Article Text

Abstract
Background Mental disorders are a major cause of work disability among the working-age population. Psychotherapy has shown to be an effective treatment for mental disorders, but the evidence is mainly based on small-scale randomised trials with relatively short follow-ups. We used population-based register data to examine the association between statutory rehabilitative psychotherapy and change in depression or anxiety-related work disability.
Methods We drew a nationally representative sample of the working-age population (aged 18–55 in 2010). The study group comprised all those who started rehabilitative psychotherapy in 2011–2014. A total of 10 436 participants who were followed from 3 years prior to 4 years after the onset of rehabilitative psychotherapy. This resulted in 83 488 observations. The annual total number of mental health-related work disability months (0 to 12) was calculated from the total number of annual compensated sickness absence and disability pension days. A quasi-experimental interrupted time series analysis was applied.
Results The onset of rehabilitative psychotherapy marked a decline in work disability in comparison to the counterfactual trend. Specifically, a 20% decrease in the level (incidence rate ratio, IRR 0.80; 95% CI 0.76 to 0.85) and a 48% decrease in the slope (IRR 0.52; 95% CI 0.50 to 0.54) of work disability were detected in comparison to the counterfactual scenario. No significant gender differences were observed. The decline in work disability was the steepest in the oldest age group.
Conclusions This study suggests that statutory psychotherapy may decrease work disability at the population level. However, further evidence of causal inference and the potential heterogeneity of the association is required.
- MENTAL HEALTH
- PUBLIC HEALTH
- SICK LEAVE
- RECORD LINKAGE
Data availability statement
No data are available. No additional data are available because of Finnish legislation. Only researchers with the permission of the Finnish Social and Health Data Permit Authority and Statistics Finland have access to the analysed data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Mental health issues are a major public health concern. Depression (and related anxiety) is among the leading causes of disability globally. Preventive measures need to be taken, but at present also providing evidence-based, accessible treatment and mental health services is essential. There is a need for longitudinal studies on psychotherapy outside controlled trials and in population-based samples.
WHAT THIS STUDY ADDS
We found that attending rehabilitative psychotherapy marked a decline in depression-related or anxiety-related work disability. The observed association was strongest in the oldest age group.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study suggests that providing statutory psychotherapy may decrease work disability at the population level.
Introduction
Mental disorders are highly prevalent among the working-age population, and they result in extensive disability costs for both individuals and society. In countries belonging to The Organisation for Economic Co-operation and Development, mental disorders account for 30–50% of all long-term sickness and disability in the working-age population.1 Work disability due to mental disorders has risen considerably in recent years in Finland, particularly in young age groups, and the prevention of disability retirement has been a priority on the Finnish public health agenda.2 3 In 2021, 36% of all compensated sickness absence (SA) days were due to mental disorders. Among those aged 20–29, mental disorders contributed to 64% of all compensated SA days in 2021. In the same year, of all disability pensions (DPs) in Finland, 33% were granted due to mental disorders. Among those aged under 35, 83% of DPs were granted due to mental disorders.4 5
Psychotherapy has been defined as a goal-directed professional activity in the healthcare sector, which aims to improve patients’ psychological health and functional capacity.6 This activity is guided by law, professional practices and ethical principles. Psychotherapy aims to eliminate or alleviate mental illnesses and emotional pain, increase the quality of life, support an individual’s psychological development and provide tools for tackling mental disorders. Mental disorders are often associated with deficient functional capacity and work ability.7–9
Psychotherapy is one form of rehabilitation provided by The Social Insurance Institution of Finland (SII). Rehabilitative psychotherapy is partly state subsidised and has been statutory since 2011. The most common approaches in subsidised rehabilitative psychotherapy in Finland include psychodynamic, cognitive, cognitive-behavioural and cognitive analytic, solution-focused and integrative psychotherapy in individual, group, couple and family settings.
