Article Text

Abstract
Background Unexplained deaths in infancy comprise ‘sudden infant death syndrome’ (SIDS) and deaths without ascertained cause. They are typically sleep-related, perhaps triggered by unsafe sleep environments. Preterm birth may increase risk, and varies with ethnicity. We aimed to compare ethnic-specific rates of unexplained infant death, explore sociodemographic explanations for ethnic variation, and examine the role of preterm birth.
Methods We analysed routine data for 4.6 million live singleton births in England and Wales 2006–2012, including seven non-White ethnic groups ranging in size from 29 313 (Mixed Black-African-White) to 180 265 (Pakistani). We calculated rates, birth-year-adjusted ORs, and effects of further adjustments on the χ2 for ethnic variation.
Results There were 1559 unexplained infant deaths. Crude rates per 1000 live singleton births were as follows: 0.1–0.2 for Indian, Bangladeshi, Pakistani, White Non-British, Black African; 0.4 for White British; 0.6–0.7 for Mixed Black-African-White, Mixed Black-Caribbean-White, Black Caribbean. Birth-year-adjusted ORs relative to White British ranged from 0.38 (95% CI 0.24 to 0.60) for Indian babies to 1.73 (1.21 to 2.47) for Black Caribbean (χ2(10 df)=113.6, p<0.0005). Combined adjustment for parents’ marital/registration status and mother’s country of birth (UK/non-UK) attenuated the ethnic variation. Adjustments for gestational age at birth, maternal age and area deprivation made little difference.
Conclusion Substantial ethnic disparity in risk of unexplained infant death exists in England and Wales. Apparently not attributable to preterm birth or area deprivation, this may reflect cultural differences in infant care. Further research into infant-care practices in low-risk ethnic groups might enable more effective prevention of such deaths in the general population.
- ethnicity
- infant mortality
- inequalities
- cohort studies
This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
In 2015, about 7% of approximately 2500 annual deaths under the age of 1 year in England and Wales were ‘unexplained deaths in infancy’ (UDI),1 2 ie, recorded as ‘sudden infant death syndrome’ (SIDS, 60%) or without any ascertained cause (40%).3 4 Broadly equivalent to ‘sudden unexpected death in infancy’ (SUDI) and ‘sudden unexpected infant death’ (SUID),5 these deaths are typically ‘sleep-related’, occurring in circumstances consistent with failure of arousal in response to hypercarbia and hypoxia triggered by unsafe sleep environments.6 Risk factors identified in research studies include sleep position (front or side), inappropriate sleep surfaces, bed-sharing (particularly in combination with parental alcohol and/or drug use, or other risk factors), not sleeping in the same room as the parents, use of soft bedding, maternal smoking (prenatal or environmental) and not breastfeeding.6 7 Genetic alterations may increase vulnerability to UDI, but there is currently no evidence that causation has a strong heritable component.7
Striking ethnic disparities in rates of SUID or SUDI are reported in the USA8 and New Zealand.9 Until recently, there were no comparable National Statistics for England and Wales, because the data collected at birth and death registration did not include the ethnicity of either the baby or the mother. Since 2005, however, the Office for National Statistics has linked birth registrations with the ‘NHS Numbers for Babies’ dataset, which contains routine information recorded when the baby’s National Health Service number is generated, including the baby’s ethnicity (as reported by the mother) and gestational age at birth.10 11 Univariable analyses of births in 2005 found relatively high incidence of both preterm birth11 and SIDS12 among Black Caribbean babies in England and Wales, suggesting the possibility that ethnic variation in risk of UDI might be influenced by gestational age at birth. Preterm birth is associated with an increased risk of SIDS, and might be on the causal pathway, for example through incomplete development of the autonomic system that is responsible for arousal.6
We aimed to compare ethnic-specific national rates of UDI during 2006–2012, explore the extent to which sociodemographic factors might account for any ethnic disparities, and test the prior hypothesis that preterm birth might contribute to the relationship between ethnicity and risk of UDI.
Methods
Study design and data sources
We conducted a national birth cohort study, using routinely-collected administrative data. The study hypothesis arose before inspection of the data. The cohort consisted of all singletons born alive at 22+weeks’ gestation in England and Wales from 1 January 2006 to 31 December 2012. The Office for National Statistics provided an anonymised data extract linking birth and death registrations with the NHS Numbers for Babies dataset.11 Linkage methods and quality evaluation are described elsewhere.10 13 We further cleaned the data by removing records with missing or implausible data, as follows: gestation recorded as 43+weeks; birth weight missing; birth weight more than twice the IQR above or below the median within sex–gestation–ethnicity strata of the dataset; death not classifiable as explained or not; and maternal country of birth not classifiable as UK or non-UK.
