Article Text

Abstract
Aim This study summarised available evidence on the association between early and on-time retirement, compared with continued working, and mortality. Moreover, this study investigated whether and to what extent gender, adjustment for demographics and prior health status influence this association.
Methods A systematic literature search of longitudinal studies was conducted. A qualitative analysis of the included studies was performed, followed by a meta-regression analysis to assess the influence of gender, prior health and demographics. Random-effects models were used in a meta-analysis to estimate the pooled effects for relevant subgroups identified in the meta-regression.
Results In total, 25 studies were included. Adjustment for prior health and demographics influenced the association between retirement and mortality (p<0.05). The results of the meta-analysis of 12 studies are presented for ‘insufficiently adjusted’ and ‘fully adjusted’ subgroups. There was no association between early retirement and mortality compared with working until retirement (fully adjusted subgroup: HR 1.05, 95% CI 0.87 to 1.28). On-time retirement was associated with a higher risk of mortality compared with working beyond retirement (insufficiently adjusted subgroup: HR 1.56, 95% CI 1.41 to 1.73). However, in the subgroup that adjusted for prior health, on-time retirement was not associated with mortality (HR 1.12, 95% CI 0.98 to 1.28).
Conclusion Early retirement was not associated with a higher risk of mortality. On-time retirement was associated with a higher risk of mortality, which might reflect the healthy worker effect. It is important to consider information on prior health and demographics when studying the association between retirement and mortality to avoid biased findings.
- health inequalities
- mortality
- occupational health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
In many countries, the population is ageing due to increasing life expectancy and decreasing birth rates.1 2 To minimise the growing proportion of retirees compared with the active working population, many governments have raised the statutory retirement age and have linked retirement age to life expectancy.3 4 In most European countries, the statutory retirement age has gradually increased from 65 years in 2012 to 67 or 69 years in 2022.5–7 Of particular concern, however, is whether and to what extent an increasing retirement age may affect the health of older people after retirement.
In recent years, there has been a growing interest in studying the impact of work and retirement on health.8–16 In general, working is beneficial for well-being and health.17–22 This is also illustrated by previous systematic reviews showing that a transition from work to retirement may lead to increasing general and physical health problems.8 9 However, retirement can also result in improvements in mental health.8 9 The conflicting results may be explained by the type and age of retirement, that is, whether early (eg, before 63 years in Finland, and before 65 or 60 years for men and women, respectively, in Austria) or on time (eg, between 63 and 67 years in Finland, and at 65 or 60 years for men and women, respectively, in Austria). For example, previous studies in Finland and the UK have shown that physical and mental health improve after early retirement,23 24 whereas a study in the USA found a decline in physical health after on-time retirement compared with working beyond retirement.25 These conflicting results are mostly from studies of subjective health outcomes and may represent rather acute effects of retirement. Therefore, it is more useful to examine the long-term association between retirement and health, and stratify the analysis by type of retirement (early and on-time retirement).
There are two prevailing beliefs when it comes to the association between retirement and mortality. The first belief is that people who retire (early) may live longer than those who continue working, since retirement may serve as a release from the adverse effects of work demands.26 27 The other belief is that those who retire (early) die sooner, since retirees no longer experience the beneficial health effects of work, and/or workers in poor health retire earlier than workers in good health.28 29 These different explanations are evident in a previous systematic review that found mixed evidence on the effects of on-time and early retirement as risk factors for mortality when analysed separately.30 More recently, several studies have assessed the impact of retirement age on mortality, but they have also had mixed findings.31–46 A summary of available evidence on this topic and an analysis of whether and to what extent prior health status influences the association between retirement and mortality would help to clarify the situation. In addition, possible gender differences in this context are important to consider since in some countries women have a lower retirement age, and women live longer than men in general worldwide.47
Therefore, the main objective of this study was to summarise available evidence from longitudinal studies on the association between early and on-time retirement, compared with continued work participation, and mortality. Moreover, this study investigated whether and to what extent gender, adjustment for demographics and prior health status influence the association between retirement and mortality.
