Article Text

Abstract
Background Stressful family conditions may contribute to inequalities in child development because they are more common among disadvantaged groups (ie, differential exposure) and/or because their negative effects are stronger among disadvantaged groups (ie, differential impact/susceptibility). We used counterfactual mediation analysis to investigate to what extent stressful family conditions contribute to inequalities in child development via differential exposure and susceptibility.
Methods We used data from the Generation R Study, a population-based birth cohort in the Netherlands (n=6842). Mother’s education was used as the exposure. Developmental outcomes, measured at age 13 years, were emotional and behavioural problems (Youth Self-Report), cognitive development (Wechsler Intelligence Scale for Children) and secondary education entry level. Financial and social stress at age 9 years were the putative mediators.
Results Differential exposure to financial stress caused a 0.07 (95% CI −0.12 to −0.01) SD worse emotional and behavioural problem -score, a 0.05 (95% CI −0.08 to −0.02) SD lower intelligence score and a 0.05 (95% CI −0.05 to −0.01) SD lower secondary educational level, respectively, among children of less-educated mothers compared with children of more-educated mothers. This corresponds to a relative contribution of 54%, 9% and 6% of the total effect of mother’s education on these outcomes, respectively. Estimates for differential exposure to social stress, and differential susceptibility to financial or social stress, were much less pronounced.
Conclusion Among children of less-educated mothers, higher exposure to financial stress in the family substantially contributes to inequalities in socioemotional development, but less so for cognitive development and educational attainment.
- health inequalities
- child health
- life course epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous research has documented the relationship between material deprivation, poor parental mental health and poor family functioning, and worse developmental outcomes of children. To what extent these stressful family circumstances account for the large inequalities in child development and childhood education between children from various social backgrounds— and whether this occurs via the process of differential exposure and/or differential impact/susceptibility—is unknown.
WHAT THIS STUDY ADDS
Differential exposure to stressful family conditions had a large contribution to the modest impact of mother’s education on child emotional and behavioural problems, and a limited contribution to the substantial impact of mother’s education on child cognitive development and secondary educational level. Differential susceptibility to stressful family conditions did not contribute to inequalities in child development and educational attainment.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Reducing exposure to stress among families with less-educated parents may be an effective strategy to reduce inequalities in children’s socioemotional development but is less likely to tackle inequalities in cognitive development and childhood education. Future research is needed to gain a better understanding of the mechanisms that account for these inequalities.
Introduction
Socioeconomic conditions in early life influence child health and development,1 2 as well as educational opportunities,3 both of which influence adult health and health determinants.4 5 Yet, there is a paucity of evidence on the mechanisms through which childhood conditions contribute to socioeconomic inequalities in development and educational attainment. Understanding these mechanisms is vital for the development of more effective strategies to address health inequalities early in life.6
Three childhood outcomes are particularly relevant for giving children a ‘healthy springboard’, that is, a set of personal assets and skills that provide them with the opportunity to lead a healthy life in adolescence and adulthood: socioemotional development, cognitive development and childhood education.7 Socialemotional and cognitive skills, and educational opportunities, aid children in improving their social, economic and health outcomes across the life course.7 As this set of personal ‘health assets’ is a major predictor of future health behaviours, mental healt and physical health, it is important to unravel how inequalities in these health assets arise.
