Article Text

Abstract
Background Intensive home visiting for adolescent mothers may help reduce health disparities. Given limited resources, such interventions need to be effectively targeted. We evaluated which mothers were enrolled in the Family Nurse Partnership (FNP), an intensive home-visiting service for first-time young mothers commissioned in >130 local authorities in England since 2007.
Methods We created a population-based cohort of first-time mothers aged 13–19 years giving birth in English National Health Service hospitals between 1 April 2010 and 31 March 2017, using administrative hospital data linked with FNP programme, educational and social care data. Mothers living in a local authority with an active FNP site were eligible. We described variation in enrolment rates across sites, and identified maternal and FNP site characteristics associated with enrolment.
Results Of 110 520 eligible mothers, 25 680 (23.2% (95% CI: 23.0% to 23.5%)) were enrolled. Enrolment rates varied substantially across 122 sites (range: 11%–68%), and areas with greater numbers of first-time adolescent mothers achieved lower enrolment rates. Mothers aged 13–15 years were most likely to be enrolled (52%). However, only 26% of adolescent mothers with markers of vulnerability (including living in the most deprived areas and ever having been looked after as a child) were enrolled.
Conclusion A substantial proportion of first-time adolescent mothers with vulnerability markers were not enrolled in FNP. Variation in enrolment across sites indicates insufficient commissioning of places that is not proportional to level of need, with mothers in areas with large numbers of other adolescent mothers least likely to receive support.
- ADOLESCENT
- CHILD HEALTH
- PUBLIC HEALTH
Data availability statement
Data may be obtained from a third party and are not publicly available. We are unable to share the individual data used for this study. HES and FNP data can be requested through NHS Digital, NPD data can be requested through the Department for Education.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Intensive home-visiting services (such as the Family Nurse Partnership (FNP)) have the potential to reduce adverse child outcomes associated with adolescent motherhood.
In England, the FNP is only offered to a subset of eligible pregnant adolescents.
There is a lack of evidence on the characteristics of mothers enrolling (and those who are not enrolled) in targeted interventions.
WHAT THIS STUDY ADDS
Using data from more than 100 000 first-time adolescent mothers in England, we showed that 23% of eligible mothers are enrolled in the FNP.
Lower enrolment rates were seen in areas with large populations of adolescent mothers; variation in enrolment rates across the country remained after adjusting for maternal risk factors in the eligible population.
Only half of mothers aged 13–15 years, 44% of those ever looked after by social care services and 40% of those with a history of mental health or adversity-related hospital admissions, were enrolled.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This research indicates a need for increased commissioning of targeted services relative to level of need in local areas.
Introduction
Children of adolescent mothers are more likely to experience adverse health outcomes than children of older mothers, partly due to socioeconomic disadvantage.1–3 Interventions aiming to reduce these inequalities include the Family Nurse Partnership (FNP), an intensive home-visiting programme supporting first-time mothers, has a strong evidence base from three US randomised trials and is recommended within the UK’s Healthy Child Programme.4 5 The FNP aims to improve birth outcomes, child health and development.6 Although a randomised trial in England found no evidence of benefit on outcomes including birth weight and hospital admissions before age 2 years, improved development and educational outcomes were reported, and there remains strong support for the programme locally.5 7–9
FNP has been commissioned in >130 English local authorities (LAs) since 2007. While eligibility criteria suggest all first-time adolescent mothers are eligible, the service has been rationed to ~25%–30% of adolescent mothers10 as sufficient funding for all was not made available. Effective targeting to those with highest need is therefore key for FNP service, with local teams encouraged to decide who to prioritise for enrolment. Evidence suggests that young mothers living in the most deprived areas, with histories of mental health conditions and prior contact with children’s social care are at higher risk of poor infant outcomes.11–13 However, little is known about the extent or drivers of variation in the targeting of intensive support to mothers in England.
To address this evidence gap and inform commissioning and targeting of the FNP, we quantified the variation in enrolment rates across 122 FNP sites in England and evaluated maternal vulnerability indicators and site characteristics associated with enrolment. We used population-based administrative data for all eligible mothers in England to generate evidence for decision-makers of targeted preventive services.
