Article Text

Abstract
Aims While investigators have typically quantified the health risk of passive (secondhand) smoking by using self-reported data, these are liable to measurement error. By pooling data across studies, we examined the prospective relation of a biochemical assessment of passive smoking, salivary cotinine, with mortality from a range of causes.
Methods We combined data from 12 cohort studies from England and Scotland initiated between 1998 and 2008. A total of 36 584 men and women aged 16–85 years of age reported that they were non-smoking at baseline, provided baseline salivary cotinine and consented to mortality record linkage.
Results A mean of 8.1 years of mortality follow-up of 36 584 non-smokers (16 792 men and 19 792 women) gave rise to 2367 deaths (775 from cardiovascular disease, 779 from all cancers and 289 from smoking-related cancers). After controlling for a range of covariates, a 10 ng/mL increase in salivary cotinine was related to an elevated risk of total (HRs; 95% CI) (1.46; 1.16 to 1.83), cardiovascular disease (1.41; 0.96 to 2.09), cancer (1.49; 1.00 to 2.22) and smoking-related cancer mortality (2.92; 1.77 to 4.83).
Conclusions Assessed biomedically, passive smoking was a risk factor for a range of health outcomes known to be causally linked to active smoking.
- passive smoking
- measurement
- mortality
Data availability statement
Data are available in a public, open access repository. Data can be downloaded from the UK data archive (www.data-archive.ac.uk).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Although there have been substantial secular declines in smoking prevalence in adults in the western world in recent years, more than 7 million UK adults still engage in the habit,1 and there are estimated to be over 1 billion smokers worldwide.2 Consequently, although perhaps overestimates owing to the implementation of smoking bans in bars and restaurants in the UK,3 in 2002, up to 13% of non-smokers reported being passively exposed to tobacco smoke in the home and 10% in the workplace.4
Globally each year more than 1 million individuals are thought to die from passive smoking, also known as secondhand smoking or environmental tobacco smoke.2 Such estimates are based on the numerous studies that have explored the health consequences of passive smoking with the suggestion that it is linked to most diseases known to be caused by active smoking, including cardiovascular disease and selected cancers.5 In these studies, investigators have typically relied on self-reported measures of passive smoking, raising concerns regarding reporting error. Furthermore, some of the evidence is based on case–control studies6–9 raising methodological concerns regarding reporting bias and reverse causality. While more recent reports have used biomarkers of passive smoking in analyses of mortality or morbidity cohort data,10–12 interpretation of these findings is hampered by the small size of most studies. Accordingly, we pooled data for non-smokers across 12 cohort studies to explore the relation of salivary cotinine, a widely used indicator of passive smoking,13 with the risk of cause-specific mortality.
Methods
The Scottish Health Survey (SHS)14 and the Health Survey for England (HSE)15 are independent, near-identical, cross-sectional, general population-based studies examining individuals living in households in each country. Described extensively elsewhere,16–18 in the present analyses, study members were aged 16–85 years at recruitment and were subsequently linked to a national cause-of-death registry. For the present analyses, we used only those surveys with salivary cotinine data (SHS 1998 and 2003; HSE 1997–2004, 2007 and 2008). Participants gave full consent.
Assessment of active and passive smoking
Data on self-reported smoking were collected using standard enquiries (current, former and never smokers). For the cotinine assessment, a dental roll saturated with participant saliva was later analysed using a gas chromatographic method (Hewlett Packard HP5890) with a lower limit of detection of 0.1 ng/mL (levels below 0.1 ng/mL are regarded as being undetectable).19 In the 2008 HSE, this methodology was changed to a liquid chromatography–tandem mass spectrometry method,19 but the two methods produce comparable results.20 21 Internal quality control is described elsewhere.22 Average coefficient of variation is 3.9% in the range 1–1000 ng/mL.19 22 Salivary cotinine, a metabolite (and anagram) of nicotine, is shown to be a valid marker of tobacco smoke exposure in the previous 72 hours and to show sufficiently high specificity and sensitivity for the purposes of population-based research.13 23 24
Assessment of confounders
Self-reported confounding factors were sex, age, survey, socioeconomic status, long-standing illness and alcohol consumption. Study member occupation was coded according to the Registrar General classification for social class,25 a six-level indicator of socioeconomic status in which a lower score indicates greater prestige. Respondents reported if they suffered from a long-standing illness and their level of alcohol consumption (consumption at least five occasions per week was denoted as high). Long-standing illness was defined as ‘long-standing illness, disability or infirmity’ and the time period referred to was ‘anything that has troubled you over a period of time, or that is likely to affect you over a period of time’, with the response alternatives: no, yes or don’t know.