Methods
A systematic review, meta-regression analysis and meta-analysis were conducted to explore the association between retirement (early and on-time) and mortality. The protocol for the current study was registered in PROSPERO (International Prospective Register of Systematic Reviews) a priori.48 The current study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.49
Search strategy and selection criteria
A literature search was conducted in March 2018 in the following databases: PubMed, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, the International Bibliography of the Social Sciences (IBSS), ABI/Inform, Business Source Elite and EconPapers. The search terms were retirement, pension, early pension, mortality, survival and longevity. We searched for longitudinal studies (both retrospective and prospective) that compared either early retirement and working until retirement, or on-time retirement and working beyond retirement. Studies that assessed the impact of work disability pension on mortality were excluded since health is inherent to this exit route.23 24 Studies were included if they used all-cause or cause-specific mortality as an outcome. Only studies written in English and published in peer-reviewed journals were selected.
Study selection
First, two reviewers independently screened 20% of the potentially relevant titles and abstracts for eligibility based on the inclusion and exclusion criteria. The remaining titles and abstracts were screened by one reviewer. Full-text articles were retrieved for further assessment of eligibility when (1) references appeared to be eligible based on title and abstract, (2) consensus could not be reached, or (3) there was no abstract available. Screening of full-text articles was performed by two reviewers. Discrepancies were discussed until consensus was reached. Finally, the reference lists of the included studies were checked for other potentially relevant studies.
Data extraction
One reviewer extracted data from all selected studies, and these data were checked by a second reviewer. The following information was extracted: first author, study design, data set used, country, description of pension system, study period, years of follow-up, sample size, characteristics of study population and confounders. Information on the effect estimate (adjusted for confounders) and variance or SE of the effect estimate (calculated from the CI or p value) was extracted for the meta-regression and subsequent meta-analysis. For studies with missing information, the corresponding author was contacted to request the required data.
Quality assessment
For methodological quality assessment, nine criteria based on Hayden et al’s checklist50 were used (see table 1). Each item was scored as positive (+) or negative (−), whereby negative was seen as potential bias. One reviewer performed the quality assessment for all selected studies, and this assessment was checked by a second reviewer. A high-quality study was defined as a study with a positive score on at least 50% of the criteria in the checklist.
Checklist of methodological quality
Qualitative analysis
Results from the studies are presented in online supplementary table 1, with ‘+’ indicating higher risk of mortality, ‘−’ indicating lower risk of mortality or ‘0’ indicating no association.
Supplemental material
Summary measures
Studies with an effect measure (ie, risk ratio, OR or HR) were included in the meta-regression and meta-analysis. From these studies, effect sizes were used to estimate (if not already presented) an HR (including 95% CI) for mortality. For studies that investigated the influence of an older age at retirement on mortality (without specifying the type of retirement or the comparison group), the inverse of the effect estimate was calculated to determine the influence of ‘retiring earlier’ compared with retiring later on mortality.
In the meta-regression, we determined whether and to what extent adjustment for prior health status, demographics and gender influenced the association between retirement and mortality. Demographics included age, gender (if applicable) and socioeconomic position (ie, education and/or income). To investigate whether and to what extent on-time retirement differed from retiring earlier, we also included retirement type in the meta-regression. In the meta-regression analysis, the pooled HRs were stratified by adjustment for these study characteristics. We used linear regression models to identify the influence of these study characteristics on the estimated risk of mortality (expressed in beta; significance p<0.05).
In the meta-analysis, the HRs were pooled using Review Manager V.5.3, and presented in forest plots by type of retirement (ie, early retirement, on-time retirement and retiring earlier), which was defined by the authors of the current study. Other subgroup analyses were presented in forest plots based on the results from the meta-regression analysis. Heterogeneity of the results was assessed using the I2 statistic. Since I2 was above 50% in most forest plots, random-effect models were applied for statistical pooling.
