Article Text

Abstract
Background Low control and high demand in the places where people work has been shown to partially explain why those in lower socioeconomic positions experience poorer health than their counterparts in higher socioeconomic positions. It would seem likely then that experiences of control in the wider living environment, beyond people’s places of work, might also play a role in shaping these health inequalities. Our recent review of theory revealed potential pathways by which low control in the living environment might explain the social patterning of health via low control beliefs and low actual control.
Methods Based on the potential pathways identified in our review of theory, we conducted a systematic review of longitudinal studies on the relationship between low control in the living environment and social inequalities in health published by January 2019, in English.
Results Six studies were included in the review. Taken together, they provide evidence that lower social positions are associated with lower control beliefs and poorer health outcomes, in terms of heart disease, anxiety, depression and self-rated health, and that some of the association between low social position and health outcomes is explained by low control beliefs. No studies investigated the pathway from low actual control to poorer health in more disadvantaged groups.
Conclusion There is strong evidence from a small number of high-quality longitudinal studies that low perceived control in the living environment may play an important role in the pathways leading from low social position to poorer health and well-being. Further studies are needed to distinguish between the effects of having low control beliefs and having actual low control.
- control over destiny
- socioeconomic status
- inequalities
- social determinants
- health
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In public health it has long been argued that differences in the level of control or autonomy between socioeconomic groups may be an underlying cause of socioeconomic inequalities in health.1 2 Sen, for example, suggests that differences in the freedom to exercise choice over daily life underlie the inequalities in health observed between different groups within populations.3 Reflecting this perspective, the Global Commission on the Social Determinants of Health concluded that health inequalities are ‘caused by the unequal distribution of power, income, goods and services, globally and nationally’.4 Thus ‘the ability of people to deal with the forces that affect their lives, even if they decide not to deal with them’5 is proposed by some to be a fundamental social determinant of health.
The empirical evidence to support this assertion came initially from studies of ‘demand’ and ‘control’ and the generation of health-damaging stress in the work place.6 A systematic review of the evidence revealed that employees experiencing a combination of high demand but low control in their jobs experienced greater stress-induced symptoms; this can lead to poorer mental and physical health compared with counterparts who have a high degree of control over their work.7 In particular, a number of studies have shown that exposure to high demand with low control increase with declining occupational class, and may lead on to the observed socioeconomic inequalities in coronary heart disease (CHD).8
In light of this evidence, it would seem likely that experiences of control in the wider living environment, beyond people’s places of work, might also play a role in shaping health inequalities. In an earlier paper, we reported our synthesis of theories on how differences in control in the living environment could lead to socioeconomic inequalities in health9 at three levels: micro (individual), meso (community) and macro (societal). We produced a series of logic models to depict the hypothesised causal pathways from low control in the living environment to poorer health in less privileged groups and communities. Here, we report the findings from a systematic review of empirical evidence from longitudinal studies testing the hypothesised pathways leading to socioeconomic inequalities in health operating at the micro (individual) level.