Methods
Data sources and linkage
The FNP enrolled first-time mothers aged <20 years at their last menstrual period, ≤28 weeks of pregnancy for most of our study period. From November 2016, a few FNP sites enabled enrolment after 28 weeks’ gestation, and among mothers aged 20–24 years with vulnerability markers.14
Using data in Hospital Episode Statistics (HES), we constructed a cohort of first-time mothers aged 13–19 years at last menstrual period, living in England, and giving birth in a National Health Service (NHS) hospital between 1 April 2010 and 31 March 2017.15 HES is an administrative database with coded information on all admissions to English NHS hospitals.16 Each care episode includes ≤20 clinical diagnosis codes from the International Classification of Diseases (ICD-10). Pseudonymised HESIDs link admissions for the same person over time. Information on Accidents & Emergency (A&E) attendance was obtained from the HES A&E dataset.
Records for enrolled FNP participants from the FNP Information System (IS) were linked to HES by a trusted third party (NHS Digital) using a deterministic linkage algorithm including name, NHS number, sex, date of birth and postcode. Of 27 065 FNP participants giving birth in our study period, 27 035 (99.9%) were linked to HES via the NHS Digital algorithm. Another 25 were linked manually based on dates of birth and delivery, birth weight, and LA, or through HES mother–baby linkage developed previously,15 leading to >99.9% linkage of FNP mothers to HES.
We used FNP IS data to determine enrolment dates by lower-tier LA, and validated site dates and catchment area with the FNP National Unit.
HES records for all mothers in our cohort were linked to the National Pupil Database (NPD) by a trusted third party (Department for Education), to enrich our dataset with information on maternal education (including Special Educational Needs status and receipt of free school meals) and contact with children’s social care services (including child protection plans and child looked after). A total of 83.5% of adolescent mothers in our cohort were linked to NPD.
Cohort definition
Our study cohort included all 110 520 eligible mothers aged 13–19 years with a first birth between 1 April 2010 and 31 March 2017, and whose first antenatal booking appointment as recorded in HES (or estimated date of 28 weeks’ gestation, if missing) occurred while there was an active FNP site in their LA of residence (figure 1). Date of last menstrual period was estimated by subtracting gestational age at birth from the date of childbirth, or subtracting 40 weeks (the median gestational age at birth among adolescent mothers) from the date of childbirth, for 13% of mothers with missing data. Mothers whose antenatal booking appointment occurred between 28 and 33 weeks’ gestation were excluded as they would not have met eligibility criteria (figure 1). (We may have excluded a small number of eligible mothers within the few sites that allowed enrolment >28 weeks from November 2016.) We considered recorded gestational age at booking appointment of ≥33 weeks among 6% of mothers to be data errors, and recoded them to 28 weeks to retain these mothers in the cohort. We excluded mothers whose pregnancy ended in stillbirth and those enrolled in FNP for their second delivery (eg, following a previous stillbirth) to ensure comparability with unenrolled mothers. Ten FNP mothers who did not link to HES, and 90 who linked to an HESID with no inpatient hospital records, were also excluded.

Flow diagram of cohort selection. Ninety mothers who linked to an HESID that contained no inpatient hospital records (eg, due to home delivery), and only A&E attendance records, were excluded from our cohort. Numbers have been rounded to the nearest 5 in accordance with NHS Digital’s statistical disclosure rules for subnational analyses; totals may not be equal to the sum of component categories. ‘First-time mothers’ refers to first live birth; mothers may have had a previous pregnancy ending in miscarriage or abortion (in line with FNP eligibility criteria). A&E, Accidents & Emergency; ANC, antenatal care; FNP, Family Nurse Partnership; HES, Hospital Episode Statistics; LA, local authority; LMP, last menstrual period; NHS, National Health Service.
Outcome
Our outcome of interest was enrolment in FNP, as identified by linkage of a mother in FNP IS to a record in HES, regardless of the number of FNP visits received.
