRP binds to low-density lipoprotein cholesterol, and it has been detected in atherosclerotic plaques, which raises the possibility that CRP may play a direct causal role.34 35 Moreover, the recent CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcomes Study) has studied 10 061 patients in 39 countries between 2011 and 2017 with stable postmyocardial infarction but with ‘residual inflammatory risk’ (defined as persistent elevations of hsCRP >2 mg/L). Anti-inflammatory (canakinumab, a fully human anti-IL-1beta monoclonal antibody) therapy lowered the inflammatory biomarkers (IL-6 and hsCRP) of participants by 35%–40% when compared with placebo, effects that led to a 17% reduction in rates of recurrent heart attack, stroke, urgent need for revascularisation or cardiovascular death.12 On the other hand, in the 4786-patient Cardiovascular Inflammation Reduction Trial, low-dose methotrexate as compared with placebo did not reduce IL-1, IL-6 or hsCRP, as well as cardiovascular event rates.36
Inflammation can affect CA development and progression through several pathways. These include altered antiapoptotic signalling, increased angiogenesis and levels of DNA adduct formation, but it remains to be seen if hsCRP is a risk marker for CA progression or if it is causally related.27
Implications
The level of hsCRP is currently used for global cardiovascular risk prediction, as a tool to determine risk of DM and metabolic syndrome, and as a method to monitor and guide statin therapy,37 and may be important for monitoring CA progression and survival.27 Our results in this new large admixed cohort are consistent with previous studies that indicate that proinflammatory biomarkers like hsCRP are independently associated with mortality risk.37–39 Although the mortality rate in Brazil has declined between 1990 and 2015, the proportion of deaths attributable to NCDs has increased from 59.6% in 1990 to 75.8% in 2015, with CVD being responsible for 31.2% and CA for 17.4% of all deaths.40 The current results may point to an important marker of risk for the Brazilian population.
Conclusions
Our study shows that hsCRP levels, independent of a large set of lifestyle and clinical variables, could affect mortality prediction in a highly admixed population. The current results may point to an important marker of risk for the Brazilian population that could identify groups which may benefit from preventive strategies. Further studies are still required to determine whether hsCRP is simply a marker of underlying systemic response to inflammation or is a contributing cause.
What is already known on this subject
High-sensitivity C reactive protein (hsCRP) has been proposed as a marker of incident cardiovascular disease and vascular mortality, and may also be a marker of non-vascular mortality.
Most evidence comes from high-income and mainly North American or European cohorts.
What this study adds
This study extends previous research in this area and demonstrates that the risk of all-cause mortality increases progressively with increasing levels of hsCRP in a middle-income South American population.
The association is independent of age, sex, body mass index, self-rated race/ethnicity, schooling, alcohol consumption, smoking status, physical activity level, and fruits and vegetables consumption.
Significant graded association persists after exclusion of deaths in the first year of follow-up and suggests that these results are unlikely to be due to reverse causality.
The HR was unaffected by the exclusion of participants who had self-reported medical history of diabetes, depression, cancer and chronic obstructive pulmonary disease.
The current results may point to an important marker of risk for the Brazilian population that could identify groups which may benefit from preventive strategies.
Further studies are still required to determine whether hsCRP is simply a marker of underlying systemic response to inflammation or is a contributing cause.
Acknowledgments
The authors thank the staff and participants of the ELSA-Brasil study for their important contributions, the Rutherford Strategic Fund and the University of Warwick, UK.
References
Footnotes
Contributors CBM, FPC, MM: contributed to design, analysis, acquisition and interpretation, and drafted the manuscript. SMB: contributed to design, analysis, acquisition and interpretation, drafted the manuscript, and critically revised it. LG: contributed to acquisition and interpretation, drafted the manuscript, and critically revised it. ALR, PGV: contributed to interpretation, drafted the manuscript and critically revised it. DRMA, CJ: contributed to design and analysis. RHG, SMAM: contributed to interpretation and critically revised it.
Funding The ELSA-Brasil baseline study was supported by the Brazilian Ministry of Health (Science and Technology Department) and the Brazilian Ministry of Science and Technology (FINEP, Financiadora de Estudos e Projetos and CNPq, National Research Council) (grants 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ). SMB is a research fellow of the National Research Council (CNPq, grant number 300159/99-4). RHG is also a research fellow of the National Research Council (CNPq, grant number 301807/2016-7). ALR receives research grants from CNPq/Brazil (grants 465518/2014-1 and 310679/2016-8) and from the Fundação de Amparo à Pesquisa de Minas Gerais (FAPEMIG, Brazil; PPM-00428-17). CBM was supported by a Rutherford Strategic International Fellowship as part of the Universities UK International (UUKi) Rutherford Fund Strategic Partner Grants programme awarded to MM and FPC.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The research protocol was approved by the ethics committee of each participating institution and by the National Research Ethics Committee. All participants signed an informed consent that included permission for the storage of biological samples.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.