Article Text

Statistics from Altmetric.com
COVID-19 has disproportionally burdened racial and ethnic minority groups within the USA.1–5 However, prior studies relied predominately on aggregated data from populations residing in congregate and non-congregate settings.1–5 This approach may underestimate outcome disparities in the community, especially in states that experienced a large COVID-19 burden in nursing homes.5 Herein, we identified COVID-19-related deaths among Connecticut residents of congregate and non-congregate settings and characterised the evolution of racial and ethnic disparities in COVID-19-related mortality among residents of non-congregate settings.
We retrospectively identified COVID-19-related deaths reported between 1 March 2020 and 13 December 2021 from the Connecticut Electronic Disease Surveillance System and determined residential status according to recorded address (online supplemental file).5 Using Poisson regressions and 2019 census population estimates, we estimated age-adjusted mortality for composite race and ethnicity categories (Hispanic, non-Hispanic (NH) black and NH white) and age-adjusted mortality rate ratios (MRR) for Hispanic and NH blacks, relative to NH whites, for three periods (1 March 2020 to 25 August 2020, 26 August 2020 to 12 July 2021 and 13 July 2021 to 13 December 2021; figure 1C; online supplemental file).5
Supplemental material

{kind=link}
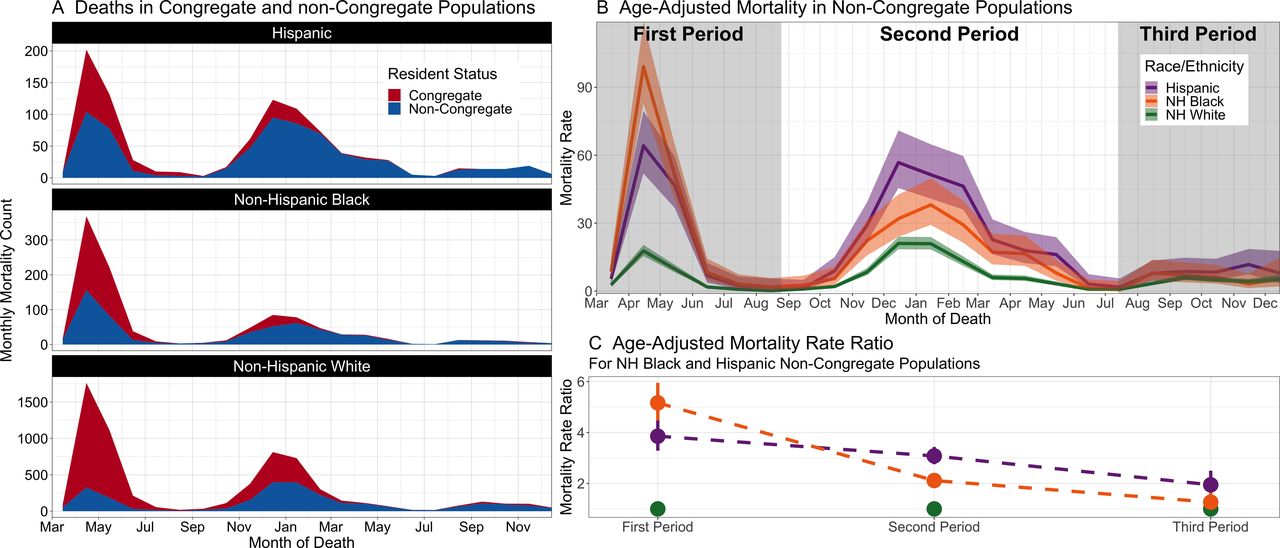
Temporal trends in COVID-19-related deaths and mortality among the Connecticut population residing in congregate and non-congregate settings, according to composite race and ethnic groups, March 2020 to December 2021. (A) Monthly COVID-19 deaths by race/ethnicity and residency status. (B) Age-adjusted monthly COVID-19 mortality (deaths per 100 000 population-months) by composite race and ethnic groups in the population residing in non-congregate settings. (C) Ratios comparing mortality among non-Hispanic black (NH black) and Hispanic to non-Hispanic white (NH white) populations residing in non-congregate settings during each of the three epidemic periods. Congregate and non-congregate residency status was defined based on recorded residential address at the SARS-CoV-2 infection was reported.
During the study period, congregate facility-associated deaths accounted for 74.6% (3205/4299), 37.7% (1341/3557) and 14.2% (84/590) of deaths in the first, second and third periods, respectively (figure 1A). Among congregate facility-associated deaths, 5.6% (259), 10.0% (463) and 84.4% (3908) were Hispanic, NH black and NH white, respectively.
Overall, age-adjusted mortality among residents of non-congregate settings was highest for Hispanics (19.6/100 000 population-months), followed by NH blacks (17.3/100 000 population-months) and NH whites (6.4/100 000 population-months). During the initial pandemic period, we observed large disparities in COVID-19 mortality within residents of non-congregate settings (Hispanic MRR: 3.9 (95% CI, 3.3 to 4.5); NH black MRR: 5.2 (CI: 4.5 to 5.9)). However, by the third wave, the disparities had attenuated and mortality between NH blacks and NH whites no longer differed significantly (Hispanic MRR: 1.9 (1.5 to 2.5); NH black MRR: 1.3 (0.9 to 1.7); figure 1B,C/online supplemental eTable).
Our findings suggest that attenuation of racial and ethnic disparities is an achievable public health goal. Future analyses investigating the role public health interventions had on reducing these disparities should be conducted to inform effective, generalisable policies targeting the outstanding inequities in COVID-19-related outcomes.
The limitations of our analysis include the use of a COVID-19-related death endpoint and the potential for misclassification of race, ethnicity and residency status. However, it was strengthened by the disaggregation of congregate facility events, through which we may have revealed levels of disparity not previously appreciated.1 2 4 5
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was not deemed as human research by the Yale University Institutional Review Board (IRB). All data were retrospective and per the requirements of the overseeing IRB, no retroactive consent was needed.
Acknowledgments
The authors thank Charles Powell for accessing the data and Matthew Cartter, Lynn Sosa and Karyn Backus for helpful comments on the manuscript.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
OS and MLL contributed equally.
Contributors OS and MLL had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: AIK, OS and DATC. Acquisition, analysis or interpretation of data: OS, MLL and JB. Drafting of the manuscript: MLL, OS, AIK and PS. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: MLL. Administrative, technical or material support: JB. Supervision: AIK and DATC.
Funding Connecticut Department of Public Health Emerging Infections Program: COVID-19 contract (DPH log # 2021-0071-3).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.