Article Text

Abstract
With almost no community-transmitted cases and without any complete lockdown throughout 2020, Taiwan is one of very few countries worldwide that has recorded minimal impact from the COVID-19 pandemic attack. This is despite being only 130 km from China and having frequent business communications with that country, where COVID-19 first emerged. At the end of December 2020, Taiwan had recorded just 873 cases and 7 deaths, in a country of around 24 million people. How to determine the effectiveness of public health policies is an important issue that must be resolved, especially in those countries that have experienced few cases of community-transmitted COVID-19. Our analysis of epidemiological data in Taiwan relating to influenza-like illness (ILI), enterovirus and diarrhoea from the past 3 years reveals dramatic reductions in the incidence of ILI and enterovirus in 2020, compared with 2018 and 2019. These reductions occurred within 2 weeks of the government issuing public health policies for COVID-19 and indicate that such policies can effectively reduce infectious diseases overall. In contrast, no such reduction in ILI activity was observed in 2020 after the first COVID-19 case was reported in the USA. We suggest that infectious diseases data can be used to inform effective public health policies needed to break the transmission chain of COVID-19 and that ongoing monitoring of infectious diseases data can provide confidence about nationwide health.
- COVID-19
- control of diseases
- epidemiology
Data availability statement
Data are available in a public, open access repository. Data are available at the Taiwan CDC website: http://nidss.cdc.gov.tw/en/, the US Influenza Surveillance System via this website: https://www.cdc.gov/flu/weekly/index.htm, and the COVID-19 website: https://www.cdc.gov/coronavirus/2019-ncov/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Shortly after the first case of severe pneumonia of unknown origin was reported in Wuhan, China, in December 2019, scientists established that the infectious agent of this novel coronavirus disease is SARS-CoV-2 (SARS-CoV-2, known as COVID-19), which is closely related genetically to the first novel and deadly coronavirus, SARS-CoV, which emerged in late 2002 and caused a global SARS outbreak.1 Following the first documented case of SARS-CoV-2 on 31 December 2019, COVID-19 spread rapidly across China in the first 2 months of 2020.2
With almost no community-transmitted cases to date and without any complete lockdown, Taiwan is one of very few countries worldwide that have recorded minimal impact from the COVID-19 pandemic. This is despite being only 130 km from China and having frequent business communications with that country, where COVID-19 first emerged. By the beginning of December 2020, Taiwan had recorded just 679 cases and 7 deaths, in a country of around 24 million people.3 Ever since the emergence of COVID-19, people in Taiwan have continued to live their normal daily routines, with schools and all other educational institutions, shops, businesses and restaurants remaining open, and all sorts of gatherings and activities permitted.
This success is largely explained by public health policies for COVID-19 issued soon after the first case was identified in Taiwan. Isolation and quarantine policies apply to every overseas arrival and many health and safety rules apply in public places, including body temperature examinations at every point of entry in department stores and restaurants, strict sanitation and hygiene measures mandating the wearing of surgical masks and social distancing requirements. Many institutions maintain daily records of body temperature for their employees. The government’s contact tracing assessment prevents further spread of the virus and strict public health policies remain in place, despite very few imported cases. In contrast, other countries that initially had fewer cases, such as Vietnam and Japan, experienced one or more surges of COVID-19 infections after relaxing their public health policies.4 5 How do we quantify the efficacy of public health policies in a country such as Taiwan, which has had very few COVID-19 cases, and how do we decide when to loosen or further tighten the quarantine policy? Is it possible to have a marker to estimate the effectiveness of public health policies needed to break the transmission chain of COVID-19?
Taiwan is one of the most populous counties worldwide, with a population density of 651 persons/km2, higher than either of its close neighbours Japan and Korea (with population densities of 333 and 516, respectively).6 Population density is an important factor that can increase susceptibility for infectious diseases, including COVID-19. This disease is easily transmitted between humans through close contact or via droplets from an infected person who is coughing, sneezing or talking. Its transmission route is the same as other diseases, such as influenza,1 a respiratory disease transmitted via droplets or enteroviruses, which are most commonly transmitted via close person-to-person contact. Enteroviruses, especially Enterovirus 71, have a major public health impact in the Asia-Pacific region7 and are epidemic in Taiwan.8 Thus, Taiwan’s Centers for Disease Control and Prevention (CDC) maintains close surveillance of both influenza and enterovirus. Our analysis of retrospective data from Taiwan relating to influenza-like illness (ILI), enterovirus and diarrhoea from the past 3 years reveals dramatic differences in the incidence of enterovirus and, to a lesser extent, ILI, in 2020 compared with the previous years. These findings suggest that the country’s public health policies are effective in reducing the spread of infectious diseases and may mitigate the impact of the COVID-19 pandemic.