Rehabilitative psychotherapy aims to support an individual’s employment, staying at work and return to work, but it is not linked to occupational health services (OHS) or other employer measures aiming to maintain employees’ work ability. The SII can compensate rehabilitative psychotherapy for 1 to 3 years with a maximum of 80 appointments per year and 200 appointments in 3 years. The applicant must be aged 16–67 and have a diagnosed mental health problem that threatens work ability (or ability to study). The need for and suitability of the individual for psychotherapy is evaluated by a psychiatrist.
Psychotherapy does not suit everyone and may have side effects, such as obtaining no results or obtaining different, unwanted results or even deterioration of the illness. It has been argued that sometimes it may be difficult to tell these outcomes apart and it may be unclear what is harmful and what is not.10–12 Heterogeneity in the effects of psychotherapy is also recognised.13 Numerous factors related to, for example, the characteristics of the patient or the therapist, and social context may modify the effects.
According to meta-analyses, psychotherapy can have positive, short-term effects on depression in adult age groups when compared with typical outpatient care.14 15 Positive effects have also been found in connection with anxiety disorders.16 However, some meta-analyses have detected various methodological challenges such as heterogeneity between different studies and low quality of the studies.17–19 Most of this evidence stem from small-scale randomised trials with relatively short follow-ups. There is a need for longitudinal studies on psychotherapy in a ‘real-world study setting’ (ie, outside controlled trials) and in population-based samples. In this register-based study, we investigated the change in the annual total number of health-related work disability months before and after the onset of rehabilitative psychotherapy, using a quasi-experimental design and comprehensive population-based register data. To examine heterogeneity, the effects were studied separately for women and men and for different age groups.
Methods
Study context
In Finland, all non-retired residents aged 16–67 are eligible for compensation for absence from work due to their own illness. When employment has lasted for at least 1 month, in cases of work disability due to illness, the employer continues to pay the employee full salary from the day on which the illness begins plus the following 9 week days. According to collective labour unions’ negotiated agreements, many employers continue to pay a full salary for the first months. After this, the SII starts paying statutory sickness benefit, which progressively compensates lost wage income. Employers are obligated to inform OHS when an employee has been absent from work for 30 calendar days.20 When sick leave has lasted for 60 days, the employer must apply for sickness benefit from the SII and OHS must evaluate the employee’s potential need for rehabilitation. When sickness benefit has been paid for a total of 90 days, OHS evaluates the work ability of the employee and negotiates the options of return to work together with the employee and employer. The maximum length of SA compensation is 300 working days per disease in 2 years. When work ability has been reduced for at least 1 year, the pension provider compensates for the loss of income with a DP. A DP can be granted either temporarily or permanently.
Study design and population
The data were obtained from a population database maintained by Statistics Finland. All Finnish residents are registered under a personal identification number in this database. This number is assigned to each citizen of Finland at birth and to immigrants when they obtain a residence permit and are common to all administrative registers, enabling extensive record linkages.21
From these data, a 33% random sample of the working-age population (aged 18–55 in the census year 2010 and, thus, of working age until the end of the follow-up in 2019) was drawn by Statistics Finland (n=7 71 540). Total population sampling was not feasible for data security reasons. The study group comprised all those who started compensated rehabilitative psychotherapy according to the SII registers (at t0, the onset of psychotherapy in 2011–2014). All those who died during the follow-up or were on DP at t0 were excluded (n=4971). The final study group included 10 436 participants. These participants were followed from 3 years prior (t-3) to 4 years after the onset of rehabilitative psychotherapy (t+4). Although the treatment could have ended at any point during the follow-up, most individuals received around 3 years of treatment.
Sociodemographic background information on the participants was drawn from the registers of Statistics Finland. Information on all sick leave periods lasting more than 11 calendar days (start and end dates and diagnostic codes (ICD-10)) was derived from the national sickness insurance register of the SII. Corresponding information on DPs was obtained from the Finnish Centre for Pensions. Annual data on the purchases of prescribed psychotropic medication were obtained from the Prescription Register (from the SII). Data from these various national registers were linked on the basis of the participant’s personal identification numbers. We analysed the individual-level register-based data of all the participants in the sample. The study followed the Rise of Mental Vulnerability in Work Life study plan, which is in line with EU and Finnish data legislation.