Methods
We conducted a systematic review to address the question: what is the empirical evidence at the micro (individual) level to support or refute the hypothesised pathways from low control in the living environment to socioeconomic inequalities in health outcomes?
Logic model
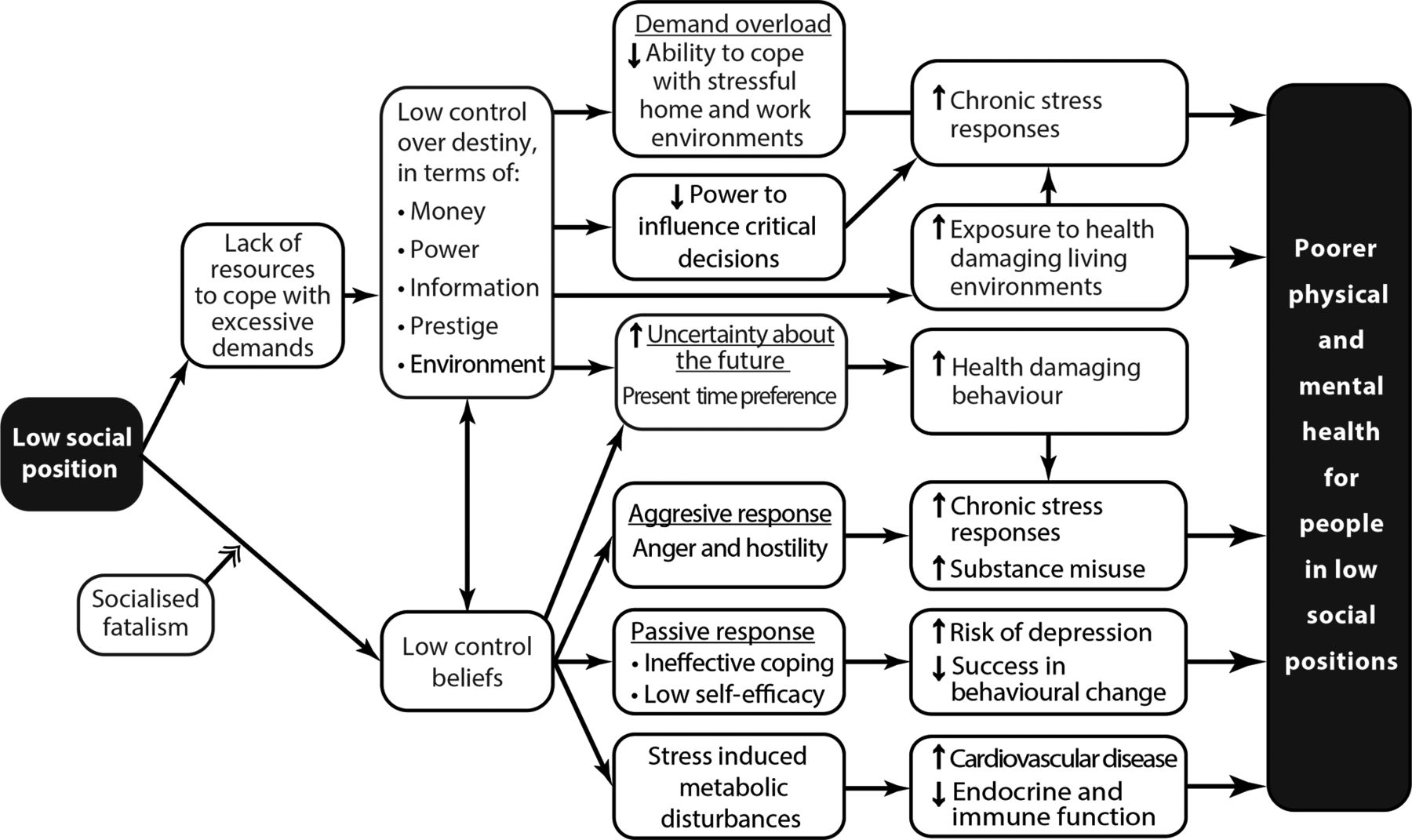
We used the logic model of micro-level pathways developed in our synthesis of theories to structure the searches9 (see figure 1). In this model two inter-related strands of theory connect the individual experience of low social position with poorer physical and mental health via lower ‘control over destiny’. One is concerned with ‘actual’ or ‘real’ control (depicted in the top half of figure 1) and relates to the degree of control that individuals are able to exercise over their living environment through the economic and social resources to which they have access. People in lower social positions have fewer resources, leading to a reduced ability to cope with stressful home environments, reduced power to influence critical decisions, and uncertainty about the future; all of which contribute to a higher prevalence of physical and mental health problems (via greater chronic stress, exposure to health-damaging environments and engagement in health-damaging behaviours). The ‘perceived control’ (or ‘control beliefs’) pathway depicted in the lower half of figure 1 suggests that the experience of low social position may lead to people having the perception that they have little or no control over decisions that affect their lives (‘low control beliefs’). Additionally, children growing up in low social positions may be socialised into having lower control beliefs than their more privileged counterparts. Low control beliefs might lead to three contrasting psychological responses:

Logic model of the theoretical pathways leading from low control to socioeconomic inequalities in health at the micro/individual level.
Anger and hostility, which may induce chronic stress and health-damaging behaviour (aggressive response).
Ineffective coping may induce depression and result in less effective behaviour change (passive response).
Stress may cause metabolic disturbance exacerbating disease risk factors.
In theory the two major pathways are connected, as low control beliefs may lead to low actual control and vice-versa.
Searches
We searched for reports of studies that included longitudinal data on the ‘perceived’ and ‘actual’ control pathways in eight electronic databases (MEDLINE and MEDLINE In-Process; EMBASE; PsycINFO; Social Policy & Practice; Social Sciences Citation Index; Conference Proceedings Citation Index—Social Sciences and Humanities; Conference Proceedings Citations Index—Science) in January 2019. Initial scoping of the literature revealed, as anticipated, problems with use of the term ‘control’, which also identified studies with ‘control’ groups. We therefore used the seminal studies already identified in our preliminary scanning of the literature (and in our critical review of theory9) to design search strategies tailored to each specific electronic database (see online supplementary file 1 for full MEDLINE strategy). We consulted key informants (including policy makers and academics) in appropriate fields to help identify relevant papers in press, and reports of evaluations commissioned by public and charitable bodies that were unavailable in electronic databases. We located additional studies through our reviews of theory and interventions and through scanning the reference lists of studies included in this review.
