Article Text

Abstract
Background Type 2 diabetes mellitus (T2DM) has been associated with infectious diseases; however, whether T2DM is associated with bacterial-resistant infections has not been thoroughly studied. We ascertained whether people with T2DM were more likely to experience resistant infections in comparison to T2DM-free individuals.
Methods Systematic review and random-effects meta-analysis. The search was conducted in Medline, Embase and Global Health. We selected observational studies in which the outcome was resistant infections (any site), and the exposure was T2DM. We studied adult subjects who could have been selected from population-based or hospital-based studies. I2 was the metric of heterogeneity. We used the Newcastle-Ottawa risk of bias scale.
Results The search retrieved 3370 reports, 97 were studied in detail and 61 (449 247 subjects) were selected. Studies were mostly cross-sectional or case–control; several infection sites were studied, but mostly urinary tract and respiratory infections. The random-effects meta-analysis revealed that people with T2DM were twofold more likely to have urinary tract (OR=2.42; 95% CI 1.83 to 3.20; I2 19.1%) or respiratory (OR=2.35; 95% CI 1.49 to 3.69; I2 58.1%) resistant infections. Although evidence for other infection sites was heterogeneous, they consistently suggested that T2DM was associated with resistant infections.
Conclusions Compelling evidence suggests that people with T2DM are more likely to experience antibiotic-resistant urinary tract and respiratory infections. The evidence for other infection sites was less conclusive but pointed to the same overall conclusion. These results could guide empirical treatment for patients with T2DM and infections.
- nutritional sciences
- infections
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
With a large burden in terms of morbidity, mortality, disability and economic costs,1–4 type 2 diabetes mellitus (T2DM) is a global health problem disproportionally affecting low-income and middle-income countries (LMICs).1–4 While much of the research about T2DM has focused on its determinants, consequences and complications regarding non-communicable diseases, T2DM as a risk and prognostic factor for infectious—communicable—diseases has gained attention lately.5–8 In this relatively novel field—T2DM and infectious diseases—antibiotic resistance remains understudied, though it carries a large disease burden globally and in LMICs.9–13
Large studies about T2DM and antibiotic resistance have focused on one pathogen or colonisation (rather than infection).14 Moreover, there appears to be discrepancies on whether T2DM is a risk factor for infections with antibiotic-resistant bacteria depending on the infection site. For example, some authors have suggested that T2DM is not an independent risk factor for urinary tract infections with resistant bacteria;15 however, for community-acquired intra-abdominal infections, T2DM has been described as a potential risk factor.16
The large burden of T2DM,1–4 paired with its potential role as a risk and prognostic factor for infectious diseases,5–8 along with the global issue of antibiotic resistance,9–13 call to thoroughly study whether people with T2DM are at higher risk of infections with resistant bacteria. This knowledge may guide empirical treatment, with a subsequent positive impact on T2DM patients who would recover faster from infections, while also reducing the burden of antibiotic-resistant bacteria by prescribing more accurate treatments. Consequently, to understand whether T2DM is a risk factor for infections with resistant bacteria, in comparison to non-resistant infections, and whether there are any differences depending on the infection site, we conducted a systematic review of the scientific literature and a random-effects meta-analysis.
Methods
Protocol
We aimed to ascertain if people with T2DM, in comparison to otherwise healthy individuals, were more likely to experience a resistant infection rather than an infection with non-resistant bacteria. We hypothesised that, in comparison to T2DM-free individuals, people with T2DM who experience an infection, this is more likely to be an antibiotic-resistant infection. We conducted a systematic review and random-effects meta-analysis. The search strategies as well as the screening and selection processes were planned in advance and not modified afterwards. This manuscript adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations (online supplemental table 1).17
Supplemental material
Eligibility criteria
The inclusion criteria were: (i) the original studies could have been conducted in the community (eg, population-based random sampling) or in healthcare facilities (eg, consecutive patients in a clinic); (ii) original studies followed an observational design with a comparison group (eg, cross-sectional, case–control or prospective/retrospective cohorts); (iii) among the study participants, there were people with T2DM and without T2DM (comparison group); and (iv) the outcome was an infection with an antibiotic-resistant bacteria, as defined by each original report. Only studies with adult subjects were included.