Outcome
The annual total number of mental health-related work disability months (0 to 12) was calculated on the basis of the total number of annual compensated SA and DP days in the diagnostic categories of depression (ICD-10 F32–33) and anxiety (F40–43). Part-time DP days were converted into whole days, so that two part-time DP days counted as one whole day. Following Hiilamo et al,22 work disability days were converted into months: no work disability months for ≤7 annual work disability days; 1 month for 8–29 days; 2 months for 30–59 days and so forth.
Statistical analyses
Our study was a retrospective secular trend study, and we used an interrupted time series (ITS) analysis to investigate the change in the annual total number of mental health-related work disability months before and after the onset of rehabilitative psychotherapy. To account for clustering of repeated measures within individuals, we used Poisson regression generalised estimating equation (GEE) with robust SE calculations. The most appropriate correlation structure was selected by comparing quasi-information criterion (QIC) values for independence with exchangeable, and first-order autoregressive correlation structures. The exchangeable correlation had the lowest QIC value and, therefore, had the best fit with the data. The Poisson GEE regression models with exchangeable correlation structures and robust SE calculations were used to assess the immediate change in the level and the gradual change in the slope of mental health-related work disability, estimated as incidence rate ratios (IRR) with 95% CIs. In this study, IRR compared the incidence rates of two time points, a rate ratio of >1 indicating an increased risk and a rate ratio of <1 a decreased risk in comparison to the intercept (t0). We analysed the outcome data 3 years before and 4 years after the onset of therapy. We first fit the crude model and then adjusted for observed time-varying covariates expected to confound the main association of interest.
Heterogeneous effects were examined in gender-stratified and age-stratified groups. We used R V.4.0.5 and the package geepack23 for the analyses.
An ITS design involves the collection of outcome data at multiple time points before and after an intervention (ie, the onset of rehabilitative psychotherapy). The preintervention outcome data are used to establish an underlying trend that is assumed would continue unchanged in the absence of the intervention under study (ie, the extrapolated counterfactual trend). Any change in outcome level or trend from the counterfactual scenario in the postintervention period is then attributed to the impact of the intervention.24 25 In comparison with simple pre–post designs in which the average outcome level is compared between preintervention and postintervention periods, the key advantage of an ITS design is that it evaluates the intervention effect while accounting for preintervention trends. In addition, ITS designs can increase power by making full use of longitudinal data instead of collapsing all the data into single preintervention and postintervention time points.24 The use of longitudinal data can also be helpful for assessing whether intervention effects are short lived or sustained over time.
A strength of ITS studies is that they are generally unaffected by typical confounding variables, which remain rather constant, such as population age distribution or socioeconomic status. Nevertheless, ITS can be affected by time-varying confounders, which change more rapidly. Known and measured time-varying confounders can be controlled for in the statistical model. In addition to age, gender and education, we adjusted for time-varying covariates. These were employment status (categorised as employed, unemployed, student, outside the workforce for other reasons) and compensated purchases of psychotropic medication (Anatomic Therapeutic Chemical, ATC, classification N06 or N05 categorised as 0=no, 1=yes).
Results
Table 1 shows the descriptive statistics of the participants, of whom 76% were women. The mean age of all the participants was 35, 72% had secondary or higher education and 9% had purchased prescribed psychotropic medication during the onset year of their rehabilitative psychotherapy. A crude estimate for the duration of psychotherapy was calculated on the basis of the information on annual statutory reimbursement for therapy. The mean duration of psychotherapy was 3.01 years (SD=1.01). Duration was slightly longer among women (mean=3.11, SD=1.01) than men (mean=3.00, SD=1.10, p<0.001).