Maternal risk factors
We selected potential risk factors for FNP enrolment based on maternal vulnerability characteristics associated with poor infant outcomes, and available in HES: maternal age, ethnicity and area-level deprivation (Index of Multiple Deprivation quintile).11 We also considered maternal unplanned hospital admissions within 2 years prior to 20 weeks’ gestation: mental health-related admissions (excluding self-harm and substance misuse), adversity-related admissions (violence, self-harm or substance misuse) and chronic condition admissions were identified based on published lists of ICD-10 diagnostic codes (online supplemental table 1).11 17–19 Having ≥1 A&E attendance within 2 years prior to 20 weeks’ gestation was also considered as a risk factor. We considered educational and social care characteristics before 20 weeks of pregnancy, including ever having a child protection plan or being looked after, having Special Educational Needs, receiving free school meals, living in the Income Deprivation Affecting Children Index (IDACI) bottom decile, school exclusion/pupil referral unit/alternative provision, and persistent absence. We also considered Key Stage 4 educational attainment.
We used 20 weeks’ gestation since 93% of all mothers attend an antenatal booking appointment by this stage.20 We defined vulnerability markers as maternal age 13–15 years, living in the most deprived quintile, ever having Special Educational Needs, ever being looked after or having a child protection plan, and previous mental health-related or adversity-related admission.
Site characteristics
FNP sites consist of a team covering one or more (neighbouring) LAs. We classified sites into enrolment rate quartiles (‘high-enrolment sites’ as those in the highest quartile and ‘low-enrolment sites’ in the lowest quartile), and examined variation in enrolment according to enrolment quartile, geographical region, and year. We hypothesised low-enrolment sites would show more selective targeting of vulnerable mothers, and provide insight into prioritisation of mothers when resources are limited.