Supplemental material
Inclusion and exclusion criteria
We included studies reporting longitudinal data on the extent and nature of the relationship between control in the living environment and a measure of physical, social or mental health and well-being. Studies must explore pathways between control in the living environment, beyond people’s places of work and inequalities in health. To be included, studies had to have all of the following components:
Provide longitudinal data on the relationship between control and health.
Include free-living general populations.
Explore some form of interaction between people and their living environment.
Measure an individual’s control over decisions that affect their daily lives.
Disaggregate data based on some measure of individual socioeconomic status (SES) or relate to specific groups that are marked by some form of disadvantage.
Measure an individual’s health-related outcome, including well-being.
Criterion (a): We were interested in studies that provide longitudinal data exploring causal pathways rather than cross-sectional studies that merely explored associations. Criterion (b): We were not interested in studies in highly selected samples (eg, studies drawn from samples of patients in healthcare settings or from other residential environments). Criteria (c) and (d): Our definition of ‘control over destiny’ included measures of ‘actual control’—for example, a person’s control over material resources for the necessities of health—or ‘perceived control’—such as their control beliefs. Other terms in the literature that encapsulate these concepts include ‘power’, ‘empowerment’ and ‘autonomy’. We excluded studies from the psychological literature that examined perceived ‘locus of control’ of individuals as a personality trait, without reference to the actual socioeconomic or psychosocial conditions in which the individual lived and studies in which ‘mastery’ was conceptualised as self-control or mastery over one’s own emotions, rather than control over external decisions. Criterion (e): Studies had to provide data that helped explain the socioeconomic gradient in health. Criterion (f): We allowed a broad conception of health and well-being outcomes.
Quality assessment, data extraction and synthesis
The methodological quality of included studies was assessed using the Newcastle-Ottawa Quality Assessment Scale.10 The scale assess the quality of non-randomised studies using a ‘star system’ in which a study is judged on three broad perspectives: the selection of the study groups; the comparability of the groups; the ascertainment of either the exposure or outcome of interest for case-control or cohort studies, respectively. Two reviewers conducted all quality assessment independently, with disagreements resolved by consensus or by recourse to a third reviewer.
Reviewers extracted data from the included studies into predesigned and piloted forms. A second reviewer checked data for accuracy and completeness. Extracted data included: study aims, study design, setting (country) and main findings. Studies were synthesised narratively11 12 examining evidence for the hypothesised pathways in our logic models. Reporting is based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses equity extension (guidance for reporting the identification, extraction and synthesis of data in equity-focused systematic reviews)13 with results organised by health outcome.
Results
From an initial 56 210 references, six studies were identified that met the inclusion criteria and explored control at the individual/micro level (figure 2).

{kind=link}
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram depicting the flow of studies through the review. SES, socioeconomic status.
The six studies drew on samples from four large datasets:
British Whitehall II Study.
GLOBE study (Netherlands).
Groningen longitudinal ageing study (GLAS: Netherlands).
Midlife in USA.
Studies were conducted in high-income countries (two each from the UK, the Netherlands and the USA). Various health-related outcomes were measured (from self-rated general health to heart disease) and control was conceptualised in different ways. Measures encompassed control beliefs or ‘perceived control’, including self-reports of perceived individual autonomy, control beliefs and personal control. These concepts were measured using a variety of tools, some based on pre-existing (validated) tools such as Sherer’s General Self-Efficacy Scale, others were measured using unvalidated measures (eg, ‘control at home’). No studies included measures of ‘actual control’. All included studies provided high quality evidence relating to the hypothesised pathways. The online supplementary file 2 provides an overview of included studies.
Supplemental material
Empirical evidence for theoretical pathways
All six studies14–19 considered perceived control or control beliefs, as depicted through the pathways in the lower half of figure 1. No studies were identified that investigated the ‘actual control’ pathways, depicted in the upper half of the logic model in figure 1. Our synthesis, therefore, relates solely to perceived control or control beliefs.
Evidence across studies suggests that lower social positions are associated with both (1) lower control beliefs and (2) poorer health outcomes, and that a proportion of the association between low social position and health outcomes may be explained statistically by low control beliefs. One study suggests some support for the passive response to low control17 as depicted in our logic model (see figure 1). Findings are discussed in more detail, below.