Results
Study selection
Figure 1 presents a flow diagram of the search, screening and selection process. The search strategy resulted in a total of 6919 records. After removing duplicates, 4099 unique records were screened by title and abstract. A total of 81 full-text publications were selected for further investigation. Finally, 22 studies met the inclusion criteria and 3 more studies were identified by reference list screening. Thus, a total of 25 studies were included in the current study.

Flow diagram.
Study characteristics
Online supplementary table 1 presents an overview of the characteristics of the included studies. Most studies were cohort studies, and a few studies used an instrumental variable approach to study the association between retirement and mortality. The follow-up periods in the included studies ranged from 2 to 31 years. Most studies were conducted in European countries (eg, Sweden, Denmark, the Netherlands, UK, Austria, Greece, Germany and Norway) and the USA. A few studies were conducted in Canada, Israel or Japan. The majority of the studies had a pension system with a statutory retirement age of 65 years and the possibility to retire early. Seventeen studies investigated the association between early retirement and mortality,26–29 31 37 38 40 41 45 46 51–56 while three studies investigated the association between on-time retirement and mortality.35 57 58 One study investigated the association between early retirement and mortality, as well as the association between on-time retirement and mortality.34 Four studies investigated the influence of a change in the retirement age or the influence of having a mandatory retirement rule at work compared with no mandatory retirement rule.44 59–61 A mandatory retirement rule implies that workers have to retire once they reach a certain age and are not allowed to prolong work participation.
Risk of bias
The outcome of the quality assessment is presented in figure 2. Two studies had a low risk of bias on all items. All other studies (n=23) had a high risk of bias; for example, some studies used a (early) retirement offer/window/reform as exposure, which is not the same as actual (early) retirement. Most studies had a high risk of bias for study confounding, that is, did not include prior health status or demographics as confounders in the analyses. However, all studies had high methodological quality and were included in the meta-analysis (studies with an estimated effect measure).
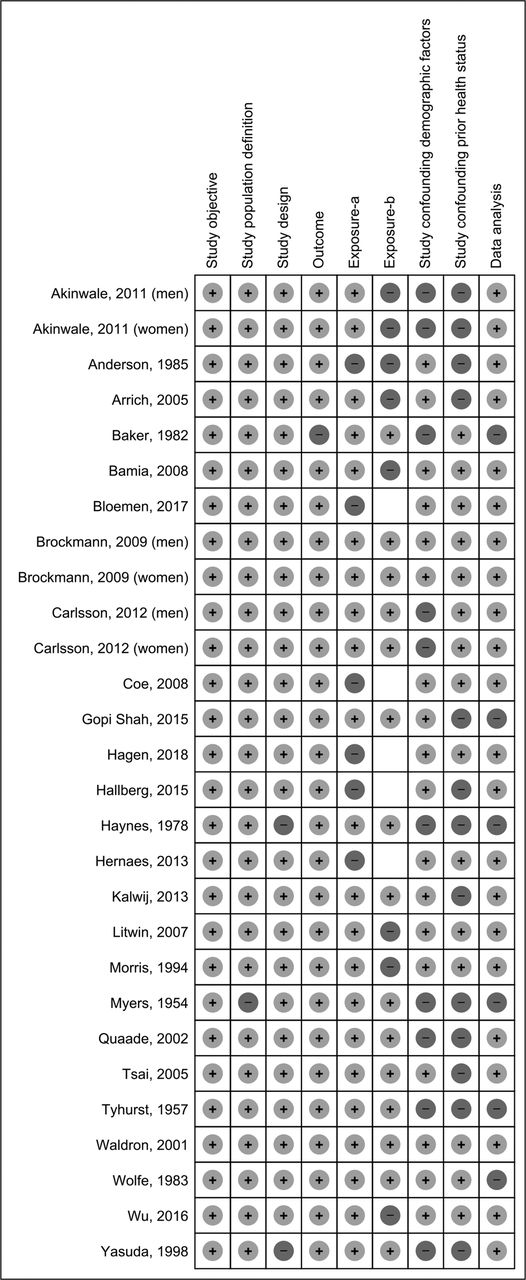
Risk of bias of included studies. The figure shows risk of bias (ie, + for low risk of bias, − for high risk of bias) for all criteria (ie, study objective, study population definition, study design, outcome, exposure, study confounding (demographics or prior health status) and data analysis).