Data sources
Percentages of outpatient visits with a clinical diagnosis of ILI, enterovirus infection or diarrhoea reported in Taiwan were collected from Taiwan’s CDC. Data for 2018, 2019 and to the end of December 2020 are presented by epidemiological week, which directly reflect the incidence of these diseases.9 10 Data were accessed from Taiwan’s National Infectious Disease Statistics System, a public and nationwide database that provides real-time epidemiological information accessible via Taiwan’s CDC website: http://nidss.cdc.gov.tw/en/.
Percentages of outpatient visits with a clinical diagnosis of ILI or COVID-19-like illness (CLI) reported in the USA were accessed from the US CDC. ILI data were accessed from the US Influenza Surveillance System via this website: https://www.cdc.gov/flu/weekly/index.htm.11 12 Two syndromic surveillance systems, the US Outpatient ILI Surveillance Network and the National Syndromic Surveillance Project, were used to monitor trends in outpatient and emergency department visits that may be associated with CLI. CLI data were accessed via this website: https://www.cdc.gov/coronavirus/2019-ncov/.
Results
Epidemiological findings reveal associations between the incidence of ILI and enterovirus and the effectiveness of public health policies for COVID-19
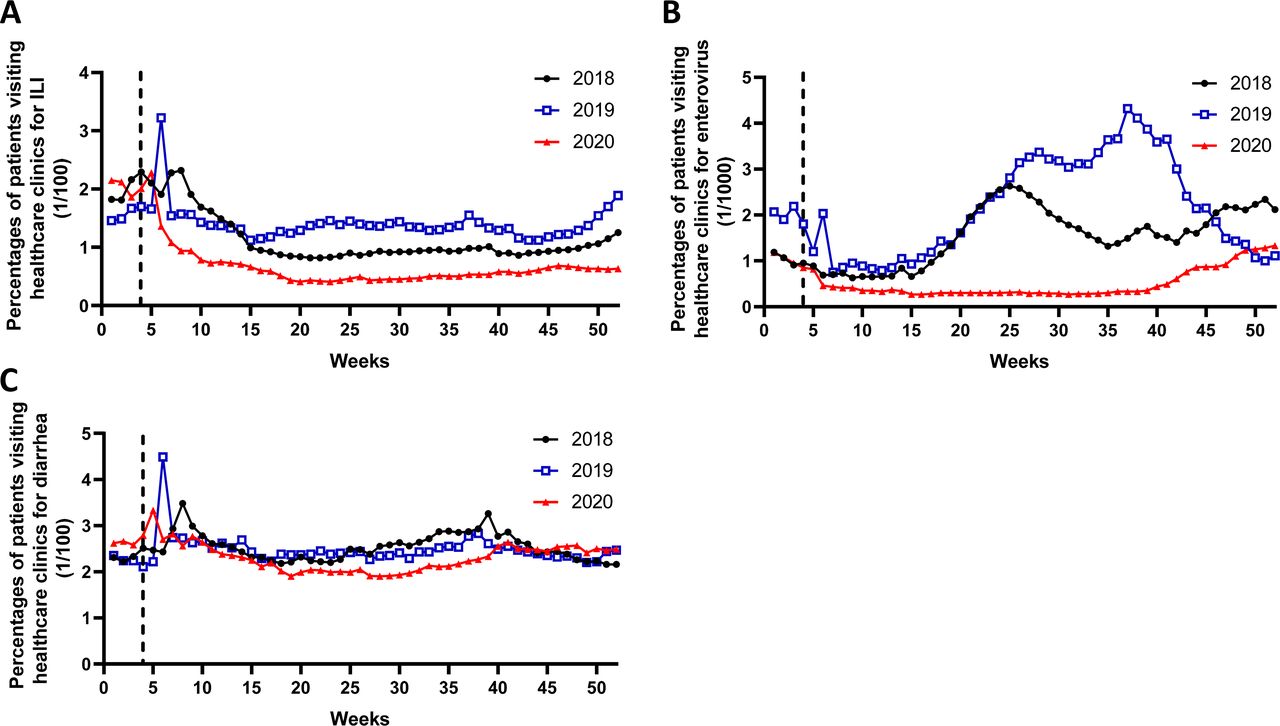
Early in 2020, Taiwan identified its first case of COVID-19 (21 January; week 4), to which the government responded with new, strict public health policies.13 Two weeks later, Taiwan recorded dramatic reductions in the percentage of outpatient visits with diagnoses of ILI (an acute respiratory illness with a measured temperature of ≥38°C and cough, with onset within the past 10 days14 (figure 1A). These diseases share similar transmission routes to those of COVID-19, that is, occurring through direct, indirect or close contact with infected persons secreting respiratory droplets, respiratory secretions and saliva. The ILI percentages in 2020 are dramatically lower than those that start from week 6 reported by Taiwan’s CDC in 2018 and 2019 (figure 1A), which suggests that the new policies in 2020 have reduced respiratory viral transmission nationwide. The same observation applies to enterovirus infections, which are mainly transmitted person-to-person through faecal-oral routes and oral-oral routes from infected faeces and saliva, and can be prevented with scrupulous attention to personal hygiene and environmental cleanliness. Notably, as well as the obvious reductions in outpatient visits for enterovirus infections starting from week 6 in 2020, which resemble the ILI data, the high seasonal peaks for enterovirus infections in 2018 (week 25) and 2019 (week 37) did not occur in 2020 (figure 1B). These reductions occurred within 2 weeks of the government issuing public health policies for COVID-19 and indicate that such policies can effectively reduce