Variables
Following methodology used by the Office for National Statistics,14 based on the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10), we defined UDI as death at age less than 1 year with either (a) any mention of R95 (SIDS) among the (up to 15) ICD-10 codes recording the causes of death, or (b) no mention of any cause except ICD-10 code R99 (’other ill-defined and unspecified causes of mortality').
Ethnicity coding in the NHS Numbers for Babies dataset is compatible with the categories used in the 2001 Census.11 We used the following ethnic groups: White British, White Non-British, Pakistani, Indian, Bangladeshi, Black African, Mixed Black-African-White, Black Caribbean, and Mixed Black-Caribbean-White. We created an ‘Other and Unspecific’ group by combining all the remaining stated categories, which were either very small (eg, Chinese) or only broadly defined (eg, ‘Any other Black background’). We included a separate ‘Unstated’ group.
Covariates were categorised as follows: gestational age at birth (22–31, 32–36, 37+weeks); baby’s sex (boy, girl); mother’s country of birth (UK, non-UK); mother’s age at delivery (<20, 20–24, 25–29, 30+years); parents’ marital/registration status based on the registration of the baby’s birth (sole registration, birth jointly registered by two parents living at different addresses, joint registration by two parents at the same address, birth within marriage)11; area deprivation based on the mother’s usual address at birth registration, measured as quintile categories of the respective national Index of Multiple Deprivation for England 201515 and for Wales 2014.16
Statistical analysis
We calculated crude rates of UDI per 1000 live singleton births by ethnic group over the full study period 2006–2012. We estimated risk for each ethnic group relative to White British by using a logistic regression model to calculate ORs with adjustment for potential confounding by birth year, which was fitted as a linear trend. To assess the extent to which other factors in our dataset might account for the ethnic variation in risk, we fitted exploratory models that were adjusted for these covariates first individually and then cumulatively, choosing each additional factor to minimise the χ2 for ethnic variation, based on the likelihood ratio test statistic. To avoid potential problems with sparse data, we did not include interaction terms. All analyses were done in Stata V.13, using two-sided tests with a 5% significance level.
Sensitivity analyses
We treated quintile categories of area deprivation for England and for Wales as equivalent in the main analysis; to check sensitivity to this simplification, the analysis was repeated using a 10-level factor representing each combination of England/Wales and the five quintiles. We did not include birth weight in the main analysis because it is very closely associated with gestation; for completeness, the analysis was repeated replacing gestation with birth weight, expressed either as categories (<1.5 kg, 1.5–<2.5 kg, 2.5–<4 kg, 4+kg) or as ‘small for gestational age’ (10% cut-off within sex–gestation strata of the dataset). To check for sparse-data bias, which can occur in maximum likelihood estimation where there are small numbers of events in some categories,17 the analysis was repeated using a penalised-likelihood method.18
Public involvement
Representatives of organisations concerned with infant health and/or work related to ethnic minority groups were consulted at the design and interpretation phases of the study and will be involved in dissemination of the results.
Results
The source file contained data on 4 744 666 babies. We successively excluded 16 695 for implausible gestation, 20 999 for missing birth weight, and 72 040 for implausible birth weight, leaving 4 634 932. Of the 15 001 infant deaths in the reduced dataset, 75 deaths had no ICD-10 cause codes. For these deaths, we used the ‘underlying cause’ if supplied (38 postneonatal deaths, nearly all in babies born in 2007, and 12 neonatal deaths, all in babies born in 2012).19 We were unable to classify the remaining 25 neonatal deaths as explained or unexplained and excluded these babies (all born in 2007) from the analysis. We further excluded 143 babies whose mother’s country of birth could not be classified as UK or non-UK. After exclusions (2.3%), 4 634 764 babies remained for analysis (table 1); the proportion of births with unstated ethnicity was 6%, decreasing from 10% in 2006 to 3% in 2012, and there were no other missing data.
Risk of unexplained death in infancy, by ethnic group and other factors. Live singleton births at 22+weeks, England and Wales 2006–2012
Figure 1 shows the distributions of maternal and infant sociodemographic characteristics by ethnic group (data in online supplementary table S1). The proportion of births registered outside marriage was low (4%–5%) for all three South Asian groups, and high for the Black Caribbean (74%) and Mixed Black-Caribbean-White (79%) groups. The proportion of mothers born in the UK was low for the Black African group (7%), and high for Mixed Black-Caribbean-White (91%) and White British (96%). The proportion of births in the most deprived quintile was 23%–24% for the White British, White Non-British and Indian groups, and 50%–60% for the Black Caribbean, Black African, Pakistani and Bangladeshi groups. The proportion of preterm births was higher for Black Caribbean babies (8%) than others (5%–6%).