The exclusion criteria were: (i) reports looking at colonisation with antibiotic-resistant bacteria (rather than infection) and (ii) research in which people with T2DM and other major or long-lasting conditions were studied, these included: neoplasms, tuberculosis, HIV/AIDS, bedridden, cerebral palsy, Alzheimer’s disease and vector-borne diseases (eg, malaria or dengue). We excluded these groups of patients because we targeted people with T2DM without any additional risk factors that could make them more likely to experience resistant infections. Studies looking at infections of viral aetiology were also excluded.
Information sources
We used OVID to search in Medline, Embase and Global Health. The search was conducted in February 2020. The search was restricted to studies with human beings; no further restrictions were included. The search terms we used are available in online supplemental table 2.
Search and study selection
The search results were downloaded to EndNote where duplicates were excluded. We then uploaded the results to Rayyan, an online open-access tool to conduct systematic reviews.18 Titles and abstracts were screened by two reviewers independently (RMC-L and AB-O); the same two reviewers studied the complete text of the reports selected in the screening phase. Discrepancies were solved by consensus between these two reviewers.
Data collection
Data from the selected reports were extracted by two groups of reviewers independently (CA-R and GS-Z as well as JHZ-T and DV-Z). Discrepancies were solved by consensus within and between these pairs of reviewers, or by consensus with a third party (RMC-L). We designed a data extraction form which was agreed on by consensus among all the reviewers; this form was not modified during data collation.
The data extraction form included study characteristics (eg, year and country of data collection, whether population-based or hospital-based, and study design), and characteristics of the study population (eg, mean age, proportion of men and T2DM proportion). We also extracted information about the infection: infection site, as well as frequency of people with and without T2DM with a resistant infection; when available, we also collated information about the specific pathogens studied and antibiotics tested. When original studies reported an association metric (and not only proportions), we extracted those as presented in the reports (eg, OR, prevalence ratio or risk ratio). Of note, the meta-analysis is based on adjusted association metrics only; these were prioritised over unadjusted estimates because adjusted estimates would reflect solid and less biased evidence.
Risk of bias in individual studies
We assessed the risk of bias of individual studies with the Newcastle-Ottawa Scale, a tool to assess quality of non-randomised studies.19 For case–control and cohort studies, we used the specific scales for these study designs. For cross-sectional studies, however, we used the same scale as for cohort studies applying all relevant criteria. This tool ranks studies with stars, where the more stars the less risk of bias the study shows. This process was conducted by two reviewers independently (CA-R and GS-Z; JHZ-T and DV-Z), and discrepancies were solved by consensus among them or after further consideration with a third party (RMC-L).
Synthesis of results
First, we narratively presented the collated information for all the selected studies. Before data analysis, we decided to conduct a meta-analysis if there were at least four estimates per infection site (ie, at least four original publications or results). In the meta-analysis, we combined all study designs (cross-sectional, prospective and case–control studies), but only estimates of the same infection site (eg, urinary tract infections). We also combined estimates regardless of the specific bacteria or antibiotic studied. We only pooled adjusted estimates available in the original reports. We conducted a random-effects meta-analysis in Stata V.15 (StrataCorp) with the DerSimonian and Laird method. Pooled estimates are reported as OR and 95% CIs. Because of the limited number of studies with similar specific characteristics, it was no possible to conduct subgroup analyses (eg, by resistant bacteria or community-based vs hospital-based studies); however, when possible, pooled estimates were reported separately by cross-sectional/cohort or case–control studies. Finally, the I2 was reported as a metric of heterogeneity. A priori, we expected heterogeneity across reports because they studied different populations, were conducted in unique settings, and followed different methods.
