Article Text

Abstract
Background Previous studies, which examined the association between employment status and postpartum depression, were limited by binary or ternary employment status measures (employed/unemployed or full-time/part-time/unemployed). This study examined the association between detailed employment status during pregnancy and risk of depressive symptomatology 1 month after childbirth, and the effect modification by one’s perceived level of social support and household equivalent income.
Methods Our study examined 76 822 participants in the Japan Environment and Children’s Study. The exposure included maternal employment status during pregnancy (regular workers, dispatched workers, part-time workers, self-employed workers, non-employed and others), and the outcome was depressive symptomatology 1 month after childbirth: Edinburgh Postnatal Depression Scale (EPDS scores ≥9 and ≥13). Adjusted ORs and 95% CIs of depressive symptomatology associated with employment status were calculated by multivariable logistic regression. Subgroup analyses by perceived level of social support and household equivalent income were conducted.
Results Compared with regular workers, the risk of depressive symptomatology (EPDS score ≥9) was higher for non-employed and others, and that (EPDS score ≥13) was so for part-time workers. There was no significant interaction by perceived level of social support and household equivalent income in the associations. However, part-time workers and non-employed had excess risk of depressive symptomatology among women with lower perceived level of social support, but not among those with the higher one.
Conclusion Compared with regular workers, part-time workers and non-employed had an increased risk of depressive symptomatology, which was confined to women with lower perceived level of social support.
- employment
- maternal health
- social epidemiology
Data availability statement
No data are available. Data are unsuitable for public deposition due to ethical restrictions and legal framework of Japan. It is prohibited by the Act on the Protection of Personal Information (Act No 57 of 30 May 2003, amendment on 9 September 2015) to publicly deposit the data containing personal information. Ethical Guidelines for Epidemiological Research enforced by the Japan Ministry of Education, Culture, Sports, Science and Technology, and the Ministry of Health, Labour and Welfare also restrict the open sharing of the epidemiological data. All inquiries about access to data should be sent to: jecs-en@nies.go.jp. The person responsible for handling enquiries sent to this email address is Dr Shoji F Nakayama, JECS Programme Office, National Institute for Environmental Studies.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Postpartum depression (PPD) is a major complication associated with childbirth, as worldwide approximately 17% of new mothers have experienced PPD1. In Japan, about 9% of new mothers have depressive symptomatology after childbirth.2 PPD may result in serious negative health impacts on both mothers and infants. For mothers, PPD is associated with decreased quality of life,3 difficulty in appropriately responding to their infants4 and poor mother–infant bonding.5 For infants, PPD was associated with disruption of sleeping and eating patterns,6 and delay of socioemotional and cognitive development.7 8
Maternal employment during pregnancy has been suggested as one of the protective factors for PPD.9–11 A prospective cohort study in Switzerland revealed that women who were unemployed during pregnancy had an increased risk of PPD compared with women who were employed.9 Furthermore, a nested case–control study in Switzerland10 and a small prospective cohort study in Japan11 revealed that women who were employed full-time during pregnancy had a lower risk of PPD compared with unemployed women. However, these previous studies were limited by binary or ternary employment status measures (employed/unemployed or full-time/part-time/unemployed), and failed to provide more detailed information pertaining to employment status.
It is assumed that the risk of PPD may vary based on one’s detailed employment status (eg, regular workers, dispatched workers, part-time workers, self-employed workers and non-employed), as each status may be accompanied by different lifestyles and levels of mental stress for pregnant women.
In Japan, there has been the gender division of labour: men go to work and women stay at home. However, the percentage of double-income households has been increasing from 47.9% in 1990 to 67.0% in 2019.12 In addition, more than half of working mothers are non-regular employees (ie, part-time, temporally or contract worker) in 2019.12 Because Japanese women are still expected to work for housework and childcare, this situation may cast adverse impact on a work and family balance and women’s mental health.