Supplementary file 1
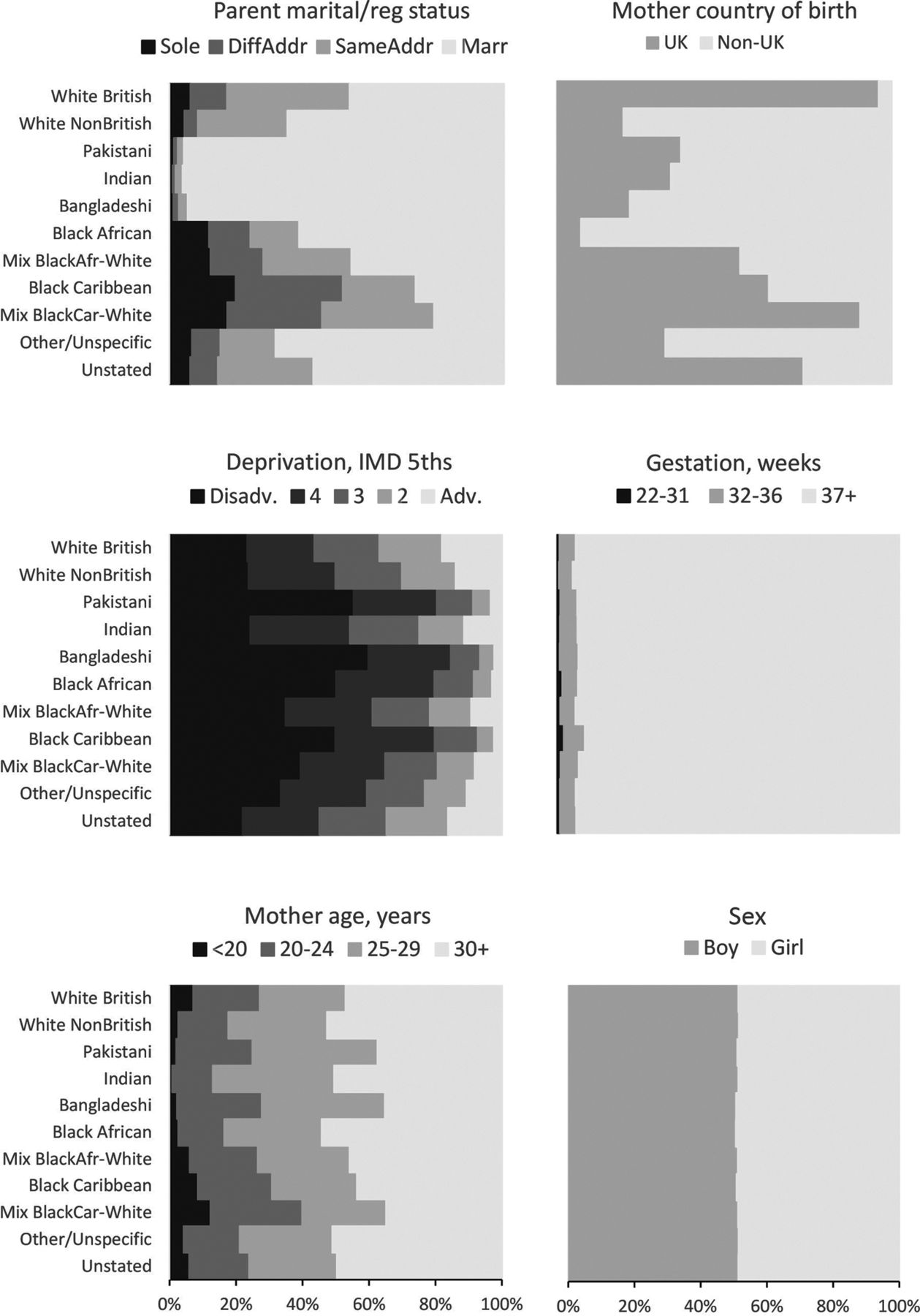
Distributions of covariates by ethnic group. Live singleton births at 22+weeks, England and Wales 2006–2012. Data are shown in online supplementary table S1. IMD, Index of Multiple Deprivation.