Data analysis
We calculated enrolment rates as the percentage of FNP participants among eligible first-time adolescent mothers living in an LA with an active FNP site at the time of first antenatal appointment, including by site and maternal risk factors. Multilevel logistic regression models with mothers nested within FNP sites were used to calculate crude and adjusted ORs of enrolment. Multivariable models included all maternal risk factors; multicollinearity was assessed using Spearman correlation coefficients. To examine variation in maternal risk factors, we stratified the analysis by site characteristics: high/low-enrolment site, region and financial year of delivery, and tested for interaction with maternal risk factors. We explicitly classified mothers not linking to NPD as ‘unlinked’ in relevant variables to retain them in models.
Lastly, we built crude and adjusted funnel plots of enrolment rates by site according to the size of the eligible adolescent mother population, separately for ages 13–17 and 18–20 years at childbirth, to assess whether variation in enrolment rates was likely due to chance. The outer limits on the plots define the range of percentages that are within three SDs of the national average. If the observed variation was due to chance alone, we would expect only 1 in 500 sites to have a percentage that is outside these limits.
Secondary analysis
We repeated the analysis for first-time mothers aged 20–24 years at last menstrual period in relevant FNP sites (detailed methods in online supplemental material 2).
Results
Description of enrolment
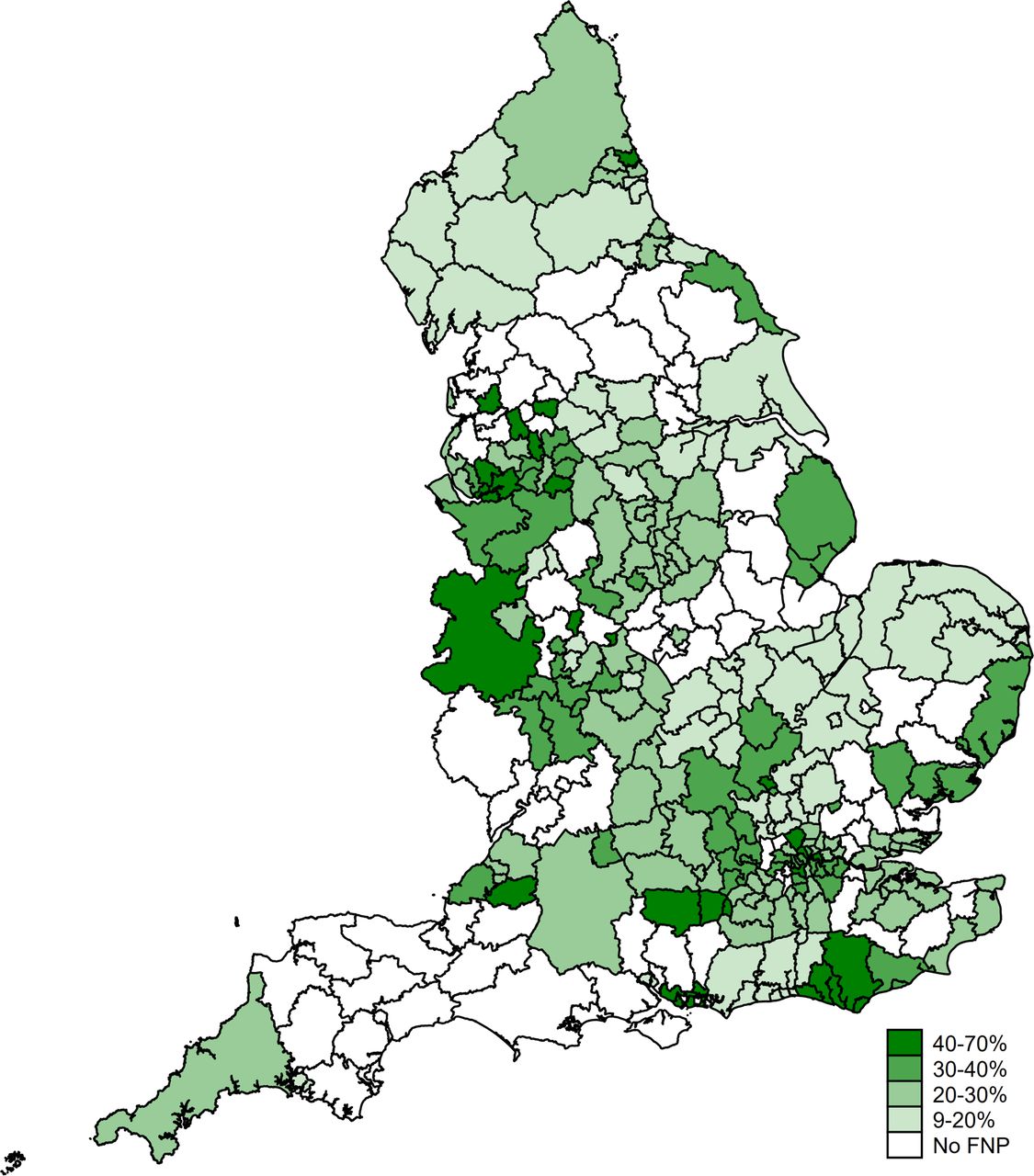
Among all 110 520 eligible adolescent mothers giving birth between April 2010 and March 2017, 25 680 (23.2% (95% CI: 23.0% to 23.5%)) were enrolled in FNP. Enrolment rates ranged across 122 FNP sites from 11% in Cumbria to 68% in Wandsworth (figure 2). Online supplemental table 2 describes the 136 LAs, enrolment dates and rates by FNP site.