Poor social support has been reported to be one of the risk factors for PPD.13 Social support can be described as the emotional, material and informational support provided by family, relatives, friends, coworkers, neighbours and so on.14 High social support provides individuals with self-esteem and self-efficacy, thereby enables them to combat negative emotions such as depression.14 15 In Japan, the percentages of nuclear families who have children under 18 years old were 69.6% in 1986 and 82.7% in 2017.12 In addition, the percentage of people who answered ‘I have a good relationship with neighbours’ has decreased both in urban and rural areas: 39.1% (1986) to 15.0% (2011) and 64.2% to 23.8%, respectively.15
Low household income also has been reported one of the risk factors for PPD probably due to increased mental stress and anxiety.13 Married women are likely to work outside in order to supplement their family income16 so that household income may affect mother’s employment status.
To our best knowledge, no study has examined the association between detailed employment status during pregnancy and risk of PPD or depressive symptomatology after childbirth. The main purpose of this study is to examine the association between detailed maternal employment status during pregnancy and risk of depressive symptomatology 1 month after childbirth. We hypothesised that the risk of depressive symptomatology was higher for non-regular workers (eg, dispatched workers and part-time workers) and non-employed compared with regular workers. Additionally, the association between employment status and risk of depressive symptomatology is more evident among women with lower perceived level of social support and lower household income than those with higher.
Methods
Study cohort
Data from the Japan Environment and Children’s Study (JECS) were used in the current study. The JECS is a birth cohort study that followed children from birth to the age of 13. For the JECS, 15 survey regions were selected: Hokkaido, Miyagi, Fukushima, Chiba, Kanagawa, Koshin, Toyama, Aichi, Kyoto, Osaka, Hyogo, Tottori, Kochi, Fukuoka and South Kyushu/Okinawa. The participants were