One of the most important contextual determinants of child development is the family environment. The family environment contributes, via several pathways, to children’s socioemotional and cognitive development and childhood education.1 The Family Stress Model posits that stressful family conditions, both financially and socially, are important pathways to explain inequalities in these health assets.8 More specifically, children of less-educated parents are more often exposed to financial hardship, parental mental health problems and poorer family functioning.9 These stressful family conditions affect the home learning and psychosocial environment, and may negatively impact children’s socioemotional development, cognitive development and school success.9 Indeed, previous studies show that family stressors partly explain the association between family socioeconomic position and children’s developmental outcomes.10 11 Similarly, ‘adverse childhood experiences’, that is, a set of childhood traumatic events ranging from direct maltreatment to more general household dysfunction, have also been shown to mediate the association between socioeconomic background and children’s mental health.12
Besides being differentially exposed to stressful family conditions, children of less-educated parents may also be disproportionally affected by these stressful family conditions. For example, more-educated parents generally are able to draw on a larger and more diverse social network to acquire social support, are better able to find and navigate through various institutions that may be beneficial to child development, and have more financial resources available to compensate for unfavourable deviations in trajectories of child development.13–15 Consequently, children from more-educated parents benefit from various advantageous resources that may buffer the negative effect of stressful family conditions,16 although previous research has not always found evidence for this differential effect.17 18
Stressful family conditions may, thus, contribute to inequalities in child development and childhood education via the processes of differential exposure and differential impact/susceptibility.19 (Please note that in the context of our study ‘differential susceptibility’ refers to a differential effect of a particular mediator across groups, which differs from the usage of this terminology as applied in literature on the ‘differential susceptibility hypothesis’20). Extant epidemiological research, however, tends to consider these processes in isolation, because they largely rely on different methods, that is., mediation analysis to investigate differential exposure and interaction/moderation analysis to investigate differential impact/susceptibility. Advances in counterfactual mediation analysis enable researchers to consider both processes simultaneously and to estimate how much a particular mediator contributes to health inequalities because (1) the mediator is unevenly distributed across groups (differential exposure) and/or (2) because the effect of the mediator differs across groups (differential impact/susceptibility).19 21 Therefore, the objective of this study was to investigate to what extent stressful family conditions contribute to inequalities in child development and childhood education via differential exposure and susceptibility (figure 1).
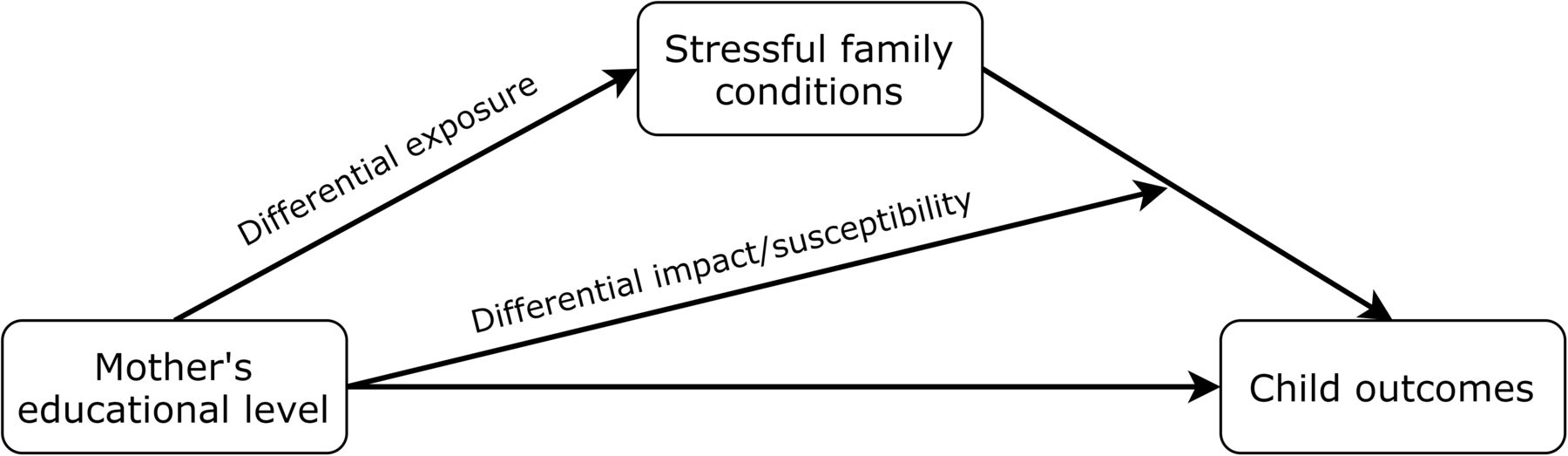
Conceptual model of the proposed processes of differential exposure and differential impact/susceptibility to stressful family conditions, leading to inequalities in child outcomes by mother’s education. Confounders are not included in the conceptual model.