Two of the six studies investigated the associations between low SES, low control beliefs and risk of CHD. Using data from the GLAS Cohort study in the Netherlands, Bosma and colleagues14 followed up 3 888 men and women, over 57 years old, without prevalent heart disease, over 5 years, to explore whether it was via their low control beliefs that low SES groups have higher risks of developing heart disease. They found perceived low control was more common among low socioeconomic groups (using the indicators of educational, occupational and income level), and was also related to risk of developing CHD over the study period. Adjusting for potential confounders, 30% of the socioeconomic inequalities in heart disease risk were accounted for by the SES differences in control beliefs, while only 4% were accounted for by the classical risk factors such as smoking, hypertension and unhealthy dietary habits. As the contribution of control beliefs was largely independent of the behavioural coronary risk factors, this suggests that low control beliefs may affect heart disease through mechanisms other than behavioural pathways.
Another study15 using the Whitehall II cohort of British civil servants, set out to differentiate the effects of perceived control in the home environment (as opposed to the work environment) on social inequalities in incident CHD events. This study followed 7 470 men and women over 8 years and found some evidence that low perceived control at home predicts the development of CHD among women but not among men. A larger proportion of women with self-reported CHD also reported low control at home compared with women without CHD. Furthermore, women from lower employment grades were over three times more likely to report low control at home compared with those from higher grades, and their elevated risk remained significant even after adjusting for financial problems and behavioural CHD risk factors.
Another study, using the Whitehall II cohort, addressed the pathways from control at home to poorer mental health. It investigated the hypothesis that a lack of perceived control in the home and work environments affects depression and anxiety differently for women and men and across three social class groups. Using data on 7 270 participants, women and men with low control at home were found to be at significantly greater risk of developing depression (women: OR=2.51, CI 1.77 to 3.56; men: OR=1.86, CI 1.52 to 2.28) and anxiety (women: OR=1.75, CI 1.22 to 2.51; men: OR=1.89, CI 1.52 to 2.35) over the 5-year study period, after adjusting for age and other potential confounders. Low perceived control and low employment grade; however, did not operate in the same way in women and men. Women in the lowest or middle employment grades who reported low control at home were at most risk for depression and anxiety. Men in the middle and highest grades were at greatest risk of both depression and anxiety if they reported low control at home.16
A fourth study based on the Dutch GLOBE study used retrospective data on 2 462 men and women to investigate the influence of childhood SES on adult self-rated health (touching on the ‘socialised fatalism’ pathway).17 Independent of adult social class, low childhood social class was related to self-rated poor health (OR 1.67, 95% CI 1.02 to 2.75) for participants whose fathers were unskilled manual workers versus participants whose fathers were higher grade professionals. Participants whose fathers were manual workers generally had more negative coping styles and psychological attributes, including low perceived control, which accounted for about half the association between childhood social class and self-rated poor health in adulthood.
Two further studies used longitudinal survey data from the USA. One18 investigated the association between education (a measure of SES) and health in a national sample and how this changed over 1 year among 2 436 men and women. Higher SES measured by education was associated with better self-rated general health at time one. Higher SES was also associated at time one with the hypothesised explanatory variables of better work and economic conditions, greater sense of control over future health and social support, and healthier lifestyles. Results of multiple regression analysis showed that 34% of the educational inequalities in health were explained statistically by differences in work and economic conditions, 8% by sense of control over future health and 13% by lifestyle factors. Over the 1-year time period, on average, self-rated general health declined over time, but the decline was significantly smaller with higher educational attainment. Analysis of hypothesised explanatory variables showed that 27% of the effect of education on the change in health from time one to time two was explained statistically by differences in work and economic conditions, 5.4% by sense of control over future health and 10.8% by lifestyle factors. A further US study with an 8 year time period19 investigated how psychosocial factors such as sense of control and social relations moderate the processes between SES and changes in specific health measures: chronic health conditions and depressive symptoms among 3 775 participants. The perception of high control was related to better health for both measures and moderated the relationship between SES and changes in health over time. In particular, the results suggested that perception of high control may be a critical protective factor for low SES individuals over time.
Discussion
Taken together the six studies included in this systematic review provide reliable longitudinal evidence. After adjusting for major confounders, low perceived control at the micro (personal) level is shown to explain statistically some of the association between low SES and greater deterioration in various mental and physical health outcomes for individuals. Two studies show that low control beliefs at home may account for up to a third of the observed socioeconomic inequalities in heart disease risk but that the effect seems to differ between men and women. Single studies reported on a number of further health outcomes. Briefly, women of lower SES who reported lower control at home were found to be at greatest risk for anxiety and depression, but for men being in higher grades put them at greatest risk. Self-rated poor health among adults that experienced low SES in childhood was associated with low perceived control. Decline in self-rated general health over 1 year was greater among lower socioeconomic groups (measured by educational level) and was partially mediated by sense of control. Finally, the perception of high control was related to better outcomes for chronic health conditions and depressive symptoms and moderated the relationship between SES and changes in health over time.