Ascertainment of cause of death
Cause of death was based on certification and coded according to the International Classification of Diseases (10th revision; ICD-10).26 We generated outcomes for mortality from all-causes, cardiovascular disease (ICD codes I01–I99) and all cancers combined (C00–D48). Based on existing evidence,27 28 we also denoted smoking-related cancers as C01–C16, C22, C25, C30.0, C31, C32, C34, C53, C64–C67, C68.0, C68.1, C68.8, C68.9 and C92. These cancers are shown to have an established relation with smoking and consist of cancers in the lung, stomach, pancreas, bladder, upper aerodigestive, kidney, myeloid leukaemia and liver.27 28
Statistical analyses
Altogether, 142 150 men and women were surveyed in 12 studies. Of these, 61 740 provided a salivary cotinine and 57 284 gave consent to use their data. After omitting self-reported smokers (n=12 862), participants with a cotinine value at or above 15 ng/mL (self-reported non-smokers with salivary cotinine ≥15.00 ng/mL were regarded as deceivers) (n=1 971),29 30 and those without complete covariate data (n=5867), 36 584 study members (19 792 women) remained. This was our analytical sample.
Having ascertained that the proportional hazards assumption had not been violated, we used Cox proportional hazards regression models31 to estimate HRs with 95% CIs to summarise the relationship between salivary cotinine level and risk of death. In these analyses, calendar time (months) was the time scale, with censoring taking place on date of death or end of mortality surveillance (15 February 2011 for HSE and 31 December 2009 for the SHS), whichever came first. As there was no effect modification of the cotinine–death relation by sex or age, we combined men, women and all ages in the analyses and adjusted for sex and age in addition to other covariates. We included survey year as fixed effects in the models. We entered two sets of covariates into the models: sex and age (comparator model); and sex, age, survey year, social class, frequency of alcohol use and long-standing illness. The mkspline procedure in STATA produced multivariable-adjusted spline curves for any death and deaths from cardiovascular disease, total cancer and smoking-related cancer. We carried out all analyses using Stata V.14.1.32
Results
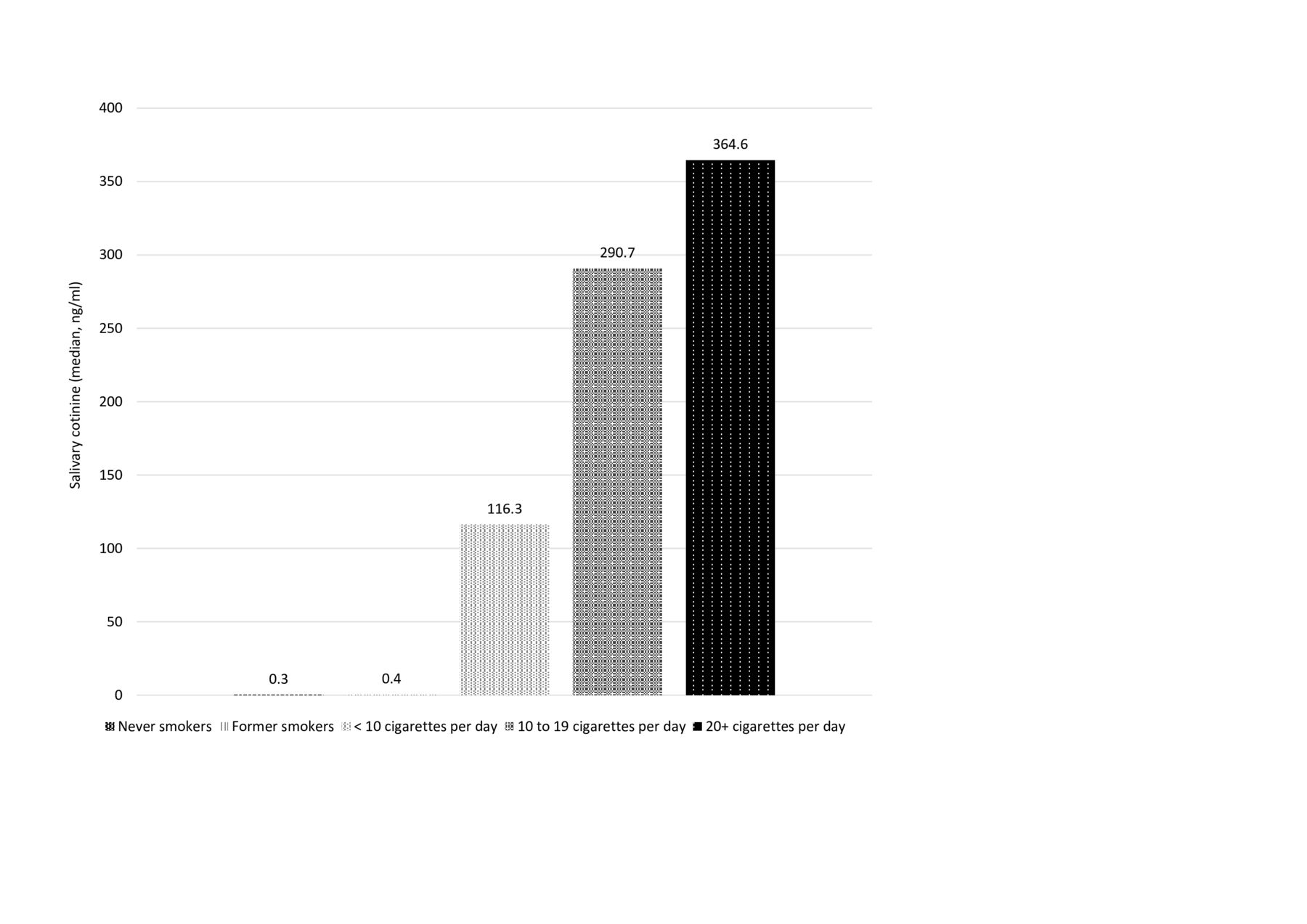