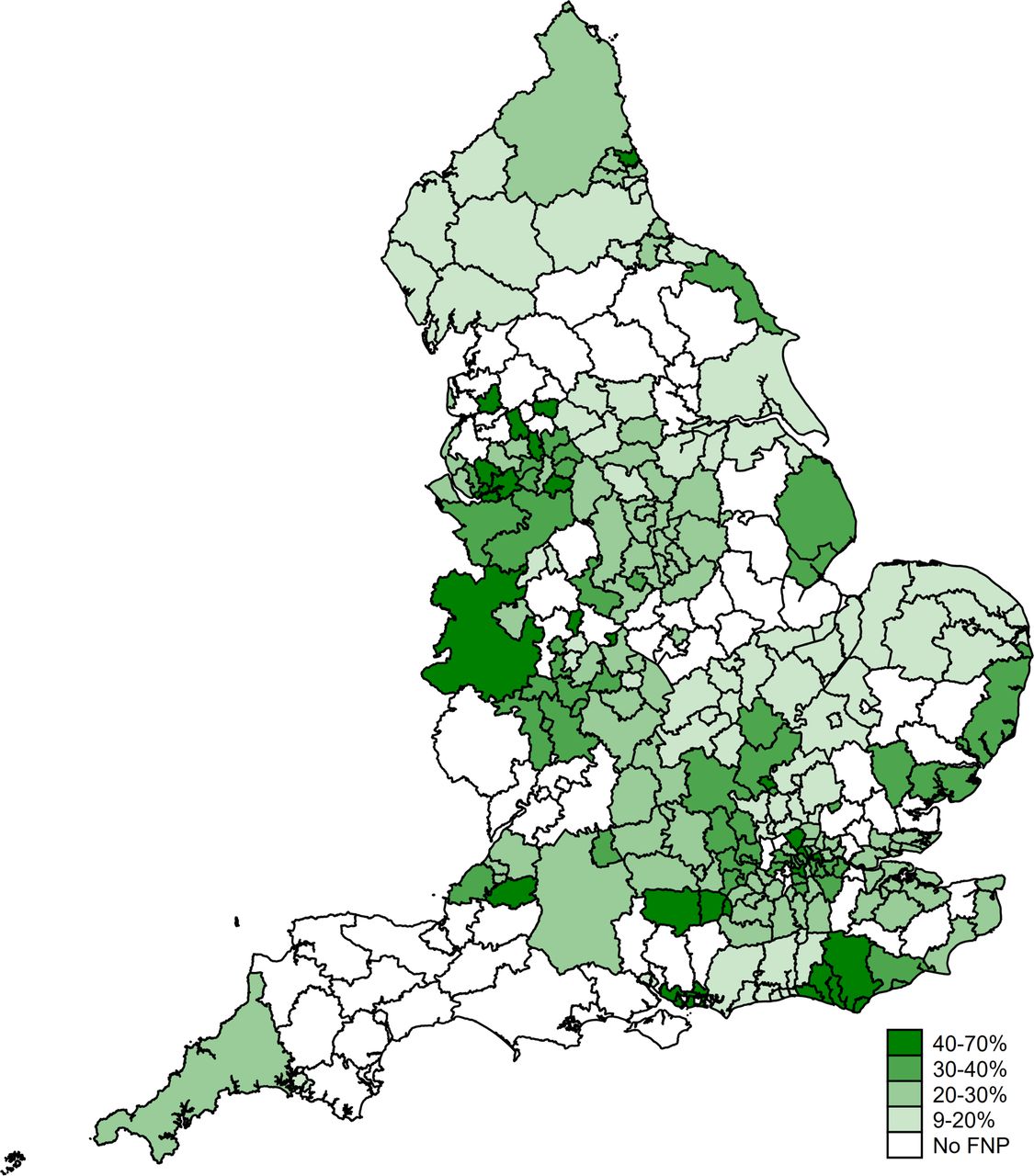
Percentage enrolment in the Family Nurse Partnership (FNP) among eligible adolescent mothers, living in a local authority (LA) with an active FNP site at the time of first antenatal appointment, by Local Authority–England, births between 1 April 2010 and 31 March 2017. The 122 FNP sites active during the study period covered 136 LAs (numbers and geographical boundaries of sites and LAs changed over the study period). Different sites were active for different periods within the 2010–2017 cohort; the FNP was never commissioned in 15 LAs (online supplemental figure 1).
Overall, 12.5% (12.4%–12.7%) of all (25 680 of 204 690) first-time adolescent mothers giving birth in England in our study period were enrolled in FNP.
Risk factors for enrolment
Most eligible first-time adolescent mothers were white (85%), aged 18–19 years at childbirth (55%) and living in the most deprived quintile (49%) (table 1). Five per cent of first-time adolescent mothers had ever been looked after before 20 weeks of pregnancy, 32% had ever been absent ≥10% school half-days within a term and 63% had attempted but not achieved 5 A*-C GCSEs. Characteristics of eligible mothers were similar to LAs having never commissioned FNP (online supplemental table 3). Overall, 52% of eligible adolescent mothers had at least one vulnerability marker.