Early retirement versus working until retirement
In the 18 studies that investigated the association between early retirement compared with continued work participation and mortality, a total of 20 associations were reported. Eight associations revealed a higher risk of mortality for early retirement, five associations pointed to a lower risk of mortality, and seven associations showed no association between early retirement and mortality (see online supplementary table 1).
In the meta-regression analysis, we found that the association between retirement and mortality was statistically weaker when adjusting for prior health status or demographics (table 2). No significant differences (p<0.05) in effect sizes were found between retirement type and gender. Therefore, in the meta-analysis, forest plots were calculated for the subgroup of studies adjusted for prior health status and demographics (ie, ‘fully adjusted subgroup’) and studies not adjusted for prior health status and/or demographics (ie, ‘insufficiently adjusted subgroup’).
Univariate meta-regression models with retirement, gender, adjustment for prior health status and adjustment for demographics modelled as independent variables and effect size (expressed in beta) as dependent variable
A total of seven studies with nine associations were used to estimate a pooled HR for early retirement and mortality (figure 3). The pooled HR for four associations in the insufficiently adjusted subgroup of studies showed no association between early retirement and mortality (HR 1.32, 95% CI 0.95 to 1.81). The pooled HR for five associations in the fully adjusted subgroup of studies was 1.05 (95% CI 0.87 to 1.28).

Effect sizes for studies investigating the association between early retirement compared with working until retirement and mortality. IV, inverse variance.
On-time retirement versus working beyond retirement
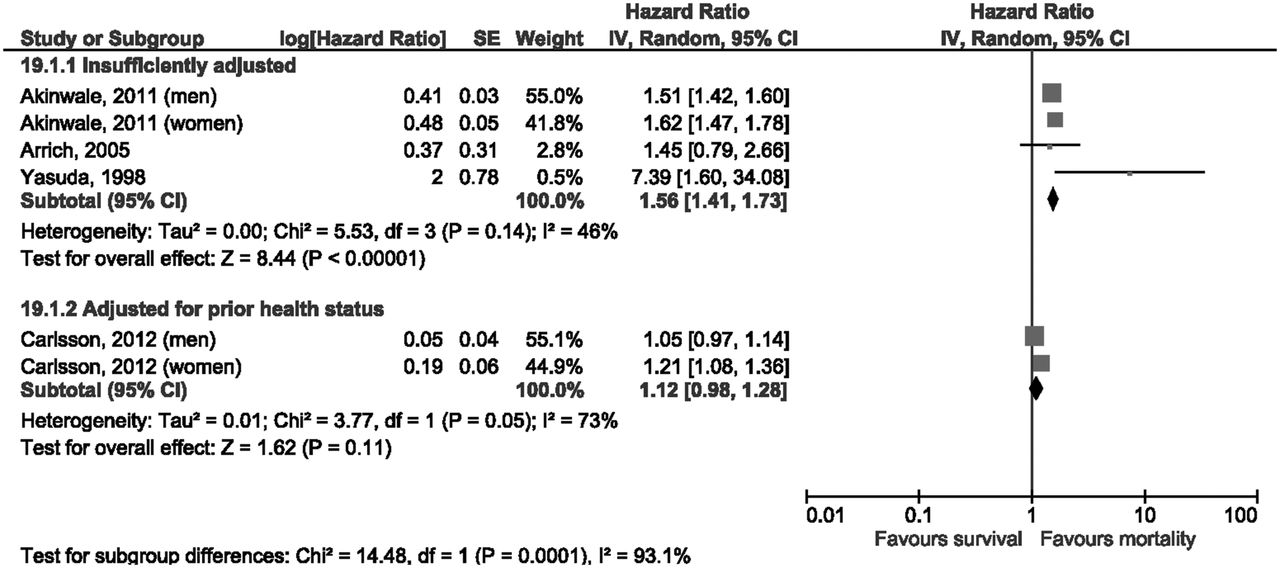
Four studies, with a total of six associations, investigated the association between on-time retirement and mortality. Four associations revealed a higher risk of mortality for on-time retirement, and two studies showed no association.