Methods
Data
We used data from the Generation R Study, a multiethnic population-based cohort from foetal life onwards in Rotterdam, the Netherlands.22 During the inclusion period, all pregnant women residing in Rotterdam with an expected delivery date between April 2002 and January 2006 were invited to participate. Approximately 61% (N=9778) of women agreed to this. These women gave birth to 9749 live-born children. For 7893 children, consent was given for postnatal follow-up. We included all children who participated in the latest available assessment wave (around age 13 years; n=6842).
Measures
Self-reported mother’s highest educational attainment at child age 5 years was used as the exposure, categorised according to the International Standard Classification of Education (ISCED) as low (primary school or lower vocational education, ISCED 0–2), medium (intermediate vocational education, ISCED 3–4) or high (higher vocational education or university, ISCED 5–7).
All outcomes were measured at child age 13 years. Emotional and behavioural problems were child-reported using the validated Youth Self-Report, which consists of 112 items.23 For the main analysis, we used the total problem score, which includes both internalising and externalising behavioural problems (reverse coded). In addition, we ran two sensitivity analyses: (1) separately investigating internalising and externalising problem behaviour and (2) using the Child Behaviour Checklist (CBCL/6–18) as a measure of mother-reported emotional and behavioural problems.24 Cognitive development was measured using a subset of the Wechsler Intelligence Scale for Children-Fifth Edition, which provides a well-standardised assessment of individual cognitive functioning in 6–16 years olds25 and correlates 0.93 with the full-scale IQ. Secondary educational level was reported by the mother as the secondary school level that their child was currently attending and coded as a 10-point scale. We ran an additional sensitivity analysis using school performance assessed with the Dutch standardised end-of-primary-school test, created by the Central Institute for Test Development (www.cito.com).
All mediators (reflecting financial and social stress) were measured at child age 9 years to adhere to the temporal ordering assumed in mediation analysis. Three measures of financial stress were available to us, and were derived from a questionnaire filled in by the mother: (1) ‘Did you have any trouble paying for your food, rent, electricity bill and such in the past year?’ (answer categories were: (A) no, no trouble, (B) yes, a little trouble or (C) yes, a lot of trouble); (2) social security or unemployment benefits (no vs yes); (3) whether or not the household owned certain possessions or conducted certain activities, roughly corresponding with the material deprivation indicator used in EU-SILC.26 Positive answers were summed and reverse coded such that a higher score indicated less possessions/activities.
Two measures of social stress were included, corresponding to those included in the Family Stress Model: family functioning and maternal mental health. Family functioning was assessed by the General Functioning subscale of the Family Assessment Device,27 which is a validated 12-item measure of statements describing healthy and unhealthy family functioning. Maternal mental health was assessed using the 21-item short form of the Brief Symptom Inventory, which includes depression, hostility, anxiety and interpersonal sensitivity subscales.28
We constructed composite measures of stressful family conditions on the basis of confirmatory factor and reliability analyses (details described in online supplemental table S1). We used a composite measure of financial stress and a composite measure of social stress as our putative mediators. In addition, we constructed a measure of ‘total family stress’ by calculating the mean score of all financial and social stress items.
Supplemental material
Several covariates were included to adjust for possible confounding: child’s age at outcome measurement; child’s gender; child’s migration background (Dutch, Western or non-Western; using classifications provided by Statistics Netherlands); mother’s age at intake; and mother’s intelligence (assessed using the short form of the Raven’s Progressive Matrices29).
Statistical analysis
Descriptive statistics of the participants, stratified by mother’s educational attainment, were calculated to describe absolute group differences in the distribution of the outcomes and mediators. We fitted linear regression models to assess differential exposure and susceptibility.21 We used multiple imputations by chained equations (M=20) to impute missing data, except for mother’s educational attainment and the outcomes.