Descriptive statistics of participants (n=10 436)
Tables 2 and 3 and figures 1 and 2 (crude models) show the results of the ITS analysis. The IRR estimates presented in table 2 indicate an increasing trend of depression-related or anxiety-related work disability during the preintervention period until time point t0 (ie, the onset year of the intervention, intercept) (IRR 1.73; 95% CI 1.68 to 1.78). Subsequently, a 20% decrease in the level (IRR 0.80; 95% CI 0.76 to 0.85) as well as a 48% decrease in the slope (IRR 0.52; 95% CI 0.50 to 0.54) of work disability was detected in comparison to the counterfactual scenario. In absolute terms, the immediate decrease in the level of work disability was 0.27 months, from 1.34 months per year in the onset year of rehabilitative psychotherapy to 1.07 months per year in the following year. Adjusting for measured time-varying covariates (employment status and purchases of prescribed psychotropic medication) had only a minor effect on the estimates. The adjusted models are presented in the online supplemental tables 1 and 2. Figure 1 illustrates the crude model prediction for the number of annual depression-related or anxiety-related work disability months.
Supplemental material
ITS analysis (GEE, Poisson regression) assessing change in level and slope of depression-related or anxiety-related work disability (annual number of work disability months) among rehabilitative psychotherapy recipients n(participants)=10 436, n(observations)=83 488

ITS analysis (GEE, Poisson regression) assessing the change in level and slope of depression-related or anxiety-related annual work disability months among rehabilitative psychotherapy recipients. Crude model. The dotted line illustrates the counterfactual scenario (ie, trend in absence of intervention). The zoomed inset provides the trend of the outcome among the rehabilitative psychotherapy recipients in more detail. The observed data points denote annual averages, and the line represents the GEE-model fit with the data, and the grey area signifies 95% CI. GEE, generalised estimating equation; ITS, interrupted time series.
{kind=link}
{kind=link}
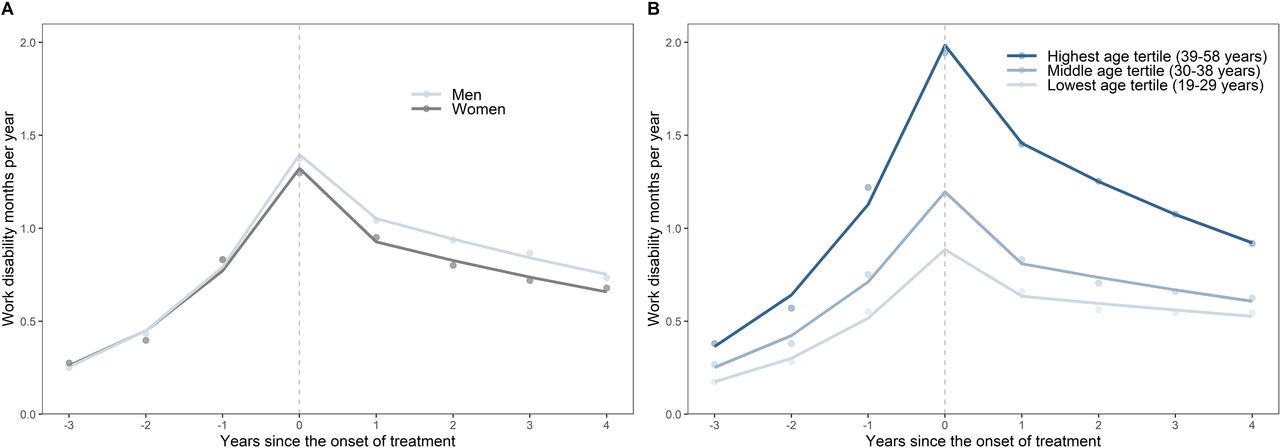
Trends of depression-related or anxiety-related annual work disability months among rehabilitative psychotherapy recipients by gender (A) and age tertile (B). Crude models. The observed data points (dots) denote annual averages, the lines represent GEE-model fits with the data. GEE, generalised estimating equation.