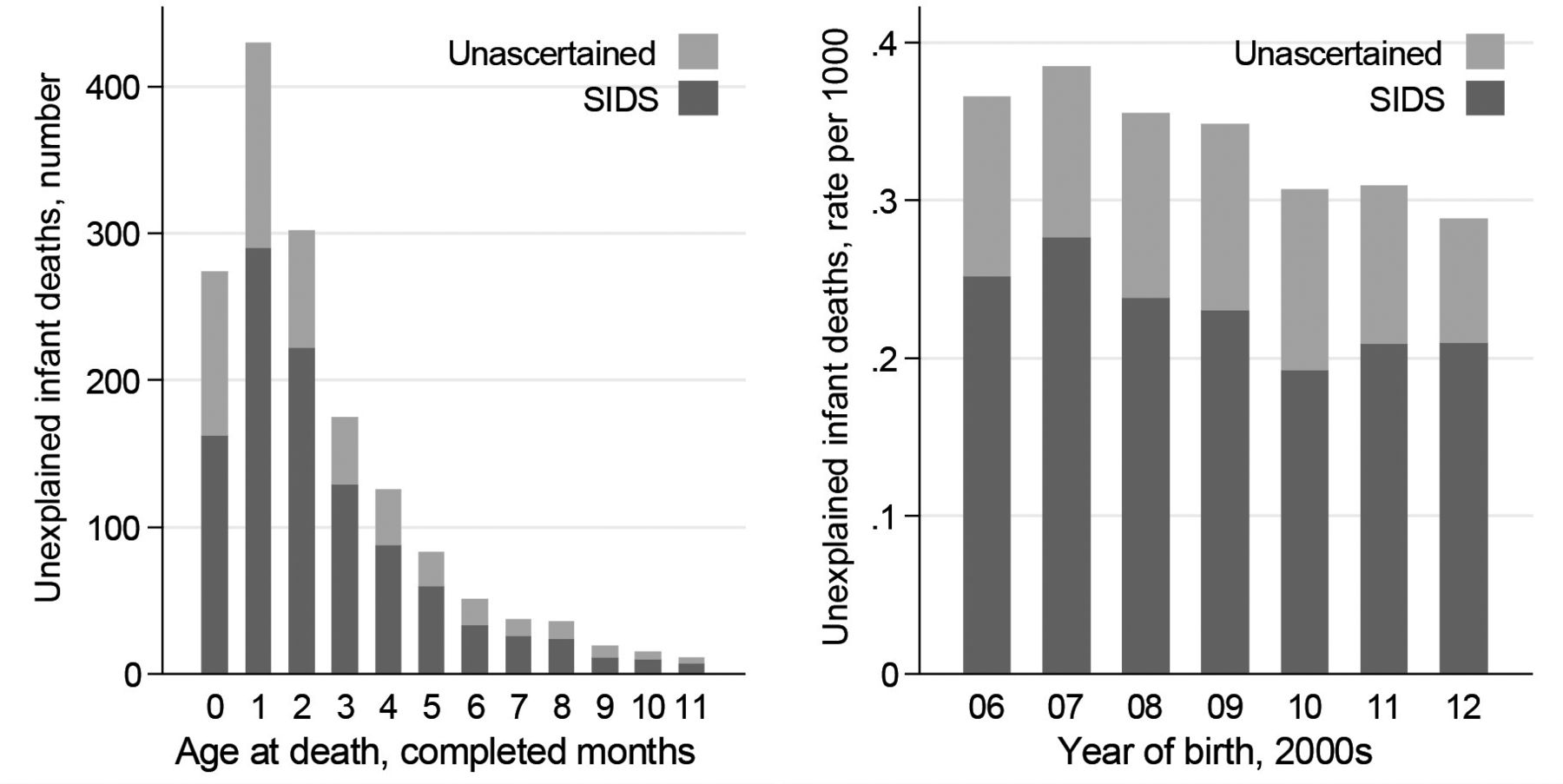
There were 1559 UDIs, with highest frequency in the second month after birth (figure 2; data in online supplementary table S2). The proportion coded as SIDS (68% overall) varied little with age at death or with birth year. Each covariate was associated with the risk of UDI in the general population after adjustment for potential confounding by birth year (table 1): risk was greater for babies born outside marriage (with risk increasing over joint registration by two parents living at the same address, joint registration at different addresses and sole registration), UK-born mothers, higher levels of area deprivation, male babies, younger mothers and earlier gestational age at birth.