To assess to what extent differential exposure and susceptibility to financial stress and social stress in the family account for inequalities in child development in maternal education, we applied the four-way decomposition by VanderWeele.21 This method allows us to decompose the total effect of mother’s education on child development into four components of mediation and interaction: the effect of stressful family conditions on child development if mother’s education is necessary for stressful family conditions to be present (pure indirect effect (PIE); ie, due to mediation only), the combined effect of mother’s education and stressful family conditions on child development with mother’s education itself needed (mediated interaction (INTmed); i.e., due to both mediation and interaction) or not needed (reference interaction (INTref), ie, due to interaction only) for stressful family conditions to be present, and the effect of mother’s education on child development through pathways that do not require stressful family conditions (controlled direct effect (CDE); ie, neither due to mediation nor interaction).21 These components can be estimated on average for a population under the assumptions of no unmeasured confounding of the (1) exposure–outcome, (2) exposure–mediator and (3) mediator–outcome relationships and (4) that there are no mediator–outcome confounders that are themselves affected by the exposure.21
Following Diderichsen et al, we define differential exposure as the sum of the components PIE and INTmed, and differential impact/susceptibility as the sum of the components INTref and INTmed.19 In other words, we consider differential exposure as the extent to which the total effect of mother’s education on child development is due to unequal exposure to stressful family conditions and differential impact/susceptibility the extent to which the total effect of mother’s education on child development is due to interaction between mother’s education and stressful family conditions. To calculate these measures, we fitted linear regression models for the mediator and outcome, and combined the relevant estimates from the two regression models following the formulae provided by VanderWeele.21 We bootstrapped the estimates for differential exposure and susceptibility (1000 repetitions) to obtain 95% bias-corrected CIs.30 In addition, we calculated their relative contribution by dividing the estimate for differential exposure and differential impact/susceptibility by the total effect. All outcomes were standardised to aid comparisons between them. For the decomposition analyses, the mediators were fixed at their minimum level (ie, 0)—representative of an absence of financial or social stress—to ensure that the effect of the interaction between exposure and mediator was captured by the interaction component (and not the CDE).21 Estimates for each of the four components of the decomposition analysis are set out in online supplemental tables S2–S8, while estimates of differential exposure and susceptibility are set out in the manuscript.
Results
Over half (54%) of the children in our study had a highly educated mother, 30% had a mother with medium educational attainment and 16% had a mother with low educational attainment (online supplemental table S9). There was a gradient in maternal education in all (standardised) outcomes and mediators considered (online supplemental table S9).
Socioemotional development
The estimated total effect of maternal education on emotional and behavioural problems was −0.05 (95% CI −0.13 to 0.01) comparing medium versus high education, and −0.12 (95% CI −0.27 to 0.01) comparing low versus high education, after adjustment for confounders (table 1).
Estimated contribution of differential exposure and susceptibility to stressful family conditions on the total effect of maternal education on emotional and behavioural development of 13-year-old children
Differential exposure to financial stress caused a 0.03 SD worse (95% CI −0.04 to –0.01) emotional and behavioural problem score comparing medium versus high, and an 0.07 SD worse (95% CI −0.12 to –0.01) emotional and behavioural problem score comparing low versus high educational attainment. These estimates correspond to 53% and 54% of the total effect. Similar estimates were obtained for the separate internalising and externalising subscales, whereas even larger estimates were obtained using the CBCL (online supplemental tables S10–S12). Estimates for differential susceptibility to financial stress were lower and their CIs included the null (table 1).
Differential exposure to social stress accounted for 32% and 27% of the total effect of mother’s education on emotional and behavioural problems, comparing medium versus high and low versus high, respectively, while differential susceptibility to social stress did not contribute to this effect (table 1).
Cognitive development
The estimated total effect of maternal education on child intelligence score was −0.29 (95% CI −0.37 to –0.23) comparing medium versus high education, and −0.54 (95% CI −0.64 to –0.45) comparing low versus high education, after adjustment for confounders (table 2).
Estimated contribution of differential exposure and susceptibility to stressful family conditions on the total effect of maternal education on child intelligence of 13-year-old children
Differential exposure to financial stress caused a 0.02 SD lower (95% CI −0.03 to –0.01) intelligence score comparing medium versus high, and a 0.05 SD lower (95% CI −0.08 to –0.02) intelligence score comparing low versus high education. These estimates correspond to 7% and 9% of the total effect, respectively. The estimates for differential susceptibility were smaller and CIs included the null. For social stress, neither differential exposure nor susceptibility contributed to the effect of mother’s education on child intelligence score (table 2).