Risk factors for FNP enrolment among mothers aged 13–19 years at last menstrual period, living in a local authority with an active FNP site at the time of first antenatal appointment (England, births between April 2010 and March 2017)
The enrolment rate was highest (52%) among those aged 13–15 years than 20 years at childbirth (12%), although those aged 13–15 years old accounted for only 2% of eligible mothers (table 1). The enrolment rate increased slightly from 21% in the least deprived quintile to 24% in the most deprived. A total of 40% of adolescent mothers with previous mental health or adversity-related admissions were enrolled, as well as 44% of mothers ever looked after and 29% of those ever identified as having Special Educational Needs. Overall, 26% of adolescent mothers with any vulnerability marker were enrolled.
Results from the adjusted model (table 1) showed younger mothers were prioritised for enrolment (the OR decreased from 2.65 (95% CI: 2.39 to 2.94) in mothers aged 13–15 years old to 0.56 (0.53 to 0.59) in mothers aged 20 years, compared with those aged 18–19 years old). Other important risk factors for enrolment included ever having been a child looked after (OR=1.92 (1.81 to 2.04)), ever had a child protection plan (OR=1.62 (1.46 to 1.80)) or ever having been identified as having Special Educational Needs (OR=1.22 (1.18 to 1.27)).
Variation in maternal risk factors according to site characteristics
Low-enrolment FNP sites included 51% of all eligible mothers in their catchment areas but enrolled ≤21% of these mothers, while high-enrolment sites included only 9% of all eligible mothers and had rates >36% (online supplemental table 4).
The effect of age and ethnicity on enrolment was more pronounced in low-enrolment sites (online supplemental table 5) and varied across regions (online supplemental figure 2, online supplemental table 6). The age gradient appeared in all regions, but was particularly pronounced in the South-West, East Midlands and South-East. In five of nine regions, mothers living in the most deprived areas were more likely to be enrolled than those in the middle quintile of deprivation. Only in London was enrolment higher in the least deprived areas (OR=1.68 (1.08 to 2.63), compared with the middle quintile).
Risk factors for enrolment also varied over time (online supplemental table 7), partly due to changes in regional distribution of active sites.
Funnel plots of variation in enrolment rates
A substantial proportion of FNP sites’ enrolment rates fell outside the funnel plot limits, indicating that much of the variation in enrolment rates across sites for younger mothers (aged 13–17 years at childbirth) was unexplained by chance (figure 3). There was even more unexplained variation among mothers aged 18–20 years at childbirth, as indicated by the majority of FNP sites falling outside the funnel plot limits. Among both age groups, adjusted enrolment rates were lower than expected in sites with larger numbers of eligible adolescent mothers (online supplemental figure 3).

{kind=link}
{kind=link}
{kind=link}
Unadjusted funnel plots of variation in FNP enrolment rates among eligible first-time adolescent mothers across FNP sites, by maternal age–England, births between April 2010 and March 2017. FNP, Family Nurse Partnership.
Secondary analysis: enrolment among mothers aged 20–24 years
In FNP sites enrolling mothers aged 20–24 years at last menstrual period, the enrolment rate was 3.7% (165 of 4470; 3.1%–4.2%), varying between 2% and 11% across sites. Mothers who were ever looked after, recorded as receiving free school meals or having Special Educational Needs were more likely to be enrolled (online supplemental material 2).
Discussion
Our study fills an important evidence gap on coverage and targeting of intensive home-visiting services such as FNP within England. We show the most vulnerable mothers are being targeted for FNP, especially the youngest teenagers, and those with prior contact with children’s social care. However, despite all first-time adolescent mothers living in FNP catchment areas being eligible for the programme, only 23% were enrolled between 2010/2011 and 2016/2017. Our findings indicate insufficient commissioning of FNP relative to need: areas with the greatest numbers of adolescent mothers had lower enrolment rates, and variation in enrolment rates remained after adjusting for known differences in maternal risk factors. Overall, only 26% of eligible adolescent mothers with vulnerability markers associated with adverse outcomes were enrolled, including 52% of those aged 13–15 years, 44% of those ever looked after, and 40% of those with prior mental health or adversity-related hospital admissions. These groups represent mothers and infants at significantly greater risk of low birth weight, unplanned hospital admissions for injury and infant mortality.11 Moreover, adolescent mothers had similar risks of young maternal age and having been looked after in areas where FNP was never commissioned, and where similar intensive support is not available.