ITS analysis (GEE, Poisson regression) assessing change in level and slope of depression-related or anxiety-related work disability (annual number of work disability months) among rehabilitative psychotherapy recipients by gender and age tertile
Table 3 and figure 2 present the results of the stratified analyses. Among women, compared with the level of work disability in the onset year of rehabilitative psychotherapy, the level of work disability decreased by 21%, which corresponded to a reduction of 0.28 work disability months per year in the first full year of rehabilitative psychotherapy. Among men, the level of work disability decreased by 16%, which corresponded to a reduction of 0.22 work disability months per year in the first full year of rehabilitative psychotherapy. Overall, the differences between women and men were relatively small and not statistically significant (p>0.05). Adjusting for the measured time-varying covariates only had a minor effect on the estimates (online supplemental table 2).
In the youngest age group, the level of work disability decreased by 24% from the onset year of psychotherapy. This corresponded to a reduction of 0.21 work disability months per year during the first full year of psychotherapy. In the intermediate age group, the level of work disability decreased by 26%, which corresponded to a reduction of 0.31 work disability months per year in the first full year of psychotherapy. In the oldest age group, the level of work disability decreased by 14%, which corresponded to a reduction of 0.28 work disability months per year in the first full year of psychotherapy. Thus, in both relative and absolute terms, the intermediate age group seemed to have the largest decrease in the level of work disability, although these differences between the level changes in the age groups were not statistically significant (p>0.05).
The change in the slope (decrease) of work disability was, however, significantly steeper (a 51% reduction) in the oldest age group than in the youngest age group (p=0.019) and the intermediate age group (p=0.028). Adjusting for the measured time-varying covariates only had a minor effect on the estimates (online supplemental table 2).
Finally, as a supplementary analysis, we repeated the analysis using either depression-related or anxiety-related work disability as the outcome (online supplemental material). Based on the results of the supplementary analysis, our findings regarding the immediate decrease in disability were driven by depression-related work disability. The level of anxiety-related work disability was relatively low during the onset year of rehabilitative psychotherapy and there was no evident decrease in anxiety-related disability in the first full year of treatment. Both depression-related and anxiety-related work disability showed a gradual decrease in their slope of development during the treatment.
Discussion
In this study of the working-age population in Finland, we used nationwide register-based data to conduct an ITS analysis of annual months of mental health-related work disability before and after the onset of rehabilitative psychotherapy. We found that participating in rehabilitative psychotherapy marked a decline in depression-related or anxiety-related work disability in comparison to the counterfactual trend. Our findings are in accordance with a recent Finnish register-based longitudinal study,26 which found that rehabilitative psychotherapy was associated with an improvement in the employment and other labour market outcomes of the recipients of rehabilitative psychotherapy. Our findings are also in agreement with those of studies reporting the beneficial effects of psychotherapy on depression and anxiety. However, most of these previous results have been based on small-scale clinical trials that have focused on symptoms of depression or anxiety. Our register-based study contributes to the existing literature by examining nationwide data from an observational study setting and focusing on rehabilitative psychotherapy as a form of statutory rehabilitation aiming to improve work ability and labour market attachment of the recipients of this treatment.
Some previous studies of gender differences in the effects of psychotherapy have found that men and women benefit differently from therapy in terms of symptoms of depression or anxiety.27 28 Our results showed an equal decline in work disability among the men and women who participated in long-term psychotherapy. This inconsistency may reflect differences in outcomes.
We detected some differences between the age groups. The oldest age group had not only the highest level of work disability at the onset of psychotherapy but also the steepest decline in work disability during the follow-up in comparison to the two other age groups. Thus, on average, those in the oldest age group were to some extent more likely to benefit from rehabilitative psychotherapy than the younger age groups, at least in terms of change in work disability. It is possible that members of older age cohorts have (cognitive) skills, resources and prior life experiences that enable them to profit from rehabilitative psychotherapy more than members of younger cohorts. A systematic review of meta-analyses reported that in two meta-analyses, higher age was associated with a better outcome of psychotherapy for adult depression.29 In this study, it is also possible that it was the higher level of baseline work disability rather than age that contributed to the steeper decline. Moreover, 29% of participants in the youngest age group and 3% in the oldest age group were students. As students in Finland are less likely to apply for sickness benefits than employed individuals, it is likely that our disability measure did not capture the improvement of work disability so well among the youngest participants. Overall, we cannot draw very strong conclusions about the age group differences that we detected.