recruited based on the following inclusion criteria: (1) expected delivery date between 1 August 2011 and mid-2014; (2) resident of the study area at the time of recruitment; and (3) capable of comprehending the Japanese language and completing the self-administered questionnaire. Details of the JECS protocol have been described elsewhere.17 18
For the JECS, self-administered questionnaires were distributed to all participants at the timing of registration for the JECS, the second or third trimester of their pregnancy and 1 month after delivery. The questionnaires collected information including mother’s mental health, socioeconomic status, obstetric history and lifestyle factors. The first questionnaire survey was conducted on registration for the JECS (T1). The second questionnaire survey was distributed during the second or third trimester (T2) of their pregnancy. A third questionnaire survey was conducted 1 month after delivery.
Study population
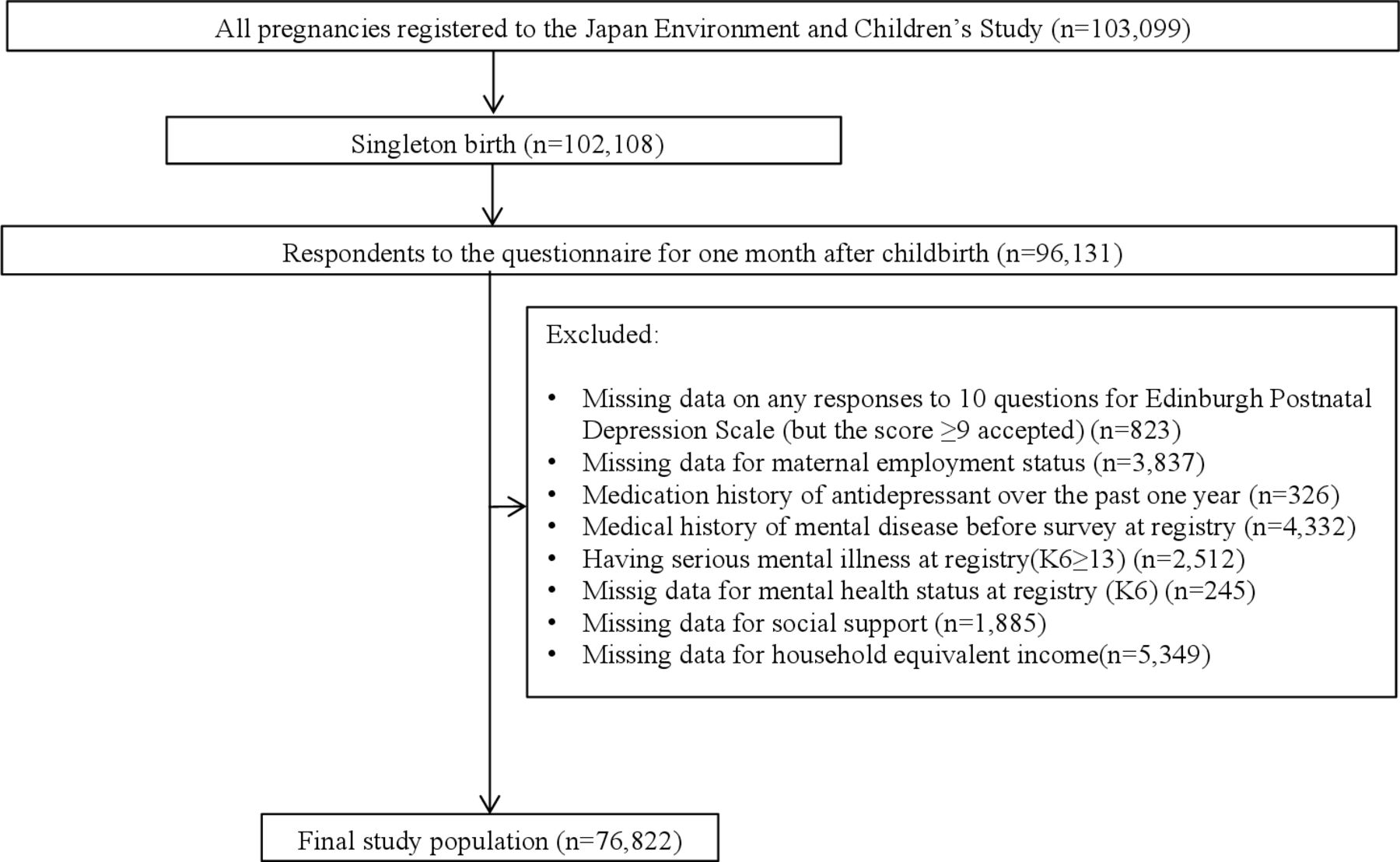
The present study used the dataset jecs-ag-20160424, which was released in June 2016 and revised in October 2016. Among the 103 099 pregnancies registered with the JECS, singleton birth (n=1 02 108) and participants who completed the questionnaire provided 1 month after childbirth (n=96 131 response rate: 94.1%) were included. Additionally, the following cases were excluded: missing data for Edinburgh Postnatal Depression Scale (EPDS) (but the score ≥9 accepted) (n=823); missing data for employment status (n=3837); having a history of using antidepressant medication over the past year (n=326); having a self-reported lifetime medical history of depression, anxiety disorder or schizophrenia prior to the T1 survey (n=4332); having serious mental illness (Kessler Psychological Distress Scale (K6) score ≥13) at the time of the T1 survey (n=2512); missing data for mental health status (K6) at the T1 survey (n=245); missing data for social support (n=1885) and missing data for household equivalent income (n=5349). The final population of this study was 76 822 (figure 1).
{kind=link}
Flow chart for study population. K6, Kessler Psychological Distress Scale.