A major strength of our study was the use of a population-based cohort of all first-time adolescent mothers giving birth in English NHS hospitals, linked to routine education and social care records, and >99.9% ascertainment of FNP mothers in HES. We used extensive data quality checks for LA-specific site activity dates and geographical coverage with the FNP National Unit to minimise misclassification of unenrolled eligible mothers. However, complex site histories (including different local areas within sites being commissioned at different times) mean we may have overestimated unenrolled eligible mothers and therefore underestimated some enrolment rates. Conversely, birth ascertainment in HES (97% of total births in English hospitals according to the Office for National Statistics)15 means some mothers may have been wrongly excluded from the denominator. Neither underascertainment nor overascertainment of unenrolled eligible mothers is likely to have biased the risk factor analysis, since they should not be associated with risk factors.
Some data limitations are worth noting. First, missing data on gestational age at booking appointment (32%) and birth (13%) required us to make assumptions to determine eligibility. Some mothers with missing gestational age at first antenatal appointment may have booked after 28 weeks but were retained in our cohort (2.6% were excluded due to known booking appointment after 28 weeks, vs 7% expected based on primary care records—S Syed, personal communication). Second, the NPD does not identify mothers who had contact with social services only before starting school, likely underestimating history of social care and effect estimates. The administrative data we used did not capture information on all relevant maternal characteristics or service contacts (eg, community mental health service use). Linkage to primary care and the Maternity Services Dataset could enable investigation of a wider range of risk factors. Given limited resources, individual-level or household-level deprivation measures (including those available through Unique Property Reference Numbers) could allow for more effective targeting and follow-up of the many young mothers experiencing socioeconomic disadvantage.21
To our knowledge, this is the first study examining enrolment in a targeted intensive home-visiting programme for expectant mothers. Similar to our findings, two previous studies have shown high variation in acceptance rates for universal home visiting between sites, and higher acceptance rates among higher-risk mothers.22 23 In a similar targeted home-visiting intervention for vulnerable families in Canada, unenrolled mothers were more vulnerable than enrolled mothers—contrary to our findings—nonetheless illustrating similar difficulties in enrolling the most vulnerable groups.24
Budget cuts since the inception of the FNP in England in 2007 mean that the programme, costing approximately £3000 per client per year, has been offered to a more select group of mothers over time.25 26 Our study demonstrates FNP places are not commissioned proportionately to the level of need within local areas, with particularly insufficient commissioning in LAs with higher numbers of adolescent births, contrary to stated aims of prioritising ‘areas with […]the highest numbers of eligible population’.27 Pregnant adolescents living in areas with many adolescent mothers are less likely to receive support than those in areas with few adolescent mothers, with important implications for equity. Commissioning an intensive service for only some eligible mothers has potential knock-on effects on those unenrolled, that is, if most adolescent mothers are assumed to be receiving additional support.
Young age is the main eligibility criterion for FNP in England, based on ease of identification, associations with social adversity, disrupted education and employment,2 28 and other factors contributing to poor health outcomes among their children.29–31 However, only half of mothers aged 13–15 years were enrolled in FNP. Furthermore, other countries additionally focus on low educational level or unemployment,32–34 based on evidence of higher effectiveness in socioeconomically deprived groups in the USA.35–37 Given strict caseload limits (maximum 25 mothers per family nurse), many sites in England have explicit policies of prioritising younger adolescent mothers. Overall, 74% of mothers with vulnerability markers were not enrolled in FNP, reflecting a failure of policy and commissioning to address vulnerable mothers’ needs, with important variation in who is offered intensive services across England.