All studies with six associations were used to estimate a pooled HR (see figure 4). Three studies with four associations were classified as an insufficiently adjusted subgroup. One study (Arrich et al57) was based only on patients with stroke. The insufficiently adjusted subgroup of studies showed that on-time retirement was associated with a higher risk of mortality compared with working beyond retirement (HR 1.56, 95% CI 1.41 to 1.73). No study could be classified as fully adjusted group, but it was possible to classify two associations in a subgroup adjusted only for prior health status. The pooled HR for two associations adjusted for prior health status was 1.12 (95% CI 0.98 to 1.28).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect sizes for studies investigating the association between on-time retirement compared with working beyond retirement and mortality. IV, inverse variance.
Other comparisons
Three studies investigated the influence of retiring earlier on mortality without specifying retirement type or comparison group (online supplementary table 1). Two studies revealed a higher risk of mortality for retiring earlier, whereas one study showed no association. A pooled HR was estimated based on two associations and showed that retiring earlier resulted in higher mortality rates for the fully adjusted subgroup of studies (HR 1.12, 95% CI 1.09 to 1.16).
Discussion
In the current study, we showed that early retirement compared with working until retirement was not associated with mortality. We also showed that in the subgroup of studies that were insufficiently adjusted, on-time retirement was associated with a higher risk of mortality compared with working beyond retirement. However, in the subgroup of studies that adjusted for prior health, on-time retirement was not associated with mortality and the effect size was smaller than in the insufficiently adjusted subgroup of studies. Furthermore, we found that it is important to consider the influence of prior health status and demographics on the association between retirement and mortality to avoid biased findings.
One major finding was that there was no statistically significant association between early retirement (excluding work disability pension) and mortality. Similarly, in the qualitative analysis, the majority of studies (mostly in the field of economics) had no association between early retirement and mortality. This can perhaps be explained by a previous study that showed both poor health and good health can influence the decision to retire early.62 Older healthy workers may voluntarily decide to retire early to enjoy their life or fulfil other goals.62 63 However, there could also be a group of workers who are ‘forced’ to retire early, for example, because they have been fired at a relatively older age. A previous study in the Netherlands found that workers who preferred a later retirement actually retired much earlier than expected perhaps due to lack of choice.64 Such involuntary retirement can have more negative consequences on health than voluntary retirement.8 65 A previous systematic review found that an early exit from work has more adverse health effects among lower socioeconomic groups compared with higher socioeconomic groups.66 For example, people working in manual occupations could experience a different impact of (early) retirement on health than highly educated white-collar workers. We recommend further research to consider differences between socioeconomic groups and the actual voluntary nature of retirement.
The findings of the current study demonstrate that without adjustment for prior health status, on-time retirement appears to be associated with mortality. In the subgroup of studies that adjusted for prior health, on-time retirement was not associated with mortality. This finding may reflect a healthy worker effect, whereby healthy persons are more likely to work beyond retirement, and unhealthy persons are more likely to exit from the workforce.67–71 Unlike our result, a previous systematic review by Shim et al30 found mixed results on the association between on-time retirement and mortality, meaning that some included studies found no effect or a lower risk of mortality for those retiring on time. However, the authors included studies that used the general population as a reference group to examine this association, and it is well known that the general population has higher mortality rates compared with the working population, especially compared with those working beyond retirement.72 The difference in reference groups between the aforementioned systematic review and the current study could explain these conflicting results. This shows that it is important to carefully choose the reference group. The increased risk of mortality among those who retire on-time compared with those who work beyond retirement is most likely attributable to the healthy worker effect.