infectious diseases overall. Importantly, while a trend can be observed demonstrating increasing disease activity from week 42 up to the end of December 2020, there was no pandemic-like outbreak. This outcome emphasises the efficiency of the government’s public health strategies in preventing the pandemic potential of enteroviruses. In contrast, data for diarrhoea caused by noninfectious diseases are very similar from 2018 through 2020 (figure 1C).

Percentages of outpatient visits with a clinical diagnosis of (A) ILI, (B) enterovirus infection or (C) diarrhoea reported to the Taiwan CDC in 2018, 2019 and 2020, by surveillance epidemiological week. The dashed lines represent the week of the first COVID-19 case identified in Taiwan. CDC, Centers for Disease Control and Prevention; ILI, influenza-like illness.
In figure 2, the comparison of ILI data from the USA for 2019 to the end of December 2020 reveals no obvious fall in numbers of cases following the first identified US COVID-19 case on 15 January 2020 (week 3). From week 10 in 2020, the USA experienced a sharp increase in CLI (ie, symptoms of fever plus cough and/or shortness of breath or difficulty breathing) that peaked around week 15.

{kind=link}
{kind=link}
US CDC data for ILI and CLI activity for 2019 and 2020 by epidemiological week. The dashed lines represent the week of the first COVID-19 case identified in the USA. CDC, Centers for Disease Control and Prevention; CLI, COVID-19-like illness; ILI, influenza-like illness.
Discussion
Taiwan’s government was swift to issue strict public health measures following the country’s first identified case of COVID-19 in January 2020. These measures were soon followed by substantial reductions in outpatient diagnoses of ILI, compared with around the same period of time in 2018 and 2019. It is important to note that multiple respiratory infectious diseases contribute to ILI.15 These much lower ILI percentages in 2020 compared with those in 2018 and 2019 suggest that the new policies in 2020 have reduced respiratory viral transmission nationwide. These diseases share similar transmission routes to those of COVID-19, that is, occurring through direct, indirect or close contact with infected persons secreting respiratory droplets, respiratory secretions and saliva. The same observation applies to enterovirus infections, which are mainly transmitted person-to-person and can be prevented with scrupulous attention to personal hygiene and environmental cleanliness. In 2020, Taiwan has avoided the high seasonal peaks for enterovirus infections that occurred in both 2018 and 2019. Interestingly, these polices have not affected diarrhoea caused by noninfectious diseases, as the data are very similar from 2018 through 2020 (figure 1C). This outcome emphasises the efficiency of the government’s public health strategies in preventing the pandemic potential of both ILI and enteroviruses.