Measurements
Major predictor: employment status
The major predictor was employment status during pregnancy. For the T1 questionnaire, participants were asked, ‘Which is your employment status now?’ The choices of the answer were the following: ‘regular worker’, ‘self-employed worker’, ‘dispatched worker’, ‘housewife’, ‘part-time worker’, ‘jobless’ and ‘others’. ‘Dispatched worker’ means employees who sign an employment contract with not their workplace but with a temporary employment agency, and are dispatched from the agency to their workplace. Because women who were ‘housewife’ (n=29 664) and ‘jobless’ (n=1048) were likely to be mixed up by respondents, we combined them into ‘non-employed’. Finally, the employment status was classified into six groups: regular workers, dispatched workers, part-time workers, self-employed workers, non-employed and others.
Outcome: depressive symptomatology
Depressive symptomatology 1 month after childbirth was assessed using the Edinburgh Postnatal Depression Scale (EPDS). The EPDS is a 10-item self-reported scale, and each item is scored from 0 to 3; the total score ranges from 0 to 30. The EPDS is a symptom screen and the first step in a necessary two-stage clinical process of determining the medical diagnosis of PPD. Because we relied on EPDS only, we called ‘depressive symptomatology’ for the outcome of this study. The questionnaire distributed 1 month after childbirth included the Japanese version of the EPDS. Reliability and validity of Japanese version of EPDS at 1 month after childbirth have been verified.19 The Cronbach’s α of EPDS in our study was 0.61.
In this study, we evaluated depressive symptomatology using two cut-off points, EPDS score ≥9 as well as EPDS score ≥13 because the cut-off of ≥9 has been recommended as the Japanese version of EPDS.19 The sensitivity, specificity, positive predictive value and negative predictive value for Japanese version of EPDS score ≥9 were 0.75, 0.93, 0.50 and 0.98, respectively.19
The cut-off of ≥13 has been recommended as the original English version of EPDS, and the corresponding statistics for the English version of EPDS score ≥13 against diagnosis of depressive symptomatology were 0.73, 0.97, 0.50 and 0.99.20
Covariates
The following were selected as confounding factors: age (min 15, max 49), educational attainment (high school or less/vocational school/junior college/more than university or higher), household equivalent income (quartile), parity (yes or no), living with partner (yes or no), living with parents (yes or no), marital status (married, unmarried, divorce or bereavement), mental health status (K6 score: min 0, max 12), perceived level of social support (social support score: min 0, max 14) and residential area (15 survey regions).
Age was collected from medical records at the time of delivery. We obtained data pertaining to parity, living with partner, living with parents, marital status and mental health status (K6) from the T1 questionnaire. The Japanese version of K6 was validated; the performance of Japanese version in detecting Diagnostic and Statistical Manual of Mental Disorders, fourth edition mood and anxiety disorders, as assessed by the areas under receiver operating characteristic curves, was as high as 0.94 (95% CI=0.88 to 0.99).21 The Cronbach’s α of K6 in our study was 0.76. Information on education attainment, household income and perceived level of social support was gathered by the T2 questionnaire. Household equivalent income is the household income divided by the square root of the number of household members. Questions pertaining to perceived level of social support included: (1) ‘Is there someone available to you who shows you love and affection?’, (2) ‘Is there someone whom you can count on to provide you with emotional support (talking over problems or helping you make a difficult decision)?’, (3) ‘How often do you have as much contact as you would like with someone you feel close to: someone in whom you can trust and confide?’, and (4) ‘Number of friends/neighbours to whom you can talk casually about your concern?’. Questions 1–4 were modified from the Social Support Questionnaire (SSQ)22; questions 1, 2 and 3 were answered using a 5-point scale (0: not always, 1: sometimes, 2: certain extent, 3: almost always, 4: always); and question 4 was answered using a 3-point scale (0: none, 1: one or two people, 2: more than three people). The Cronbach’s standardised α of the social support measurement of the present study was 0.74. Then, we calculated the total score ranging from 0 to 14.