Results
Study characteristics
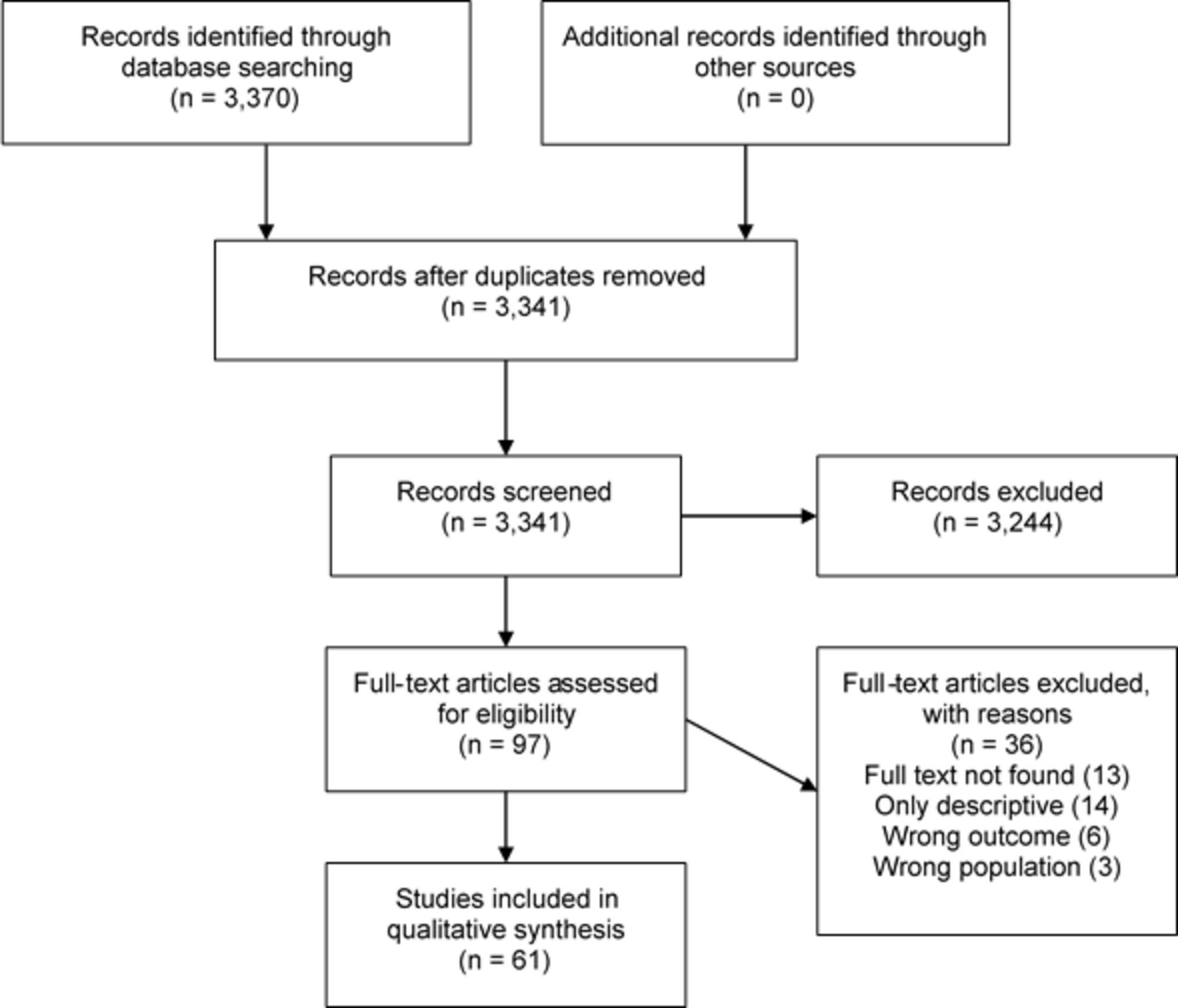
The search yielded 3370 results, we screened 3341 and studied in detail 97 reports; finally, 61 (449 247 subjects) reports were included in the review (figure 1, tables 1 and 2). Reports were informed by data collected since 198920–2017.21 22 The studies were conducted in Argentina,16 Bangladesh,23 24 Belgium,25 Brazil,26 27 Canada,28 29 China,21 30–32 Egypt,33 Finland,34 France,35–37 Germany,37 Greece,38 Guyana,22 India,39 Italy,37 40 Israel,28 41–43 Japan,44 Korea,45 46 Madagascar,47 Nepal,48 Netherlands,15 Norway,49 Pakistan,50 Poland,51 Singapore,20 52 53 Spain,37 54–57 Sweden,34 58 USA,37 59–75 Taiwan76 77 and Thailand.78

{kind=link}
Study selection process. Depending on the outcome and subgroup analysis, the number of studies included in the meta-analysis varied. Therefore, the number of selected reports for quantitative synthesis is not reported in this figure but reported in the text.