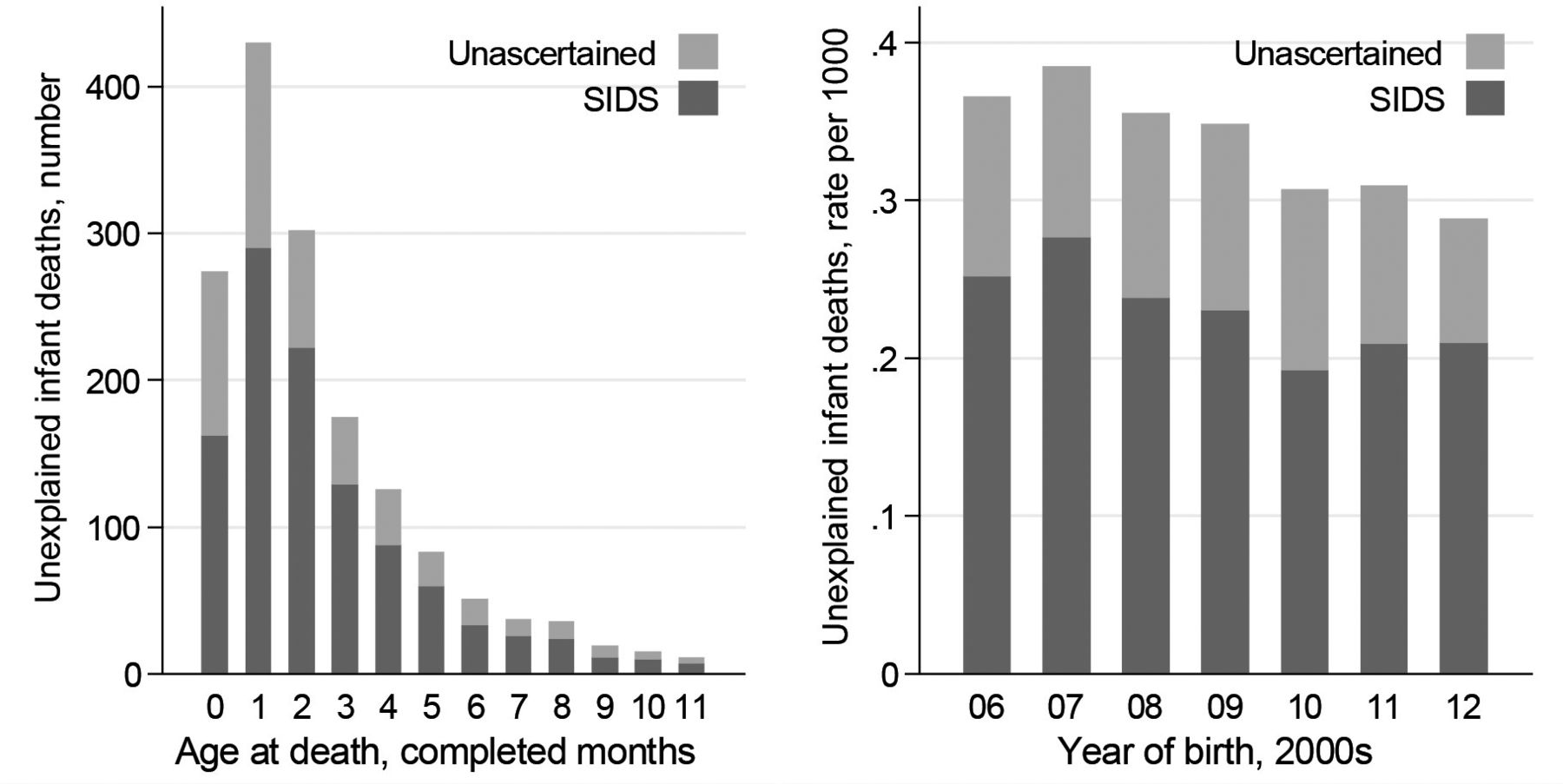
Unexplained deaths in infancy, by recorded cause. Number of unexplained deaths in infancy, by age at death. Crude rate of unexplained infant death per 1000, by year of birth. Live singleton births at 22+weeks, England and Wales 2006–2012. SIDS, sudden infant death syndrome. Data are shown in online supplementary table S2.