Statistical analysis
We calculated the proportion of all confounding variables according to employment status; we compared these using Χ2 tests. Then, we performed multivariable logistic regression analysis to estimate the adjusted ORs and 95% CIs of depressive symptomatology according to employment status. The outcome, depressive symptomatology, was assessed by the two cut-off points: EPDS score ≥9 and EPDS score ≥13. We adjusted for the potential confounding variables. We categorised the missing covariates as dummy variables and included in the model of multiple logistic regression analyses. Further, we conducted the stratified analyses by perceived level of social support and household equivalent income split by the median. We estimated multivariable ORs and 95% CIs for each group and each version of cut-off points, EPDS score ≥9 and EPDS score ≥13. Then, we tested statistical interactions using cross-product terms for employment status with perceived level of social support and household equivalent income. All statistical analyses were carried out using the SAS 9.4.
Results
Table 1 shows proportions of depressive symptomatology and all confounding and stratification variables according to maternal employment status. In total, 6741 (8.8%) mothers and 1167 (1.5%) mothers developed one when we used the cut-off point for EPDS score ≥9 and ≥13, respectively. The average age was 31.3 years old. The percentages of employment status were 35.4% for regular workers, 1.8% for dispatched workers, 20.8% for part-time workers, 3.2% for self-employed workers, 36.3% for non-employed and 2.5% for others. Women who were regular workers have higher educational attainment and higher income than those with other employment status.
Demographic and socioeconomic characteristic of study population according to maternal employment status
Table 2 shows age-adjusted and multivariable ORs and 95% CIs of depressive symptomatology according to maternal employment status. Compared with regular workers, the risk of depressive symptomatology (EPDS score ≥9) was higher for non-employed (OR=1.11, 95% CI 1.03 to 1.19, p=0.004) and others (OR=1.20, 95% CI 1.01 to 1.41, p=0.034), and that (EPDS score ≥13) was higher for part-time workers (OR=1.19, 95% CI 1.003 to 1.42, p=0.046).
Age-adjusted and multivariable ORs and 95% CIs of depressive symptomatology 1 month after childbirth according to maternal employment status
Table 3 shows the subgroup analysis results stratified by lower and higher perceived level of social support. Confounding variables according to maternal employment status, stratified by perceived level of social support are shown in online supplemental table 1. There was no statistically significant interaction by perceived level of social support in the association between employment status and risk of depressive symptomatology. However, among women with lower perceived level of social support, the risk of depressive symptomatology (both EPDS scores ≥9 and ≥13) was higher for part-time workers (OR=1.10, 95% CI 1.01 to 1.21, p=0.036 and OR=1.24, 95% CI 1.02 to 1.52, p=0.031, respectively) and non-employed (OR=1.14, 95% CI 1.05 to 1.24, p=0.002 and OR=1.22, 95% CI 1.02 to 1.46, p=0.032, respectively) compared with regular workers. However, such associations were not observed among those with higher perceived level of social support.
Supplemental material
Age-adjusted and multivariable ORs and 95% CIs of depressive symptomatology 1 month after childbirth according to maternal employment status, stratified by perceived level of social support
Table 4 shows the subgroup analysis results, stratified by lower and higher household equivalent income. Confounding variables according to maternal employment status, stratified by household equivalent income are shown in online supplemental table 2. Household equivalent income did not modify the association between employment status and risk of depressive symptomatology. However, the risk of depressive symptomatology (EPDS score ≥13) was higher for dispatched workers (OR=1.82, 95% CI 1.02 to 3.26, p=0.043) and part-time workers (OR=1.39, 95% CI 1.06 to 1.83,p=0.018) compared with regular workers among women with higher household equivalent income. Such associations were not observed among those with lower household equivalent income except for non-employed who showed similar excess risk of depressive symptomatology in both income groups.