Childhood education
The estimated total effect of maternal education on her child’s secondary educational level was −0.47 (95% CI −0.54 to –0.40) comparing medium versuss high and −0.84 (95% CI −0.95 to –0.72) comparing low versus high, after adjusting for confounders (table 3).
Estimated contribution of differential exposure and susceptibility to stressful family conditions on the total effect of maternal education on secondary educational level of 13-year-old children
Differential exposure to financial stress accounted for 6% and 6% and differential susceptibility for 7% and 3% of the total effect, comparing medium versus high and low versus high education, respectively. Using the same educational contrasts, differential exposure to social stress accounted for 2% and 1%, and differential susceptibility for 6% and 1%, respectively, of the total effect (table 3).
Using school performance on the end-of-primary-school test as an outcome resulted in a slightly higher estimated contribution of differential exposure to financial stress (6% and 16%, respectively), but no contribution of differential susceptibility to financial or social stress (online supplemental table S13).
Discussion
The objective of this study was to investigate to what extent stressful family conditions contribute to inequalities in child development and childhood education by maternal education, as a potential result of (1) their uneven distribution across educational groups (ie, differential exposure) or (2) their detrimental effect being greater among children of less-educated mothers (ie, differential impact/susceptibility). Our results showed that differential exposure to financial or social stress in the family had a limited contribution to (the substantial) inequalities in intelligence score and secondary educational level, but a large contribution to (the modest) inequalities in emotional and behavioural problems (figure 2). Differential susceptibility to financial or social stress did not contribute to inequalities in any of the outcomes considered.

{kind=link}
{kind=link}
Contributions of differential exposure and susceptibility to financial stress (A) and social stress (B) to the effect of mother’s educational level (high vs low) on child development. Estimates for total effects, differential exposure and differential susceptibility were derived from four-way decomposition analyses. Estimates are expressed in number of SD. For example, differential exposure to financial stress caused a 0.07 lower SD socioemotional development score among children from less-educated mothers compared with children from more-educated mothers. Minor differences in total effect estimates occurred due to bootstrapping.
Before turning to the interpretation and implications of our results, some limitations need to be considered. Our analyses rest on assumptions about no confounding between exposure, mediators and outcomes.21 While we adjusted for several potential confounders based on previous research in this area, unmeasured confounding remains a possibility. This is perhaps most relevant for the estimated total effect of mother’s educational attainment on child’s secondary educational level, because similar determinants that affected the educational opportunities of mothers may also impact those of their children (eg, related to the educational system).3 Such unobserved confounding likely results in an overestimation of the total effect, but it is unclear in which direction this bias would have affected the estimated mediation effects. Furthermore, children of less-educated mothers are under-represented in the Generation R Study as compared with the general population, which likely caused an underestimation of the magnitude of the reported inequalities. Regarding the exposure–mediator relationship, potential biases are most likely to occur from unobserved confounding of childhood factors of the mother. For example, childhood mental health of the mother may have affected her educational attainment as well as some of the mediators (eg, adult mental health and unemployment). Similarly, confounding of child factors at an earlier age may have biased the mediator–outcome relationships. For example, a child’s emotional and behavioural problems at a younger age may negatively affect family functioning, which, in turn, may further increase child problems. These reinforcing mechanisms could not be adjusted for in our analyses, because it would take away part of the direct pathway from maternal education to child development, but not adjusting for it may have resulted in overestimations of the magnitude of the indirect pathways. Furthermore, we did not consider any temporal dependencies between the mediators, even though financial stress may also have an impact on parental mental health and family functioning,8 which would make financial strain an intermediate confounder in the mediation models on social stress. However, since the estimated mediation effects of social stress were much lower than those of financial stress, even without adjusting for the latter, we consider it unlikely that this had a substantial impact on our results.