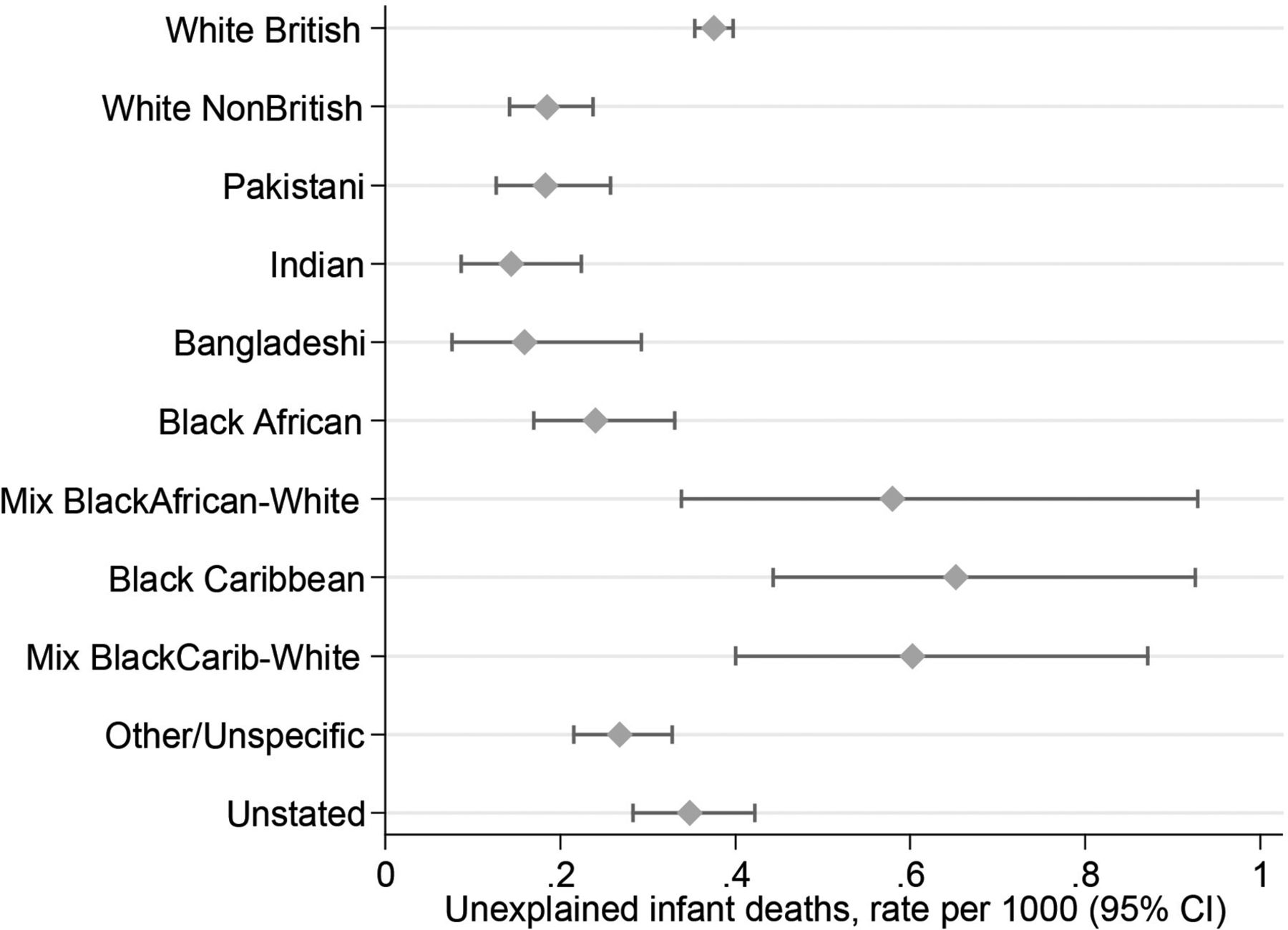
The crude rate of UDI was 0.34 per 1000 live singleton births, varying from 0.1–0.2 for the South Asian, White Non-British and Black African groups, to 0.4 for White British, and to 0.6–0.7 for Black Caribbean and both Mixed Black-White groups (table 1, figure 3). The highest rate (Black Caribbean) was 4.6 times the lowest (Indian). Adjusting for birth year, there was statistically significant ethnic variation in risk (χ2(10 df)=113.6, p<0.0005), with ORs relative to White British ranging from 0.38 (95% CI 0.24 to 0.60) for Indian babies to 1.73 (95% CI 1.21 to 2.47) for Black Caribbean (table 1).

{kind=link}
{kind=link}
{kind=link}
Unexplained death in infancy, by ethnic group. Crude rate of unexplained infant death (95% CI) per 1000 live singleton births at 22+weeks, England and Wales 2006–2012. Data are shown in table 1.
In exploratory analyses, the ethnic variation in risk of UDI remained statistically significant when the ORs were adjusted for each covariate individually; the residual ethnic variation was least after adjustment for parents’ marital/registration status (χ2=26.7, p=0.003) and greatest after adjustment for deprivation (χ2=163.3, p<0.0005) (table 2). When the factors were fitted cumulatively, in the order that minimised the χ2 for ethnic variation at each stage, the ethnic variation ceased to be statistically significant after joint adjustment for parental marital/registration status and maternal country of birth (χ2=7.8, p=0.6); with these two adjustments none of the ethnic groups was significantly different from White British (table 2). Further adjustments for deprivation, sex, gestation and maternal age made little difference.
Exploratory analyses. Covariate-adjusted ORs for unexplained death in infancy, by ethnic group relative to White British. Live singleton births at 22+weeks, England and Wales 2006–2012
Sensitivity analyses did not materially affect the findings. Adjustments for birth weight or ‘small for gestational age’ were less effective than adjustment for gestation in reducing the χ2 for ethnic variation. Modelling the deprivation scores for England and Wales separately, or using penalised rather than maximum likelihood methods, made little difference.