Age-adjusted and multivariable ORs and 95% CIs of depressive symptomatology 1 month after childbirth according to maternal employment status, stratified by household equivalent income
Discussion
In this large birth cohort study of 76 822 pregnant women, 6741 (8.8%) mothers and 1167 (1.5%) mothers developed depressive symptomatology 1 month after childbirth when we used the cut-off points for EPDS scores ≥9 and ≥13, respectively. Compared with regular workers, the risk of depressive symptomatology (EPDS score ≥9) was higher for non-employed and others, and that (EPDS score ≥13) was so for part-time workers. We found no statistically significant interaction by perceived level of social support and household equivalent income in the association between employment status and risk of developed depressive symptomatology. However, as we hypothesised a priori, the association of part-time workers and non-employed with risk of depressive symptomatology was evident among women with lower perceived level of social support, but not among with the higher one.
The mechanisms by which part-time workers, non-employed and others increase the risk of depressive symptomatology are unclear. There are several potential factors through which part-time work can raise depressive symptomatology, such as job insecurity,23 work strain and exposure to hazardous work conditions.24 Non-employed would lead to lowering of economic safety, social status, social support and self-esteem which represent potential sources of mental stress.25 Several previous studies reported that housewives or women who were not working during pregnancy had higher risks of mental stress and anxiety than those who were working during pregnancy.26 27 Stress-induced activation of the hypothalamic–pituitary–adrenal (HPA) axis has been implicated in PPD,28 29 though increased levels of stress hormones including corticotropin releasing hormone,30 31 adrenocorticotropic hormone30 and cortisol.32
Social support is suggested as a protective factor for PPD through the suppressed activation of the HPA axis.33 34 An observational study of 82 pregnant women in Canada reported that women who received inadequate social support (emotional, informational and task support by their partner) had the higher salivary cortisol concentrations in response to psychological distress, than those who received effective social support.33 A placebo-controlled study of 37 German men reported that participants who received social support (bring their friends to the experimental session) exhibited the lower salivary cortisol concentrations during stress exposure (5 min of public speaking task and mental arithmetic performed in front of an audience) than those without social support.34
Unlike our a priori hypothesis, we found dispatched workers and part-time workers had higher risk of depressive symptomatology compared with regular workers among women with higher household equivalent income when we used the cut-off point for EPDS score ≥13. The reasons for this unexpected result are unclear. One of the possible reasons is that self-reported income was generally less reliable: some persons may report the higher income than the real one, and vice versa. As for another reason, these subgroups may seek an extra household income by dispatched and part-time working probably because they needed more money to make a living. The shortage of their income and a lack of control for household finances and the associated decision might lead to depressive symptomatology. Furthermore, dispatched and part-time workers with higher household income had higher educational attainment than corresponding workers with lower household income as shown in online supplemental table 2. Persons who were highly educated but earned low income status inconsistency had a higher risk of psychological distress and anxiety disorders.35
The strength of the present study is the use of a large-scale prospective birth cohort study in Japan, and the characteristics of the study participants were comparable to those collected in the national survey.18 We collected a wide range of information through questionnaires and medical records, which enabled us to control for various potential confounders. However, there are some limitations of this study. First, the outcome measurement, the EPDS, is self-reported and we did not have the data of physician’s diagnosis for PPD. Despite this, the EPDS for Japanese version was well validated and has been commonly used in research.19 Therefore, the impact of measurement error is expected to be small. Second, our social support measurement was adapted from the SSQ, and has not been verified.22 However, the Cronbach’s standardised α of the social support measurement of the present study was 0.74, which revealed acceptable internal consistency. Third, there was a lack of demographic information for those who did not participate in the present study; thus, the potential impact of selection bias could not be examined. However, the characteristics of the participants of the JECS (eg, age at delivery, parity and gestational age at birth) were similar to those obtained from the 2013 Japan’s Vital Statistics Survey.18 Therefore, the impact of this bias is expected to be small.
In conclusion, our findings indicate that part-time workers and non-employed had increased risk of depressive symptomatology which was confined to women with lower perceived level of social support. Additionally, dispatched workers and part-time workers had increased risk of depressive symptomatology among women with higher household income. Our findings may be informative for health professionals to identify women at high risk of depressive symptomatology after childbirth.