Age, sex, social status, self-reported illness and former smoking varied with cotinine level such that study members in the lowest cotinine tertile were older, and there was a lower proportion of men, manual workers and former smokers relative to the higher tertiles (table 1). Furthermore, higher proportions of participants in the lowest tertile reported long-standing illness than in the other groups. There was no difference in the prevalence of high alcohol intake according to cotinine categories. Salivary cotinine levels varied with study years, with lower levels after the smoking ban was implemented in UK in 2006 (results not shown). Cotinine levels varied substantially across smoking categories, with self-reported active smokers having the highest cotinine levels (see figure 1).
Baseline characteristics by salivary cotinine level in 36 584 non-smokers

Median salivary cotinine levels by self-reported smoking status. N=51 417.
The 36 584 non-smoking study participants were followed up for a mean of 8.1 years (range: 0.02–13.1 years) giving rise to 2365 deaths (out of which 775 deaths were from cardiovascular disease, 779 were from all cancers and 289 were from smoking-related cancers). In table 2, we show the relation of salivary cotinine with mortality risk. The highest level of cotinine was associated with elevated rates of death from all-causes (HR; 95% CI: 1.25; 1.14 to 1.38) cardiovascular disease (1.33; 1.13 to 1.58) and all cancers combined (1.20; 1.01 to 1.42), with the strongest effect apparent for smoking-related cancers (1.57; 1.19 to 2.06). There was some attenuation of risk after adjustment for multiple cofounding factors, although statistical significance at conventional levels was retained in most analyses. Mortality by continuous cotinine showed a similar pattern with elevated risk of death from any cause, cardiovascular disease, all cancers and smoking-related cancer. Additional analysis for total mortality adjusted for physical activity, blood pressure, mental health and self-assessed general health was carried out. However, these adjustments did not change the result.
HRs (95% CI) for the association between salivary cotinine and mortality in 36 584 non-smokers
Figure 2 shows the spline curves for death from all-causes, cardiovascular disease, all cancers combined and smoking-related cancers in which we illustrate thresholds of risk in relation to cotinine levels. The curves indicate that there is an increase in mortality from all causes, cancer and cardiovascular disease with increasing cotinine levels with a plateau at around 2 ng/mL such that no association seems to be present thereafter. For smoking-related cancer, this inflection is less apparent.

{kind=link}
{kind=link}
Deaths from any cause, cancer, cardiovascular disease (CVD) and smoking-related cancer by salivary cotinine level (ng/mL). Solid line represents HR, and dotted line represents 95% CIs.