Characteristics of cross-sectional and cohort reports
Characteristics of case–control reports
Evidence was mostly derived from cross-sectional (29 reports),16 20–22 25 28 30 31 33–38 40 44 47 48 52 53 60–65 76 77 and case–control (28 reports)15 23 24 27 32 39 41–43 45 46 49 50 54–58 66–75 78 studies; fewer followed a cohort (five reports)26 29 51 59 61 design (tables 1 and 2); of note one report contributed to both the cross-sectional and cohort count.61
Infection sites reported varied among urinary tract (34 reports),15 20 23 26 28 30 33 36 38–41 43 45 47–49 53–55 57 62 63 65–67 69 70 74–78 respiratory (11 reports),21 24 28 31 32 37 46 64 68 69 78 skin and soft tissue (6 reports),22 34 52 59 60 62 intra-abdominal (2 reports),16 65 surgical wounds (2 reports)47 67 and ophthalmic (1 report)35 (table 3).
Adjusted association estimates of antibiotic-resistant from cross-sectional and cohort reports
Infections
We report on adjusted association estimates as these were available in the original publications because these represent the most reliable and robust evidence (tables 3 and 4). Crude estimates and frequencies are available in online supplemental tables 3 and 4. Most studies reported that resistant infections were more frequent among people with T2DM in comparison to T2DM-free individuals; this observation was consistent across infection sites and study designs. Overall, regardless of the infection site, T2DM appears to be a risk factor for resistant infections (tables 3 and 4). Evidence to support this statement was weak only in a few studies as their estimates were not significant.15 34 45 Across infection sites, the comparison group was an infection with a non-resistant bacteria (rather than no infection or colonisation), except for two reports,42 50 where patients were colonised but did not develop an infection.
Adjusted association estimates of antibiotic-resistant from case–control reports
The association estimates from cross-sectional or cohort studies were as high as fivefold (OR=5.2, 95% CI 1.4 to 19.8) for surgical wounds, blood, urinary and respiratory tract or burn infections;47 other studies also reported a similar association estimate for urinary tract, skin or soft tissue infections (OR=5.1, 95% CI 2.1 to 18.6).62 On the other hand, the smallest estimate was 1.70 (95% CI 1.0 to 2.8) for community-acquired pneumonia.64
The association estimates from case–control studies showed a similar pattern. The largest estimate showed an OR of 6.4 (95% CI 2.1 to 19.3) for respiratory, urinary, wound or bloodstream infections.69 At the other extreme, people with T2DM had 50% higher odds of a resistant urinary or bloodstream infection (OR=1.5, 95% CI 1.2 to 1.8).70
Meta-analysis
We further elaborated on urinary tract infections because most studies addressed this condition. The pooled OR across 10 reports,15 30 43 45 49 53 66 75–77 supported the premise that people with T2DM were most likely to have a resistant infection in the urinary tract, rather than a non-resistant infection: OR=2.42 (95% CI 1.83 to 3.20; I2 19.1%; 3675 subjects). When only cross-sectional studies were pooled (all hospital-based), the summary estimate based on these four studies was30 53 76 77: OR=2.92 (95% CI 2.02 to 4.21; I2 00.0%; 1312 subjects); alternatively, when only case–control studies were pooled (all hospital-based), the summary estimate based on these six studies was15 43 45 49 66 75: OR=2.07 (95% CI 1.37 to 3.12; I2 30.3%; 2363 subjects). These reports analysed a range of bacteria and antibiotics, and consistently suggested that people with T2DM were most likely to experience a resistant infection in the urinary tract (tables 3 and 4), rather than a non-resistant infection.
There were also at least four estimates to conduct a meta-analysis for respiratory tract infections.32 37 64 This analysis also suggested that people with T2DM showed higher odds of resistant infections: OR=2.35 (95% CI 1.49 to 3.69; I2 58.1%; 1637 subjects). It is noteworthy that one study64 contributed with two estimates from the same study population (375 subjects), thus it was considered twice for this meta-analysis. There were three cross-sectional hospital-based studies,37 64 and one case–control hospital-based study32; therefore, further stratification by study design was not possible. These reports analysed a range of bacteria and antibiotics, consistently suggesting that resistant infections were more likely in people with T2DM (tables 3 and 4). Overall, people with T2DM appear to be at higher risk of a resistant respiratory infection.