What is already known on this subject
Previous studies have examined the association between employment status during pregnancy and risk of postpartum depression, and reported that unemployment was associated with the increased risk.
No study has examined the association between detailed categorised employment status (regular workers, dispatched workers, part-time workers, self-employed workers, non-employed, others) and risk of postpartum depression, or depressive symptomatology also examined effect modification by social support and household income.
What this study adds
Compared with regular workers, the risk of depressive symptomatology (Edinburgh Postnatal Depression Scale/EPDS score ≥9) was higher for non-employed and others, and that (EPDS score ≥13) was so for part-time workers.
Part-time workers and non-employed had excess risk of depressive symptomatology (both EPDS scores ≥9 and ≥13) among women with lower perceived level of social support, but not among with the higher one.
Dispatched workers and part-time workers had excess risk of depressive symptomatology (EPDS score ≥13) among women with higher household income, but not among with the lower one.
Data availability statement
No data are available. Data are unsuitable for public deposition due to ethical restrictions and legal framework of Japan. It is prohibited by the Act on the Protection of Personal Information (Act No 57 of 30 May 2003, amendment on 9 September 2015) to publicly deposit the data containing personal information. Ethical Guidelines for Epidemiological Research enforced by the Japan Ministry of Education, Culture, Sports, Science and Technology, and the Ministry of Health, Labour and Welfare also restrict the open sharing of the epidemiological data. All inquiries about access to data should be sent to: jecs-en@nies.go.jp. The person responsible for handling enquiries sent to this email address is Dr Shoji F Nakayama, JECS Programme Office, National Institute for Environmental Studies.
Ethics statements
Patient consent for publication
Ethics approval
Written informed consent was obtained from all participating women. The JECS protocol received approval from the Ministry of the Environment’s Institutional Review Board on epidemiological studies and the Ethics Committees of all participating institutions. The JECS was conducted in accordance with the Helsinki Declaration and other nationally valid regulations and guidelines.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Collaborators The chief members of the Japan Environment and Children’s Study (JECS) as of 2019 are Michihiro Kamijima (principal investigator, Nagoya City University, Nagoya, Japan), Shin Yamazaki (National Institute for Environmental Studies, Tsukuba, Japan), Yukihiro Ohya (National Center for Child Health and Development, Tokyo, Japan), Reiko Kishi (Hokkaido University, Sapporo, Japan), Nobuo Yaegashi (Tohoku University, Sendai, Japan), Koichi Hashimoto (Fukushima Medical University, Fukushima, Japan), Chisato Mori (Chiba University, Chiba, Japan), Shuichi Ito (Yokohama City University, Yokohama, Japan), Zentaro Yamagata (University of Yamanashi, Chuo, Japan), Hidekuni Inadera (University of Toyama, Toyama, Japan), Takeo Nakayama (Kyoto University, Kyoto, Japan), Hiroyasu Iso (Osaka University, Suita, Japan), Masayuki Shima (Hyogo College of Medicine, Nishinomiya, Japan), Youichi Kurozawa (Tottori University, Yonago, Japan), Narufumi Suganuma (Kochi University, Nankoku, Japan), Koichi Kusuhara (University of Occupational and Environmental Health, Kitakyushu, Japan), and Takahiko Katoh (Kumamoto University, Kumamoto, Japan).
Contributors YA designed the study, performed the statistical analysis and drafted the manuscript. KH conceived the study and helped to draft the manuscript. TK helped to make the statistical analysis. SI conducted the data collection and helped to draft the manuscript. HI supervised the study and made critical revision of the article. All authors read and approved the final manuscript.
Funding The Japan Environment and Children’s Study was funded by the Ministry of the Environment, Japan.
Disclaimer The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the above government agency.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.