Discussion
Statement of principal findings
There is nearly fivefold variation in risk of UDI between ethnic groups in England and Wales. This variation does not appear to be explained by preterm birth, baby’s sex, maternal age, or area deprivation. The risk is lowest for Indian, Bangladeshi, Pakistani, White Non-British and Black African babies; intermediate for White British; and highest for Mixed Black-African-White, Mixed Black-Caribbean-White and Black Caribbean. Parents’ marital/registration status (married, joint registration by two parents living at the same address, joint registration with different addresses and sole registration by one parent) and mother’s country of birth (non-UK/UK) seem to jointly account for much of the ethnic disparity in risk, perhaps representing cultural variation in causal factors.
Strengths and weaknesses of the study
This is the first study to quantify risk of UDI in England and Wales by ethnicity. Based on a recent 7-year national birth cohort, the study is large enough to yield precise estimates for relatively homogeneous minority ethnic groups. Some of the findings may be generalisable to similar groups resident in other countries. Several potentially important covariates are examined. Studies based on routine data are particularly valuable for this research area, because much of the existing evidence for risk factors derives from interview-based case–control studies, with potential for participation and reporting bias. The study is limited by a lack of information for individual families on infant sleep practices and other lifestyle factors, although prior national surveys provide some relevant data at the subpopulation level, as discussed below. The proportion of births with unstated ethnicity is 6% overall, decreasing with time, but the characteristics of such births have been shown to resemble those of White British,11 and our analysis is adjusted for potential confounding by birth year. We are unable to generalise from the White Non-British group because it is very diverse: maternal countries of birth include Poland (24%); UK (20%); Lithuania and Romania (4% each); South Africa and Turkey (3% each); France, Slovakia, Ireland, the USA, Germany, Latvia, Portugal, Australia, Czech Republic (2% each); and >200 other countries worldwide. Social disadvantage is measured by area-based deprivation, which does not necessarily reflect individual socioeconomic status. Although the ethnic group recorded in the NHS Numbers for Babies dataset is nominally the ethnicity of the baby as reported by the mother to the health professional notifying the birth, in practice it may sometimes have been the ethnicity of the mother or decided by the health professional without asking the mother.11 Any resulting misclassification might tend to underestimate differences between ethnic groups; the size of this potential bias is uncertain but probably small.
Relation to other studies
To our knowledge, there are only three comparable UK studies.12 20 21 All examined SIDS (not UDI), and two date from the 1980s: one of these was regional (not national) and the other used mother’s country of birth as a surrogate for ethnicity. A univariable analysis of ethnic variation in infant mortality for babies born in England and Wales in 2005 noted higher risk of SIDS in Caribbean babies.12 In Birmingham (England) 1981-83, ethnic differences in risk of SIDS (low for Asian and high for Afro-Caribbean babies) persisted after controlling for social class, birth weight and maternal age,21 consistent with our finding that individual adjustment for area deprivation, gestation and maternal age made little difference to the ethnic variation. In England and Wales 1982-85, babies of mothers born in Bangladesh, West Africa, East Africa, India, Pakistan and the Caribbean had lower SIDS rates than babies of UK-born mothers20; in our study, Black Caribbean babies had higher UDI rates than White British, but their mothers were mostly born in the UK. Internationally, our findings are consistent with a pattern of relatively low risk for Asian groups (i.e. originating in East, South East or South Asia) within majority White populations, as reported in USA 2011-14,8 New Zealand 2003-079 and (using maternal country of birth) Victoria (Australia) 1985-89.22 Bearing in mind potential differences in culture, our results for the Black Caribbean and Mixed Black-White groups also appear consistent with the relatively high risk of SUID reported for Black Non-Hispanic babies in the USA.8
Meaning of the study
In the UK from the mid-1950s to the late 1980s, professional advice to use the front or side sleeping position influenced a whole generation of mothers, and was almost certainly a real cause of SIDS.23 Subsequent public health campaigns have aimed to correct this advice, stressing sleep position among other aspects of ‘safe sleep’.24 Nevertheless, a recent multiagency review set in the West Midlands (England) reported that ‘most SUDI still occur in hazardous sleep environments, despite public health campaigns’.25 This suggests that, among ethnic groups with high proportions of UK-born mothers, prevalence of unsafe sleep practices may be associated with inaccessibility to health messages, and hence perhaps with sociodemographic characteristics. Parental marital/registration status, in particular, may represent a constellation of risk factors: a survey of maternity-care users in England in 2007 found that single mothers were less likely to access timely care, attend NHS antenatal classes, or have a postnatal check-up.26 Unfortunately, direct evidence on relevant infant care practices is very limited: for example, a comparison of 20 Afro-Caribbean with 33 White British babies in East London found that the Afro-Caribbean babies were more likely to share the parental bed and to ‘prefer’ front sleeping, but numbers were very small, the participating parents were volunteers and more than one preferred sleep position could be reported, with no indication of frequency.27