Five estimates from the same study informed the pooled analysis for complicated skin infections: OR=0.98 (95% CI 0.68 to 1.41; I2 43.3%; 390 subjects). This was a cross-sectional hospital-based study, which analysed different antibiotics and bacteria (table 3).34 The available evidence is still inconclusive on whether people with T2DM have higher risk of complicated skin infections. Similarly, for other infection sites, it was not possible to reach strong conclusions or to conduct a meta-analysis, because the body of evidence was small or there was large heterogeneity (tables 3 and 4).
Risk of bias
On average, the summarised reports had 5.9 stars in the risk of bias assessment tool (online supplemental table 5), with just a few showing fewer than four stars mostly because some criteria did not apply for the study design, or information was not available or was unclear.20 28 38 48 52
Discussion
Summary of the evidence
The evidence suggests that, in comparison to T2DM-free subjects, people with T2DM who acquire a urinary tract and respiratory infection, are more likely to experience a resistant infection. The evidence for other infection sites was less conclusive because of fewer reports and large heterogeneity in the outcomes. The body of evidence studying T2DM as an associated factor for resistant infections has increased, suggesting that researchers and practitioners find this topic relevant. This work has summarised and pooled available evidence and delivered strong conclusions about two infection sites, while signalling other infections sites that warrant further research.
Pathways behind T2DM and resistant infections
A comprehensive discussion on the immunological or pharmacological mechanisms involved in the association between T2DM and resistant infections is beyond the scope of this work. Nonetheless, we acknowledge that T2DM negatively interacts with the immune system and could be a risk factor for infections.79–83 In this line, other conditions related with T2DM, obesity for example, have been associated with an increased risk of infections due to the role of adipose tissue in the production of proinflammatory cytokines (tumor necrosis factor (TNF)-α, interleukin (IL) 6, IL-1β, IL-18, monocyte chemoattractant protein (MCP)-1), proinflammatory adipokines and other inflammatory products;84 85 another point is the pharmacokinetics of antibiotics in obese population that can lead to suboptimal levels of antibiotic concentrations and increase the risk for antibiotic resistance.86
Whether the impaired immune system is responsible for higher risk of resistant infections in people with T2DM, has not been studied to the best of our knowledge. Another pending question is whether the frequency with which people with T2DM visit clinics or hospitals is a risk factor for resistant infections. That is, people with T2DM have more contact with healthcare facilities because of regular control visits or other related complications. In these visits, they could acquire infections with in-hospital bacteria, perhaps more likely to be resistant.
Public health and clinical practice implications
The estimates herein summarised could inform clinical practice for people with T2DM. Our estimates support the fact that T2DM are more likely to have resistant infections, particularly urinary tract and respiratory infections. Empirical treatment for these infection sites in people with T2DM needs to be carefully thought; that is, the empirical treatment for the general population may not be the best option in people with T2DM. This does not imply starting treatment with a very powerful antibiotic, but to carefully consider available options and if possible, request an antibiotic sensitivity test to inform the empirical treatment choice.
From a health economics perspective, treatment failure with a first-line antibiotic because of antibiotic resistance in people with T2DM would impose a large economic burden.10 87 These T2DM patients may need a second appointment with their medic, and start a different course of antibiotics; in the worst-case scenario, the infection could progress and develop some complication. These are additional costs for the health system or the patient.
Resistant infections are a major concern in infectious diseases medicine. For example, the burden of resistant tuberculosis88 has received great attention, it is frequently monitored, and guides diagnosis and treatment allocation. Talking about resistant infections in the field of non-communicable diseases is new, yet some authors have already highlighted the links between communicable and non-communicable diseases.5–8 A surveillance system of antibiotic resistance profiles among people with T2DM could be implemented to identify the most dangerous bacteria, select the best treatment considering other concomitant risk factor such as obesity,86 and monitor trends of the resistance patterns in the T2DM community. An antibiotic resistance surveillance programme could inform local and international guidelines for infections in people with T2DM.