With regard to the role of gender, in the meta-regression analysis, we found no significant difference in effect size by gender. However, looking at some of the individual studies that did stratify by gender, different effect sizes for men and women were found.31 34 35 For example, Carlsson et al35 found that on-time retirement was associated with an increased risk of mortality for women, but not for men. The absence of a significant difference in the meta-regression analysis could be explained by the relatively small number of studies in the subgroup of studies among women (n=3). Since some countries are applying different statutory retirement ages for men and women, further studies are needed to elucidate the gender differences in the association between retirement and mortality.
A strength of the current study is that we summarised available evidence from longitudinal studies on the association between retirement and mortality. To our knowledge, this is the first study that combines the results of the literature by conducting a meta-analysis. Another strength is that we compared the results between studies that did and did not adjust for prior health status and demographics. By doing so, we were able to contribute to an important discussion in the literature: whether the timing of retirement is related to the risk of mortality, independent of prior health status. Moreover, we were able to investigate whether the association between retirement and mortality varied across study characteristics related to the adjustment for demographics, gender and retirement type.
This study also had limitations. First, the assessment of the full-text articles by two reviewers to identify discrepancies avoided false positives, but it did not address false negatives. Therefore, it is possible that relevant studies were missed. However, we minimised this risk by screening the reference lists of the included studies to identify other relevant studies. Second, since risk estimates differed among the included studies and not all data were available from all studies, we were unable to include all studies in the meta-regression analysis and meta-analysis (only 12 out of 25 included studies). This resulted in a relatively small number of studies in some subgroups. For example, in the meta-regression analysis where we tested whether retirement type influenced the association between retirement and mortality, we analysed four studies for on-time retirement, seven for early retirement and two for retiring earlier. In the meta-analysis, we presented the results for on-time retirement from four studies. If more studies in the meta-regression and meta-analysis would have been available, then we could have provided more certainty to our effect sizes. Third, one study (Arrich et al57) was based only on patients with stroke. However, this study contributed little weight to the pooled HR in the insufficiently adjusted subgroup of studies for on-time retirement and mortality. Fourth, we did not include studies that investigated the influence of a retirement reform or offer (eg, by exploiting a natural experiment) in the meta-regression analysis and meta-analysis since these studies used risk estimates that could not be pooled with the risk estimates of the included studies.
The findings of the current study have a number of implications and give direction to future research and policy. Since prior health status is an important factor in the association between retirement and mortality, in the context of an increasing retirement age, policymakers should consider health inequalities in the working population. Furthermore, we showed that there is an urgent need to consider information on demographics and prior health status in research on the association between retirement and mortality. Not adjusting for prior health status may lead to a biased conclusion that working longer results in living longer.
Conclusions
We did not find an association between early retirement, compared with continued work participation, and mortality. On-time retirement, compared with working beyond retirement, was associated with a higher risk of mortality. However, in the subgroup of studies that adjusted for prior health, we did not find an association between on-time retirement and mortality. Hence, when studying the association between retirement and mortality, it appears to be relevant to consider demographics as well as prior health status.
What is already known on this subject
In recent years, there has been a growing interest in studying the impact of work and retirement on health.
Several studies have assessed the impact of retirement age on mortality, but they have had mixed findings.
A summary of available evidence on this topic and an analysis of whether and to what extent prior health status influences the association between retirement and mortality would help to clarify the situation.
What this study adds
Early retirement was not associated with a higher risk of mortality.
On-time retirement was associated with a higher risk of mortality, which might reflect the healthy worker effect.
It is important to consider information on prior health and demographics when studying the association between retirement and mortality to avoid biased findings.
Since prior health status is an important factor in the association between retirement and mortality, in the context of an increasing retirement age, policymakers should consider health inequalities in the working population.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RS, AdW, SS, PC, IL, CB and AvdB contributed to the design of the paper. RS, AdW, IL and PC performed the literature search and data analysis. RS participated in drafting the article. AdW, SS, PC, IL, CB and AvdB revised the article critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.