Discussion
The main finding of the present analyses was that salivary cotinine, our biomarker of passive smoking, was associated with elevated rates of mortality from various causes, effects that was independent of selected confounding variables. The magnitude of these relationships was, as anticipated, lower than those apparent for active smoking (online supplemental file).
Supplemental material
Comparison with published studies
As discussed, few studies of mortality risk have used biomarker measurements to capture exposure to passive smoking. That different cotinine measures have been deployed—urine, saliva and blood10 12 33 34—complicates synthesis, although correlations among the passive smoking indicators is high. Weak and modest associations have been reported for cotinine indices in relation to total mortality12 33 34 and lung cancer,33 while associations between cotinine level and deaths from heart disease and cardiovascular disease vary.33–35 The shape of the cotinine–cardiovascular disease association in the current study suggests a threshold at low doses after which there is no distinct increase in mortality. This observation seems to accord with extant studies.12 33–35 The observed lower threshold in cancer mortality may indicate that low but detectable levels of cotinine are not carcinogenic. An explanation of the observed threshold for CVD and cancer mortality needs further investigation. By contrast, the relation between cotinine and cancers ascribed to passive smoking was incremental across the cotinine continuum.
Study strengths and limitations
A reliance on self-report of any characteristic may be problematic as interpretation may be hampered by socially desirable responses, and smoking is no exception.36 37 Our study has the advantage of having biological measurement of passive smoking, salivary cotinine, which correlates highly with cotinine in blood23 and may even offer higher sensitivity than cotinine from urine and serum.13 In addition, our study has an objective health outcome, that is, cause of death was based on certification and coded according to the ICD-10.26 However, while salivary cotinine may capture exposure in all contexts, it has a half-life of 20 h and will such only index recent passive smoking. There is also some individual variability in nicotine metabolism and elimination.10 23 24 These conditions might have caused some misclassification of smokers and non-smokers. That salivary cotinine levels correlated strongly with self-reported active smoking status such that there was a marked difference between smokers and non-smokers (figure 1) gives us confidence in our results for passive smoking.
There are some study limitations. Passive and active smoking were captured at a single point in time, and this may have resulted in some degree of misclassification of the study participants who changed habits during follow-up, during the more than decade-long period of baseline data collection (1997–2008), smoking prevalence and hence passive smoking decreased considerably.38 It is likely that this misclassification was not systematic with respect to the outcomes under study, and as such, we have underestimated the health risks of passive smoking, possibly more for cancers due to a longer lag between exposure and outcome. Residual confounding is a perennial limitation in observational analyses, and our study is no exception. Lastly, the use of cotinine, the most common biomarker of passive smoking, is not without its challenges. Other exposures that may influence cotinine level such as nicotine vapour from room surfaces, clothing and dust, some foods, smokeless tobacco products (snus) and nicotine replacement therapy were not captured in the present study and were not taken into account. However, we did exclude study members because their cotinine levels were too high for them to be realistically classified as non-smokers. It is possible that at least some of these people had used nicotine products other than cigarettes.
In conclusion, our study supports an association between objectively ascertained secondhand smoking and mortality from any death, cardiovascular disease and smoking-related cancers. The apparent threshold effects for some of these relationships require further exploration.
Data are available in a public, open access repository.39
What is already known on this subject
Passive smoking appears to be related to a range of chronic diseases.
With studies almost exclusively relying on self-reports of passive smoking, the magnitude of relationship may have been biased.
There are also very few prospective cohort studies in this context which, in the absence of clinical trials, provide the best evidence of a causal link.
What this study adds
In the present context, this multicohort study is the largest to date with data on a biomarker of passive smoking.
In non-smokers, salivary cotinine above a threshold of 0.5 ng/mL was associated with a 20%–40% higher rate of death from all-causes, cardiovascular disease and smoking-related cancers.
Data availability statement
Data are available in a public, open access repository. Data can be downloaded from the UK data archive (www.data-archive.ac.uk).
Ethics statements
Ethics approval
Ethical approval was provided by the London Research Ethics Council.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EK: conception and design of the work, acquisition and interpretation of data and drafting the work. AT: analysis and interpretation of data and revising the work critically for important intellectual content. GB: conception and design of the work, acquisition and interpretation of data and revising the work critically for important intellectual content. All authors have final approved this version of the work to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.