Our results indicate that public health policies for COVID-19 have effectively reduced the spread of ILI and enterovirus infections in Taiwan. Since the lack of COVID-19 case data for Taiwan prevents direct comparison of statistics from other countries, we have compared recent data for other transmissible epidemic infectious diseases in Taiwan with data from the USA, which is currently reporting very high COVID-19 caseloads. When we compared ILI percentages between 2019 and 2020 in the USA, a country with extremely high COVID-19 rates, we did not observe any dramatic reduction in ILI after the first identified US COVID-19 case in January 2020 (week 3) (figure 2). Following that case, despite several public health policies issued by the US government, no reduction in ILI was observed. Instead, the USA experienced a high peak of CLI. Notably, mild-COVID-19 illness presents with symptoms similar to ILI, which may be a confounding factor for statistical analysis of these percentages. At the time of writing this report, we predict that the USA faces huge challenges as it enters winter, as the highest seasonal peak for ILI that generally occurs at around week 50 will obstruct any efforts to reduce COVID-19 transmission rates. Notably, an observable trend revealed increasing disease activity for enterovirus in Taiwan (figure 1) from week 42 up to the end of 2020, which likely reflects the relaxation of peoples’ attitudes towards public health policies during the Mid-Autumn Festival national holiday (1 October to 4 October at epidemiology week 40) and the holidays around Double Tenth Day (9 October through 11 October at epidemiology week 41). Our analysis of retrospective data from Taiwan suggests that ongoing monitoring of infectious diseases data can provide confidence about nationwide health. Moreover, the reduction of ILI/enterovirus occurred within 2 weeks of the government issuing public health policies in relation to the first case of COVID-19, which indicates that such policies can effectively reduce infectious diseases overall and perhaps prevent chains of disease transmission at the very beginning of highly infectious viral infections, such as COVID-19.
Unlike other countries worldwide, Taiwan experienced many deaths during the SARS outbreak in 2003, which included hospital-acquired infections and resulted in 346 officially confirmed cases, among which were 37 direct SARS deaths (cause of death was recorded as SARS) and 36 SARS-related deaths (cause of death was not directly attributed to SARS).16 SARS endangered both the country’s economy and public health. However, this highly lethal disease disappeared in the wake of intense public health mitigation measures. Seventeen years later, the government of Taiwan showed how much it had learnt from that SARS-CoV outbreak by deciding to close its borders with China as soon as the COVID-19 pandemic started on 23 January 2020. Public health policies were simultaneously enacted that were designed to effectively halt COVID-19 transmission in Taiwan without having to implement a complete lockdown process. SARS-CoV heightened a sense of vigilance and responsibility among people, especially in relation to wearing face masks. Thus, for several years before COVID-19, people were already accustomed to wearing face masks to protect themselves from other communicable diseases and from the effects of air pollution. This explains why, despite Taiwan having so few COVID-19 cases, people willingly wear face masks when out in public. The SARS experience also inspired Taiwan’s government to build a comprehensive system to monitor contagious diseases and prevent the spread of any novel viruses. Soon after the COVID-19 outbreak in late January 2020, the government invested NT$200 million (US$6.6 million) in 90 production lines for surgical masks, increasing the daily production capacity of surgical masks from 1.88 million to 17 million by mid-April. On 24 January 2020, the government also announced a month-long export ban on surgical masks, followed soon after by a mask rationing system to prevent panic hoarding of masks and ensure universal access. Now, masks are easily procurable. Whereas many other countries experienced shortages for several months, people in Taiwan have been able to buy surgical masks throughout 2020 at an affordable price (NT$5; US$0.16 per unit). Taiwan has proven that public health policies can break the transmission of COVID-19. We suggest that these policies could be usefully applied to other countries worldwide that are experiencing ongoing COVID-19 infections.
Data availability statement
Data are available in a public, open access repository. Data are available at the Taiwan CDC website: http://nidss.cdc.gov.tw/en/, the US Influenza Surveillance System via this website: https://www.cdc.gov/flu/weekly/index.htm, and the COVID-19 website: https://www.cdc.gov/coronavirus/2019-ncov/.
Ethics statements
Footnotes
IM and J-LH are joint first authors.
Contributors J-LH and IM wrote the manuscript. J-LH prepared the figures. Both authors reviewed the manuscript.
Funding This investigation was supported by the Ministry of Science and Technology, Taiwan (MOST 109–2628-B-039–004) and China Medical University, Taiwan (1095310A).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.