There are several explanations and implications of this. First, identifying vulnerable mothers may be challenging, due to limited and variable information on vulnerabilities available to referring health providers and FNP teams. Although FNP teams may prioritise mothers with additional vulnerabilities not captured in administrative data we used (homelessness or community mental health service use), we show that only 44% of mothers looked after as children were enrolled. Some vulnerabilities (such as family violence) may be disclosed only after a trusting relationship is built with their family nurse or health visitor,38–40 underscoring the need for effective universal services. Second, there is uncertainty regarding which vulnerable mothers are likely to accept and benefit from intensive support. Ongoing evaluations of the FNP will determine which subgroups of young mothers benefit the most from FNP and inform decisions by referring clinicians.41 Given insufficient funding for universal offer, family nurses and referring providers need standardised, real-time information on vulnerabilities for all mothers to support decision-making and better target the FNP. Work on defining vulnerabilities by the FNP National Unit will support sites to determine priority criteria for their local context.
Third, vulnerable mothers may have higher refusal rates. FNP’s fidelity target is to enrol 75% of mothers offered FNP; aggregate site data suggest not all sites meet this target. We were unable to determine whether under-representation of some groups, for example, South Asian adolescent mothers, was because they were less likely to be offered a place, accept it or both. FNP teams report most mothers who decline feel socially well supported, although some decliners are especially vulnerable (eg, involved with social care services).42 Last, more vulnerable mothers may be unknown to midwifery services, due to enrolling after 28 weeks (eg, due to moving between LAs in pregnancy). Individual-level information on who is approached and who accepts would help inform strategies to increase uptake among especially vulnerable mothers.
To successfully reduce social inequalities, interventions need to be commissioned for all families with higher need. In 2010–2017, most adolescent mothers at highest risk of adverse outcomes were not receiving intensive support during and after pregnancy. Due to variation in service delivery across England, eligible adolescent mothers living in areas with many adolescent mothers were least likely to receive FNP support. Moreover, adolescent mothers with similar vulnerabilities had no access to equivalent support in areas where FNP was not commissioned. Commissioning should aim to provide adequate support to meet the needs of all adolescent mothers (not just a subset of them), through increased provision of intensive services in line with local need, including for mothers not eligible for FNP. With limited resources and pressure on health visiting services, decisions about the appropriate level of care for each family should be based on continuous evaluations of who is most likely to benefit, supported by more complete recording of vulnerabilities antenatally and real-time linkage of routine health and social care data.11 43
Data availability statement
Data may be obtained from a third party and are not publicly available. We are unable to share the individual data used for this study. HES and FNP data can be requested through NHS Digital, NPD data can be requested through the Department for Education.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and approval for the protocol41 was obtained from Nottingham Research Ethics Committee (ref 18/EM/0014), the Department for Education (ref DR190430.02) and the Confidentiality Advisory Group (ref 18/CAG/0013). This study used de-identified administrative data, and therefore it was not possible for us to contact participants to request consent.
Acknowledgments
We are grateful to Sue Hillsden from the FNP National Unit for her help identifying catchment areas and activity dates for FNP sites. We thank Nicole Hobson from the FNP National Unit, as well as Debbie Bougard, Karen Arkle, Caroline Scott, Mel Green, Lydia Ottavio, Catherine Dent, Charde Thompson, Anna Parry and Kristin Vreugdenhil from FNP teams for their help with understanding referral processes and sharing aggregate enrolment data from their sites.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @CescaCava, @epi_counts, @andreeacali
Contributors KH, the guarantor, designed the study, with input from RG, EK, EH, SK and JvdM. KH, FLC and LPMMW acquired the data for analysis. FLC and KH conducted the analyses. FLC wrote the first draft of the manuscript with KH. All authors, including MAC and LR, contributed to the interpretation of results and writing of the manuscript.
Funding This work was funded by the NIHR Health Services Research and Delivery panel (17/99/19). This research was supported in part by the NIHR Great Ormond Street Hospital Biomedical Research Centre. KH is funded in part by the Wellcome Trust (212953/Z/18/Z). RG is funded in part through the NIHR Children and Families Policy Research Unit and Senior Investigator Award, and the Health Data Research UK (grant no. LOND1), which is funded by the UK Medical Research Council and eight other funders.
Disclaimer The views expressed in this article are those of the author(s) and are not necessarily those of the NIHR or the Department of Health and Social Care.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests LR is the National Lead for Family Nurse Partnership (FNP) and Parenting Programmes, and MAC Head of Data and Analysis for the FNP National Unit.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.