Our supplemental findings suggested that psychotherapy may show differential effects in depression and anxiety. However, baseline work disability was higher in those with depression than in those with anxiety and this may have contributed to the steeper decline of work disability among the depressed. More research is needed on this issue.
The accessibility of and compensation for psychotherapy is likely to affect the selection of patients or customers for psychotherapy. Thus, the effectiveness of psychotherapy on work disability is likely to depend on the social security system and the larger social context. Results from countries in which psychotherapy is statutory, like Finland, must be cautiously compared with results from countries in which the treatment is non-statutory. In Finland, psychotherapy has been statutory since 2011 and SII compensation covers around 55% of its expenses. This supports access to therapy among those with low incomes but may somewhat limit the use of long-term therapy to those who are financially better off.
A strength of this study is that its design was based on comprehensive, valid national registers with no loss to follow-up. In Finland, as well as in other Nordic countries, administrational registers are of good quality. The results can be generalised to the population level in Finland. ITS analysis has been argued to be the strongest quasi-experimental research design and particularly useful when a randomised trial is infeasible or unethical.30
However, the results must be interpreted with some caution as the strength of inference is weaker in the absence of a suitable control group. To begin with, our intention was to include a comparison group of those who did not participate in rehabilitative psychotherapy in the analyses to control for unknown time-varying confounders and, thus, improve the internal validity of the study. However, the recipients of rehabilitative psychotherapy were a selected group in several ways. One criterion for applying for statutory rehabilitative psychotherapy in Finland is an existing patient-care relationship (of at least 3 months) with a physician and a referral for psychotherapy from a psychiatrist. This information in addition to other factors that are likely to cause selection for treatment was not available from the registers. For example, we had no data on whether participants in the control group had received other treatment or mental health services. In the constructed control group, the level of mental health-related work disability of the participants was stable and at a lower level than in the intervention group. These groups could not be rendered comparable, and, consequently, a controlled ITS analysis was not feasible. The follow-up of 4 years (after the onset of therapy) did not allow us to make conclusions regarding long-term effects. We also lacked exact information on the approach or length of the rehabilitative psychotherapy received. Due to the age distribution of the individuals who received rehabilitative psychotherapy, the participants were, on average, relatively young. Consequently, the oldest age group covered a larger age range than the first two, younger age groups. This may have diluted our findings regarding the oldest age group
To conclude, mental health issues are a major public health concern. Depression (and related anxiety) is among the leading causes of disability globally. As well as the individual, mental health issues also affect the communities, and the economic burden of mental health-related disability is enormous. Preventive measures are needed, but at present, evidence-based, accessible treatment and mental health services are also essential. This longitudinal nationwide study based on administrative records suggests that providing statutory rehabilitative psychotherapy may increase work-life participation at the population level by reducing work disability. Nevertheless, studies carried out in different societal contexts and populations and with different methods are needed. Future cost-benefit analyses are required to estimate the economic value of subsidised rehabilitative psychotherapy.
Data availability statement
No data are available. No additional data are available because of Finnish legislation. Only researchers with the permission of the Finnish Social and Health Data Permit Authority and Statistics Finland have access to the analysed data.
Ethics statements
Patient consent for publication
Ethics approval
The ethics committee of the Finnish Institute of Occupational Health approved the study. The Finnish Social and Health Data Permit Authority and Statistics Finland both gave their permissions for data linkage and the use of these data sets.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tatsijatsi
Contributors Conceptualisation and methodology: JK, AV, KG, JT and SS; writing original draft preparation: JK; writing review and editing: JK, AV, KG, SS, JT and LP. All authors have read and agreed to the published version of the manuscript. Guarantor: JK
Funding This work was supported by the Social Insurance Institution of Finland (grant number 18/26/2020).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.