A number of limitations should be taken into account when interpreting the findings of this review. We stipulated that only studies with a longitudinal design were eligible. This meant that only the highest quality evidence was included but it also led to a small number of studies making it into the review. There are gaps in geographical coverage, with data from studies in high-income countries only. Applicability beyond these settings may be limited. Studies are yet to explore differential pathways by ethnicity, a potentially important social determinant. While gender emerged as a potentially important modifying factor, there is too little evidence to draw conclusions on its exact role in the reported pathways between control and inequalities in health. Perhaps most striking; however, we found no studies measuring ‘actual’ or ‘real’ control (the degree of control that individuals or communities are able to exercise over their living environment through the economic and social resources to which they have access). We could not, therefore, make an assessment of the nature of the evidence on the pathways leading from ‘actual control’ to socioeconomic inequalities in health (the proposed links between a sense of personal control and the objective conditions that may produce it). We also could not assess the connections between ‘perceived’ and ‘actual’ control, as we found no studies that investigated this question. This is a major evidence gap as the theoretical literature puts forward a pivotal role for actual control, over and above that of perceived control.9
Future studies could learn from the developments that have taken place in measurement of ‘actual control’ in relation to gender discrimination, outlined in our companion review20 and from studies in the work environment. Measures of ‘actual control’ used in the gender studies were applied to situations of profound restrictions on women’s choice and movement in some societies. Measures, for example, included whether the woman was allowed out of the home unaccompanied, or without having to seek permission from of a male relative; whether she could decide to take a sick child for medical treatment without seeking permission from a male relative. Many studies developed autonomy indices, combining several measures of what women reported they were able to do or not do in daily decision-making.20 Some were well tested and validated but most were based on self-report. This means that reliability (and comparability) of the measures could not be guaranteed. Measures of ‘actual control’ used in work studies capture an individual’s potential control over his/her tasks and his/her conduct during the working day (including, eg: task organisation, time pacing, organisational policy influence and control over potential uncertainties).6 Future research should provide more detail on the mediating factors between low control and poor health identified in our review of theory. The current evidence does not make clear whether the influence of low perceived control operates through increased chronic stress reactions, reduced success in behavioural change or some other factor. Future studies could use long-term in-depth ethnographic methods to provide further context for the causal pathways that have been proposed.
This is the first systematic review of empirical evidence that considers whether ‘control over destiny’ at the micro (individual) level leads to socioeconomic inequalities in health. Building on our review of theory,9 it reveals the value of control for understanding the determinants of health and health inequalities in the places where people live and for designing interventions to target these inequalities. It extends our understanding of control as a social determinant of health not just in the places where people work,8 21 but also in their living environment. In so doing, it reveals an important gap in the empirical evidence to support or refute the theoretical pathways from low social position or poor socioeconomic circumstances to poorer population health at the micro level. Methodologically, we demonstrate how logic models of the theoretical pathways can be used as frameworks to structure searches of observational evidence in ways that inform the substantive public health debate. The stringent inclusion criteria strengthen the degree to which we could examine causality within the proposed pathways between low control and health.
Conclusion
There is strong evidence from a small number of high-quality longitudinal studies that low perceived control over destiny in the living environment may play an important role in the micro-level pathways leading from low social position to poorer health and well-being. Further, this review reveals the substantial gaps in the observational evidence for the ‘actual control’ pathway. It suggests further research priorities to gain greater understanding of how low control in the living environment may operate to influence health.
What is already known on this subject
There is empirical evidence to indicate that control in the work environment might contribute to the social gradient in health.
Our recent review of theory suggests some plausible pathways by which control in the wider living environment might also contribute to these observed health inequalities.
What this study adds
This is the first systematic review of the empirical evidence for the hypothesised pathways at the micro-level from control in the living environment to socioeconomic inequalities in health.
Evidence from high-quality longitudinal studies reveals that the association between low social position and poorer health outcomes is explained statistically in part by low control beliefs.
References
Footnotes
Contributors MW conceived of the review published in this manuscript. LCO and AP conducted the review with supervision from MW and assistance from SN. LCO led in the writing of this manuscript with MW. AS, MP and MW guided the review process and the writing of this manuscript at all stages.
Funding This study was supported by Department of Health and Social Care Policy Research Programme.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.