There are clinical practice guidelines for diabetic food infections,89 which represent a great burden on T2DM patients. Guidelines for other infections in people with T2DM are less common. Although available guidelines, for example, those for urinary tract infections,90 91 acknowledge T2DM as a risk factor for asymptomatic bacteriuria or complicated infections, little is discussed about antibiotic resistance or tailored treatment choices for people with T2DM. Our work, accounting for its limitations, could be adopted by these guidelines to suggest some pragmatic approaches for people with T2DM. For example: (i) carefully contemplate the empirical treatment considering that the choices for the general population may not be ideal for T2DM patients or (ii) consider an antibiogram before starting any empirical treatment. Ideally, experimental studies would come to further strengthen—or reject—these suggestions for the benefit of T2DM patients. We advocate for a map of antibiotic-resistant profile in people with T2DM, at least for the urinary tract and respiratory infections, and diabetic foot infections.89 This evidence would have a positive impact on guiding empirical treatment for people with T2DM.
It is worth noting that most of the original studies herein summarised were hospital-based or conducted with captive populations (eg, nursing homes). Whether the same findings would apply to the general population in community-based or population-based studies with implications in primary care, deserves further investigation.
Limitations
We conducted a comprehensive review following standard methods. However, there are also some limitations to acknowledge. First, it was not always specified whether the original studies referred to T2DM patients alone; that is, we cannot be certain that type 1 diabetes mellitus patients were fully excluded. However, because we focused on adults, in whom the overall prevalence of T2DM is the largest relative to other types of diabetes, it is reasonable to consider that only (or mostly) T2DM patients were studied. Second, in many studies the sample size was limited particularly when authors tried to look at specific subgroups. More comprehensive and larger research is needed in this field, particularly with other infection sites where evidence is much limited. Third, a consequence of a limited sample size is the lack of multivariable models. It was challenging to ascertain whether T2DM is an independent risk factor for resistant infections. Metabolic control as per HbA1c levels and hyperglycaemic status are relevant variables to account for.79–83 Future studies should include HbA1c and other variables. Fourth, original studies followed different designs and sampling frameworks. Electronic health records could provide a remarkable and timely opportunity to further explore the role of T2DM in resistant infections.
Conclusions
This systematic review and meta-analysis found evidence signalling that people with T2DM are more likely to experience resistant urinary tract and respiratory infections. Although the evidence for other infection sites was less conclusive, it already pinpoints that people with T2DM are more likely to have resistant infections regardless of the infection site. This evidence, along with clinical knowledge and decision-sharing, could guide empirical treatment for patients with T2DM and infections.
What is already known on this subject
There is a growing body of evidence about diabetes as a risk factor for infectious diseases and antibiotic-resistant infections; however, there is great heterogeneity among individual reports and most studies included small samples. This sparse evidence limits our understanding of diabetes as a compelling risk factor for antibiotic-resistant infections.
What this study adds
Diabetes appears to be a strong risk factor for antibiotic-resistant infections, particularly urinary tract and respiratory infections. Although evidence for other infection sites was limited, in terms of quantity, quality and with great heterogeneity, their findings already suggested that diabetes was associated with higher risk of resistant infections. This evidence could inform clinical guidelines for infectious diseases, with focus on people with diabetes, which is a large and growing proportion of the general population.
Ethics statements
Patient consent for publication
Ethics approval
This is a review of published scientific information. This work did not study, directly, any human beings and was thus considered of low risk. We did not seek approval from an Ethics Committee or Institutional Review Board. All authors had access to the collated data and are collectively responsible for the accuracy of the data, results interpretation and conclusions. All authors approved the submitted version. The funder had no role in the study design, analyses, interpretation or conclusions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @cecianza
Contributors RMC-L and AB-O conceived the idea. RMC-L and AB-O conducted the search, the screening and the final study selection. CA-R, GS-Z, DV-Z and JHZ-T extracted the information from the selected reports. RMC-L wrote the manuscript with support from CA-R, AB-O and CU-G. All author approved the submitted version. RMC-L, AB-O, CA-R, GS-Z, DV-Z and JHZ-T are collectively responsible for the accuracy of the information.
Funding RMC-L has been supported by a Strategic Award, Wellcome Trust-Imperial College Centre for Global Health Research (100693/Z/12/Z) and Imperial College London Wellcome Trust Institutional Strategic Support Fund (Global Health Clinical Research Training Fellowship) (294834/Z/16/Z ISSF ICL). RMC-L is supported by a Wellcome Trust International Training Fellowship (214185/Z/18/Z).
Disclaimer The funder had no role in this work and decision to submit for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.