Large inequalities in child development and childhood education have been reported across the globe, caused by an interrelated and complex web of factors at the family, neighbourhood, school and societal level.1 2 31 32 Evidence on the contribution of different causal pathways between social background and child development is crucial for identifying opportunities to tackle health inequalities early in life. In the context of these intermediate pathways, it is also important to assess the processes (ie, differential exposure and/or susceptibility) through which these mechanisms impact inequalities in child outcomes.1 19 At the family level, research has documented the relationship between material deprivation, poor parental mental health and poor family functioning, and worse developmental outcomes of children.33–36 Our study indicates that (1) inequalities by maternal education at age 13 years are particularly pronounced for cognitive development and childhood education, (2) financial and social stress in the family measured 4 years prior have a limited contribution to these inequalities in cognitive development and childhood education, but have a large contribution to—the much more modest—inequalities in socioemotional development and (3) this contribution is mainly due to the process of differential exposure. Future studies could adapt similar methods to support a stronger evidence base for tackling health inequalities.37
Why are stressful family conditions less relevant for explaining inequalities in cognitive and educational outcomes than for explaining inequalities in socioemotional development? One reason may be that the role of genetic determinants is perhaps stronger for cognitive development and educational attainment than for socioemotional development.38 39 However, by adjusting for mother’s intelligence we have tried to at least partly account for the intergenerational transmission of cognitive ability, which may be due to both genetic and environmental factors related to mother’s intelligence. Moreover, because genetic factors are not modifiable, they hold little relevance for informing public health policy. Another explanation may be that cognitive development and school results at age 13 years are more dependent on cognitive stimulation that also occurs outside of the family environment, while socioemotional development is much more dependent on family dynamics, in addition to school environment and peer-relationships. Especially in early adolescence, cognitive ability and educational progress are perhaps more dependent on contextual determinants at the school and peer level, such as school and classroom composition, and social connectedness. Finally, we assessed stressful family conditions at one particular point in time, and 4 years prior to the outcomes, which does not capture the cumulative effects of stress over a longer period or effects from stressful conditions that have occurred nearer in time to the outcome. Future research should consider to what extent these results are dependent on the time lapse between the (repeated) occurrence of stress and child development, and the cumulative effects of prolonged exposure to (periods of) stress.
In sum, our study found that higher exposure to stressful family conditions among children from less-educated mothers substantially contributes to inequalities in socioemotional development, but less so for cognitive development and educational attainment. Future research is needed to gain a better understanding of the mechanisms that account for these inequalities.
Ethics statements
Patient consent for publication
Ethics approval
The Rotterdam Study has been approved by the Medical Ethics Committee of the Erasmus MC (registration number MEC 02.1015) and by the Dutch Ministry of Health, Welfare and Sport (Population Screening Act WBO, licence number 1071272–159521PG). The Rotterdam Study Personal Registration Data collection is filed with the Erasmus MC Data Protection Officer under registration number EMC1712001. The Rotterdam Study has been entered into the Netherlands National Trial Register (NTR; www.trialregister.nl) and into the WHO International Clinical Trials Registry Platform (ICTRP; www.who.int/ictrp/network/primary/en/) under shared catalogue number NTR6831. All participants provided written informed consent to participate in the study and to have their information obtained from treating physicians. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Center in close collaboration with the Erasmus University Rotterdam, School of Law and Faculty of Social Sciences, the Municipal Health Service Rotterdam area, Rotterdam, the Rotterdam Homecare Foundation, Rotterdam, and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond (STAR), Rotterdam. We gratefully acknowledge the contribution of general practitioners, hospitals, midwives and pharmacies in Rotterdam.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors JOG, TH and FJVL conceived and designed the study, with input from PWJ, NH, MB and PvL. JOG conducted the analysis, with input from TH and FJVL. JOG wrote the first draft of the manuscript and acts as guarantor. All authors reviewed, edited and commented on multiple versions of the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was supported by a grant from the Netherlands Organization for Health Research and Development (ZonMw) (project No. 531003013). TH is financially supported by an NWO grant (grant number NWA.1238.18.001), and though a grant awarded by the Norwegian Research Council (project number 288638) to the Centre for Global Health Inequalities Research (CHAIN) at the Norwegian University for Science and Technology (NTNU). PWJ is member of the SEED Consortium. SEED stands for Social InEquality and its Effects on child Development: A study of birth cohorts in the UK, Germany and the Netherlands (Grant # 462-16-030) and is part of the Dynamics of inequality across the Lifecourse (DIAL) Programme of the EU’s New Opportunities for Research Funding Agency Co-operation in Europe (NORFACE) initiative.
Disclaimer The funders had no role in analysis or interpretation of data.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.