Protective infant-care traditions may tend to persist in ethnic groups with high proportions of mothers born outside the UK. In 1991, shortly before the start of the national ‘Back to Sleep’ campaign, a survey of multiparous mothers attending an antenatal clinic in Birmingham found that 34% of 172 South Asian mothers, or 47% of those who had lived in the UK for less than 5 years, reported placing their babies on their backs for sleep, compared with 6% of 202 White mothers.28 The authors commented that the South Asians were probably continuing practices learnt from previous generations, facilitated by the active involvement of older members of the extended family. Similarly, a Welsh qualitative study found that White babies might sleep in their parent’s room for a few months but would then be encouraged to ‘get used’ to sleeping alone, whereas Bangladeshi babies were less likely to be alone at any time and would remain with adults during daytime sleeping.29 In Bradford (England) 2008-09, a large telephone survey found that Pakistani parents were more likely than White British to report that their babies bed-shared or used a pillow; however, reported alcohol use was rare,30 and a qualitative study in the same population found that the typical ‘pillow’ was a traditional small firm headrest designed to prevent flattening of the skull while sleeping on the back, not a soft European-style pillow.31 It has been suggested that similar small headrests used in East Asia may reduce the risk of rolling over to the front position.32 Further research is needed, bearing in mind current concern about the safety of ‘infant sleep positioners’.7 33 34
Although maternal smoking and not breast feeding are associated with increased risk of sleep-related infant death in the general population,7 the ethnic patterns of tobacco use and breast feeding seen in UK national survey data do not seem entirely consistent with the ethnic pattern of UDI seen in our study. Black Caribbean mothers in the Millennium Cohort Study (MCS) had a higher rate of breast feeding initiation,35 and a lower rate of discontinuation before 4 months,36 than any other ethnic group except Black African and ‘Other White’, whereas Black Caribbean babies in our study had the highest risk of UDI. Self-reported current smoking in the MCS was rare among South Asian (particularly Bangladeshi) and Black African mothers, and relatively frequent among ‘Other White’, White British and Black Caribbean mothers.37 In the 2004 Health Survey for England, however, young Bangladeshi women reported chewing (not smoking) tobacco, and had higher prevalence of cotinine in saliva assays than young Pakistani, Indian or African women, while Bangladeshi men had higher prevalence of cigarette smoking, and cotinine, than men in any other minority ethnic group or the general population.38 Thus, Bangladeshi babies could be exposed to components of tobacco both prenatally (through their mothers’ chewing and secondhand smoking) and postnatally (through environmental smoke). Against this background, Bangladeshi babies in our study had the second-lowest risk of UDI.
Policy implications and future research
Safe-sleep campaigns in the UK should target the ethnic groups that experience higher rates of UDI. Further research into ethnic-specific infant care practices is required, and potentially protective customs in South Asian families should be evaluated. Implications for the aetiology of UDI should be considered.
What is already known on this subject
Striking ethnic disparities in risks of ‘sudden unexpected infant death’ (SUID) or ‘sudden unexpected death in infancy’ (SUDI) exist in the USA and New Zealand.
Comparable UK data have recently become available, making it possible for the first time to investigate national variation in risk among the ethnic groups resident in England and Wales.
What this study adds
There is nearly fivefold variation between ethnic groups in England and Wales in risk of ‘sudden infant death syndrome’ (SIDS) and other unexplained death in infancy.
The variation does not seem to be attributable to preterm birth, maternal age or area deprivation, and may reflect cultural differences in infant care.
Further research into infant-care practices in low-risk ethnic groups might enable more effective prevention of these deaths in the general population.
Acknowledgments
We thank Bliss, the Race Equality Foundation, Sands and the Lullaby Trust for their helpful contributions to the patient and public involvement consultation for this project.
References
Footnotes
Contributors JH conceived the study and all authors contributed to the design. Data acquisition was primarily conducted by JH, and data cleaning and management by YL. Analyses were performed by MEK and supported by MAQ and JH. MEK drafted the initial manuscript and MAQ, JJK, ND, YL and JH significantly contributed to revising it. All authors read and approved the final manuscript.
Funding This paper reports on an independent study which is funded by the National Institute for Health Research Policy Research Programme in the Department of Health and Social Care (grant no 108/001).
Disclaimer The views expressed herein are those of the authors and not necessarily those of the Department of Health and Social Care.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved by the National Research Ethics Service Committee South Central—Oxford B (reference 15/SC/0493).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The Office for National Statistics provided data for this study under an agreement which allows the data to be used only for the programme of infant mortality work of which this is a part.